
Editors: Morrey, Bernard F.
Title: Master Techniques in Orthopaedic Surgery: The Elbow, 2nd Edition
Copyright ©2002 Lippincott Williams & Wilkins
> Table of Contents > Part I – Elbow > 1 – Limited and Extensile Triceps Reflecting and Exposures of the Elbow
1
Limited and Extensile Triceps Reflecting and Exposures of the Elbow
Bernard F. Morrey M.D.1
1 Mayo Medical School and Department of Orthopaedics, Mayo Clinic and Mayo Foundation, Rochester, Minnesota.
Facility with exposures to the elbow characterized by
flexibility and extensibility is an essential prerequisite to the
execution of the full spectrum of elbow surgery while optimizing
function and minimizing complications. In this chapter I emphasize how
limited exposures to the elbow can be expanded to address broadened
pathology and perform more complex procedures. The review includes
three most important exposures from a conceptual standpoint: the
Kocher, Mayo, and medial extensile. Virtually all needed exposures can
be drawn from one of these three. Details are found in those chapters
addressing specific pathology. Although I do not favor and have
performed only one olecranon osteotomy for exposure, this technique is
relatively easy and commonly performed and hence is detailed in Chapter 4 and is further discussed in Chapter 6.
flexibility and extensibility is an essential prerequisite to the
execution of the full spectrum of elbow surgery while optimizing
function and minimizing complications. In this chapter I emphasize how
limited exposures to the elbow can be expanded to address broadened
pathology and perform more complex procedures. The review includes
three most important exposures from a conceptual standpoint: the
Kocher, Mayo, and medial extensile. Virtually all needed exposures can
be drawn from one of these three. Details are found in those chapters
addressing specific pathology. Although I do not favor and have
performed only one olecranon osteotomy for exposure, this technique is
relatively easy and commonly performed and hence is detailed in Chapter 4 and is further discussed in Chapter 6.
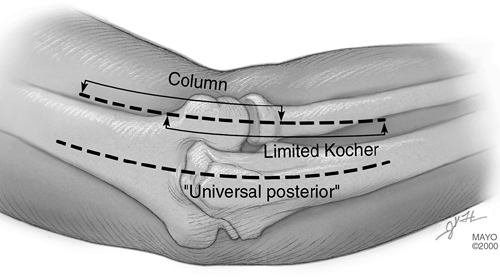
There are two conceptual incision types: an extensile posterior or limited, specific for purpose exposure (Fig. 1-1).
Both proximal and distal limited and focal procedures laterally have
been described. Distally, the skin incision is placed over Kocher’s
interval between the anconeus and the extensor carpi ulnaris and
brought proximally over the lateral epicondyle. Proximally, an incision
is placed over the lateral column and brought distally past the lateral
epicondyle.
Both proximal and distal limited and focal procedures laterally have
been described. Distally, the skin incision is placed over Kocher’s
interval between the anconeus and the extensor carpi ulnaris and
brought proximally over the lateral epicondyle. Proximally, an incision
is placed over the lateral column and brought distally past the lateral
epicondyle.
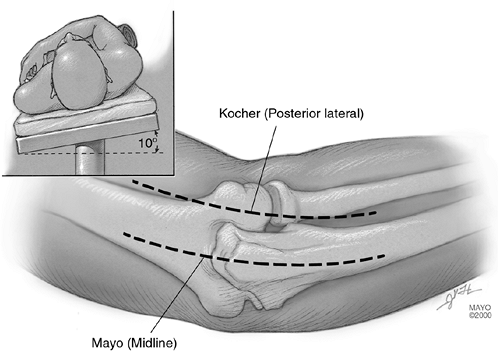
For extensile exposures, a straight posterior incision
is used. We term this the “universal” incision. For fear of injuring
the ulnar nerve, a posterior incision of variable length (12 to 18 cm)
is placed just medial or lateral to the tip of the olecranon and not
directly over the cubital tunnel. The most extensile exposure is
realized with this simple straight posterior skin incision, since both
medial and lateral aspects of the triceps mechanism and both collateral
ligaments can be exposed through it.
is used. We term this the “universal” incision. For fear of injuring
the ulnar nerve, a posterior incision of variable length (12 to 18 cm)
is placed just medial or lateral to the tip of the olecranon and not
directly over the cubital tunnel. The most extensile exposure is
realized with this simple straight posterior skin incision, since both
medial and lateral aspects of the triceps mechanism and both collateral
ligaments can be exposed through it.
 |
|
FIG. 1-1.
The straight posterior incision is considered “universal” as the entire joint can be exposed through this skin incision. Specific “for purpose” skin incisions such as for the “Column” or limited Kocher are frequently portions of a more extensive incision, such as the extensile Kocher incision. |
P.4
Limited: Lateral Surgical Exposures
The distal lateral approach is indicated in the case of
simple excision of the radial head. Landmarks include the lateral
epicondyle, radial head, palpate interval between anconeus and extensor
carpi ulnaris.
simple excision of the radial head. Landmarks include the lateral
epicondyle, radial head, palpate interval between anconeus and extensor
carpi ulnaris.
Surgery
The skin incision is made from the subcutaneous border
of the ulna obliquely across the posterolateral aspect of the elbow in
line with Kocher’s interval and ends at the lateral epicondyle (Fig. 1-2).
of the ulna obliquely across the posterolateral aspect of the elbow in
line with Kocher’s interval and ends at the lateral epicondyle (Fig. 1-2).
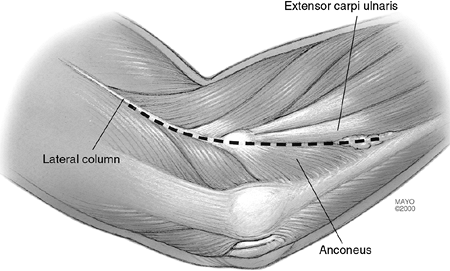
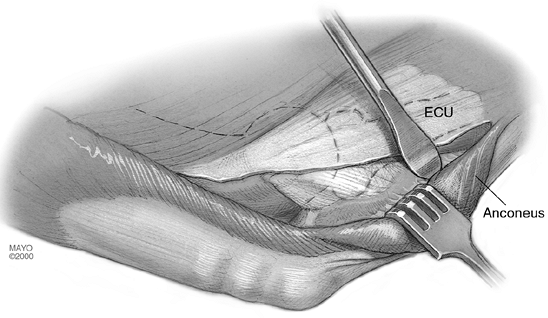
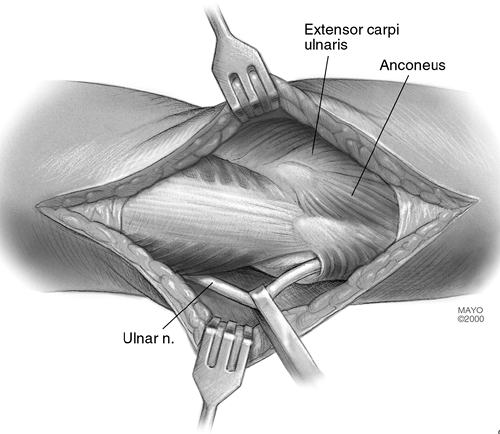
The interval between the anconeus and extensor carpi ulnaris is identified and entered (Fig. 1-3).
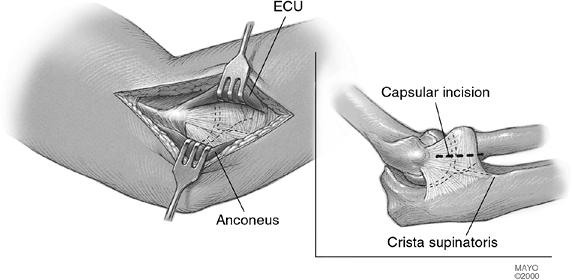
For excision of the radial head, the extensor carpi ulnaris and a small
portion of the supinator muscle are dissected free of the capsule and
retracted anteriorly (Fig. 1-4). The annular
ligament is then identified and entered. Care should be taken to enter
the annular ligament approximately 1 cm above the crista supinatoris to
avoid injury to the lateral ulnar collateral ligament (Fig. 1-4).
For excision of the radial head, the extensor carpi ulnaris and a small
portion of the supinator muscle are dissected free of the capsule and
retracted anteriorly (Fig. 1-4). The annular
ligament is then identified and entered. Care should be taken to enter
the annular ligament approximately 1 cm above the crista supinatoris to
avoid injury to the lateral ulnar collateral ligament (Fig. 1-4).
Expanding the Distal Lateral Exposure (7)
Expanding the distal lateral exposure is indicated in reconstruction of the lateral ulnar collateral ligament.
Landmarks include the lateral epicondyle, posterior
border of the extensor carpi ulnaris, anterior edge of the anconeus,
and the crista supinatoris.
border of the extensor carpi ulnaris, anterior edge of the anconeus,
and the crista supinatoris.
 |
|
FIG. 1-2.
The two most common incisions for extensile exposure of the elbow are a Kocher posterolateral and a straight posterior incision that deviates just medial or lateral to the tip of the olecranon. |
 |
|
FIG. 1-3. The interval between the anconeus and the extensor carpi ulnaris is the major landmark for the Kocher incision.
|
 |
|
FIG. 1-4.
Separating this interval exposes the lateral capsule covering the radial humeral joint. Care must be taken to expose the radial head anterior to the crista supinatoris. (Abbreviation: ECU, extensor carpi ulnaris.) |
P.5
P.6
Surgery
If the lateral ulnar collateral ligament is to be
reconstructed, the skin incision described earlier is simply extended
proximally about 3 cm (Fig. 1-3).
reconstructed, the skin incision described earlier is simply extended
proximally about 3 cm (Fig. 1-3).
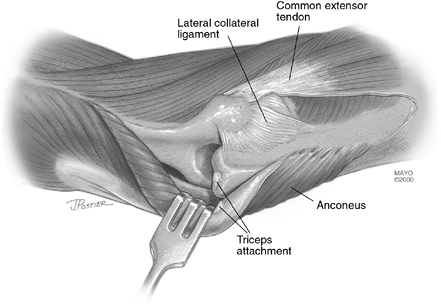
After the interval is entered the anconeus is more completely reflected from its ulnar insertion (Fig. 1-5).
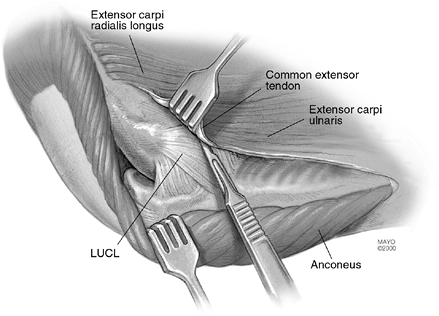
The lateral collateral ligament complex is identified by first
elevating the extensor carpi ulnaris from the annular ligament just
distal to the lateral epicondyle (Fig. 1-6).
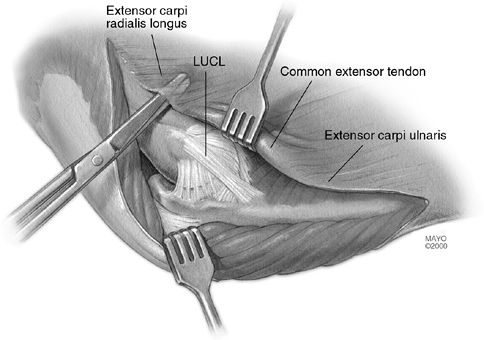
The fleshy attachment of the extensor carpi radialis longus is
identified just above the common extensor tendon. This origin is freed
from the supracondylar ridge. The dissection then elevates the common
extensor tendon and the posterior edge of the extensor carpi radialis
brevis from the lateral ligament complex (Fig. 1-7).
This is done very carefully to identify and leave intact the lateral
collateral ligament complex so that the lateral ulnar collateral
ligament can be reconstructed (see Chapter 15).
The lateral collateral ligament complex is identified by first
elevating the extensor carpi ulnaris from the annular ligament just
distal to the lateral epicondyle (Fig. 1-6).
The fleshy attachment of the extensor carpi radialis longus is
identified just above the common extensor tendon. This origin is freed
from the supracondylar ridge. The dissection then elevates the common
extensor tendon and the posterior edge of the extensor carpi radialis
brevis from the lateral ligament complex (Fig. 1-7).
This is done very carefully to identify and leave intact the lateral
collateral ligament complex so that the lateral ulnar collateral
ligament can be reconstructed (see Chapter 15).
The Proximal Lateral Exposure (7)
The proximal lateral exposure may be a proximal extension of the distal exposure or a focused proximal approach.
It is indicated for anterior-posterior capsular release for stiff elbow (Column procedure).
Landmarks include the extensor carpi radialis longus, anterior capsule.
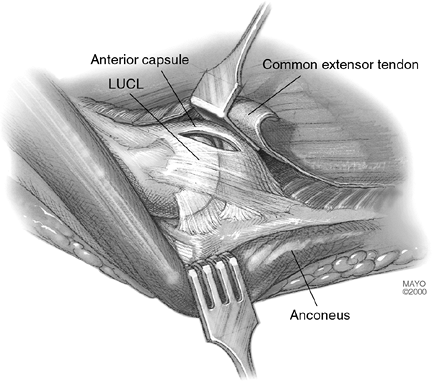
If an anterior capsular release is to be performed, a
new, limited exposure is described. The skin incision is drawn over the
lateral column extending proximal to the lateral epicondyle (Fig. 1-2).
The extensor carpi radialis longus is elevated from the lateral column
and epicondyle, and the anterior capsule is visualized. An incision is
made in the capsule just superior to the collateral ligament (Fig. 1-8).
A periosteal elevator is used to elevate the brachialis muscle off the
anterior capsule, which can be safely performed, since the arthrotomy
provides accurate spatial orientation from lateral to medial across the
joint. The procedure then continues as described in Chapter 21.
new, limited exposure is described. The skin incision is drawn over the
lateral column extending proximal to the lateral epicondyle (Fig. 1-2).
The extensor carpi radialis longus is elevated from the lateral column
and epicondyle, and the anterior capsule is visualized. An incision is
made in the capsule just superior to the collateral ligament (Fig. 1-8).
A periosteal elevator is used to elevate the brachialis muscle off the
anterior capsule, which can be safely performed, since the arthrotomy
provides accurate spatial orientation from lateral to medial across the
joint. The procedure then continues as described in Chapter 21.
Note: If an extensile
exposure is anticipated, a posterior incision is made. The same deep
exposure can be accomplished by extending the posterior lateral skin
incision and elevating the lateral skin cutaneous flap.
exposure is anticipated, a posterior incision is made. The same deep
exposure can be accomplished by extending the posterior lateral skin
incision and elevating the lateral skin cutaneous flap.
 |
|
FIG. 1-5. For a more detailed exposure of the lateral ligament complex the anconeus is reflected posterior from its ulnar insertion.
|
 |
|
FIG. 1-6.
The posterior margin of the extensor carpi ulnaris serves as the interval through which the common extensor muscles may be elevated, exposing the lateral collateral ligament complex. (Abbreviation: LUCL, lateral ulnar collateral ligament.) |
 |
|
FIG. 1-7.
The common extensor tendon may be elevated in continuity with the extensor carpi radialis longus exposing the anterolateral capsule and lateral ulnar collateral ligament. |
 |
|
FIG. 1-8. Incision into the capsule provides an orientation that allows exposure of the remainder of the anterior capsule.
|
P.7
P.8
P.9
Extensile Exposures
The extensile posterolateral exposure (Kocher) (6) is an extension of the limited exposures described earlier involving the release of collateral ligament and capsule.
Extensile exposure to the joint surface is indicated for
reconstructive procedures, including open reduction internal fixation,
total elbow arthroplasty (resurfacing), and interposition arthroplasty.
reconstructive procedures, including open reduction internal fixation,
total elbow arthroplasty (resurfacing), and interposition arthroplasty.
Landmarks include the proximal lateral column and the distal Kocher interval.
The triceps may be elevated from the posterior aspect of
the humerus by extending the skin incision proximally up the lateral
column (Fig. 1-2). This may proceed 6 to 7 cm proximal to the lateral epicondyle without fear of violence to the radial nerve.
the humerus by extending the skin incision proximally up the lateral
column (Fig. 1-2). This may proceed 6 to 7 cm proximal to the lateral epicondyle without fear of violence to the radial nerve.
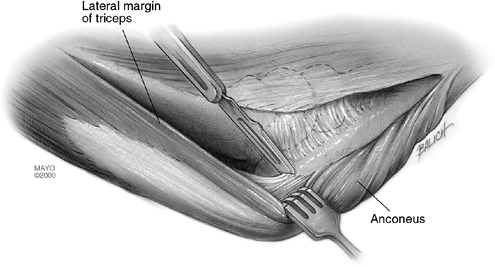
Proceed as shown in Fig. 1-5 by
completely elevating the anconeus from the ulna. The triceps is easily
elevated from the posterior humerus in the normal situation, and even
in posttraumatic contractures it can be elevated with a periosteal
elevator without much additional difficulty (Fig. 1-9).
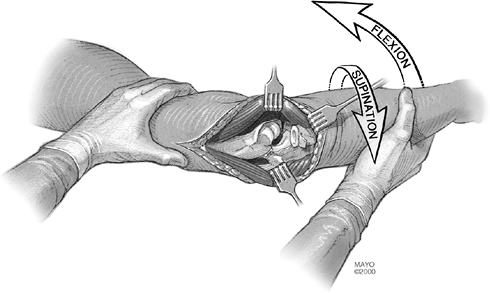
The lateral collateral ligament is released from the humeral origin as
a separate structure or if prior surgery has caused scarring, with the
common extensor tendon complex. The anterior capsule is then incised. A
varus stress is applied to the elbow, which opens like a book hinging
on the medial ulnar collateral ligament (UCL) and common flexor muscles
(Fig. 1-10). The triceps remains attached to the ulna.
completely elevating the anconeus from the ulna. The triceps is easily
elevated from the posterior humerus in the normal situation, and even
in posttraumatic contractures it can be elevated with a periosteal
elevator without much additional difficulty (Fig. 1-9).
The lateral collateral ligament is released from the humeral origin as
a separate structure or if prior surgery has caused scarring, with the
common extensor tendon complex. The anterior capsule is then incised. A
varus stress is applied to the elbow, which opens like a book hinging
on the medial ulnar collateral ligament (UCL) and common flexor muscles
(Fig. 1-10). The triceps remains attached to the ulna.
 |
|
FIG. 1-9. The lateral margin of the triceps may be readily separated from the posterior aspect of the lateral column.
|
 |
|
FIG. 1-10.
By releasing the common extensor tendon and the anterior capsule as well as the triceps and anconeus posteriorly, a varus stress to the elbow allows it to hinge on the medial collateral ligament and flexor pronator group, providing an extensile exposure to the joint.) |
P.10
Mayo Modified Kocher Extensile Posterior-Lateral Exposure
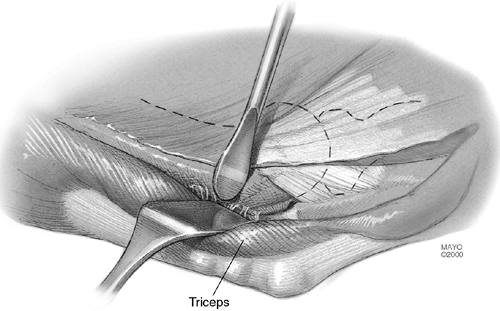
The triceps attachment is further released from the olecranon and the triceps mechanism is reflected from lateral to medial (Fig. 1-11).
This procedure is indicated in ankylosis release,
resurfacing arthroplasty, open reduction with internal fixation (ORIF)
lateral column, distal humerus.
resurfacing arthroplasty, open reduction with internal fixation (ORIF)
lateral column, distal humerus.
Landmarks include the triceps insertion at the olecranon.
 |
|
FIG. 1-11. The Kocher approach is extended by releasing the triceps attachment along with the mobilized anconeus muscle.
|
 |
|
FIG. 1-12.
The brachial fascia is excised at the margin of the medial aspect of the triceps exposing the ulnar nerve. This may be done through a Kocher incision by subcutaneous dissection. |
P.11
If more extensile exposure is required than has been obtained with the previous steps (Figs. 1-9 and 1-10), a medial skin flap is elevated and the ulnar nerve is identified (Fig. 1-12).
It is protected or translocated according to the merits of the case and
after the release has proceeded according to the steps shown in Figs. 1-5, 1-8, and 1-9. The triceps and anconeus muscle sleeve is reflected from the tip of the olecranon by releasing Sharpey’s fibers (Fig. 1-13). The entire extensor mechanism, including anconeus, is thus reflected from lateral
It is protected or translocated according to the merits of the case and
after the release has proceeded according to the steps shown in Figs. 1-5, 1-8, and 1-9. The triceps and anconeus muscle sleeve is reflected from the tip of the olecranon by releasing Sharpey’s fibers (Fig. 1-13). The entire extensor mechanism, including anconeus, is thus reflected from lateral
P.12
to medial (Fig. 1-14).
After the triceps has been reflected and the posterior capsule
released, the lateral collateral ligament may be detached from the
humerus, depending upon the goal of the specific procedure and the
additional exposure required. By flexing the elbow and removing the tip
of the olecranon, the articular surface and the entire posterior
humerus can be exposed.
 |
|
FIG. 1-13. The triceps is released from the tip of the olecranon.
|
 |
|
FIG. 1-14. The entire extensor mechanism may be translated from the lateral to the medial aspect of the joint.
|
Limited Exposure Proximal Portion of Kocher Incision
The “Column Procedure”
Note: As a similar exposure
has been described for the medial joint, this approach will henceforth
be referred to as the “lateral column.”
has been described for the medial joint, this approach will henceforth
be referred to as the “lateral column.”
It is indicated in the case of anterior-posterior capsular release or removal of coronoid or olecranon osteophytes.
Surgery
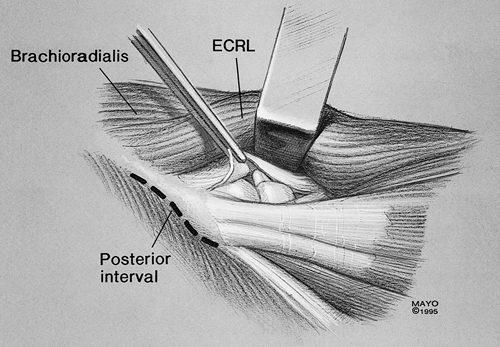
A 6- to 7-cm incision is made over lateral column, 2 cm distal and 4 cm proximal to lateral epicondyle.
The lateral epicondyle is exposed. The extensor carpi
radialis longus (ECRL) is identified, as are the muscle fibers
immediately proximal to the common extensor tendon. A hockey stick
incision is performed laterally and extended distally in line with the
fibers of the common extensor tendon over the radiocapitellar joint.
The muscular attachment of the distal fibers of the brachial radialis
and ECRL are released from the lateral column, exposing the extensor
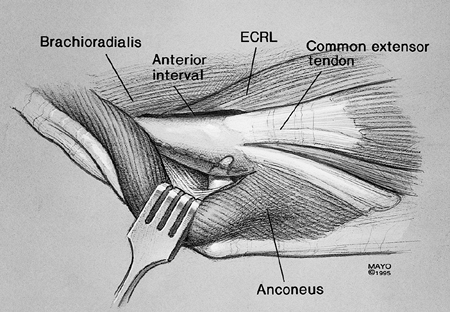
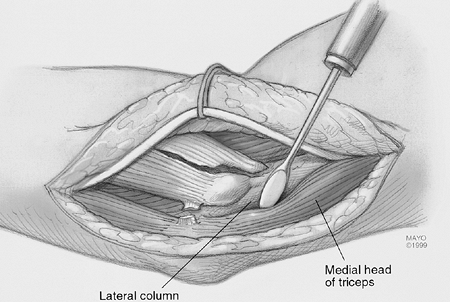
capsule (Fig. 1-15). If necessary, the triceps may be elevated and the posterior capsule also exposed (Fig. 1-16).
radialis longus (ECRL) is identified, as are the muscle fibers
immediately proximal to the common extensor tendon. A hockey stick
incision is performed laterally and extended distally in line with the
fibers of the common extensor tendon over the radiocapitellar joint.
The muscular attachment of the distal fibers of the brachial radialis
and ECRL are released from the lateral column, exposing the extensor
capsule (Fig. 1-15). If necessary, the triceps may be elevated and the posterior capsule also exposed (Fig. 1-16).
 |
|
FIG. 1-15.
Limited exposure to the anterior capsule realized by elevating the humeral origin of the ECRB and distal fibers of the brachioradialis. |
 |
|
FIG. 1-16. By elevating the triceps from the posterior aspect of the lateral column, the posterior capsule and olecranon may be exposed.
|
P.13
P.14
Posterior-Medial Exposure
The extensile Mayo approach of Bryan-Morrey (1)
is indicated in the case of ankylosis release, semiconstrained total
elbow arthroplasty, ORIF medial column, distal humeral fractures.
is indicated in the case of ankylosis release, semiconstrained total
elbow arthroplasty, ORIF medial column, distal humeral fractures.
Surgery
A 14-cm skin incision is made just medial to the tip of
the olecranon. The dissection is carried to the medial aspect of the
triceps 6 cm proximal and 4 cm distal to the tip of the olecranon. The
ulnar nerve is identified, and if a femoral translocation is carried
out, it is released from the margin of the triceps and elevated from
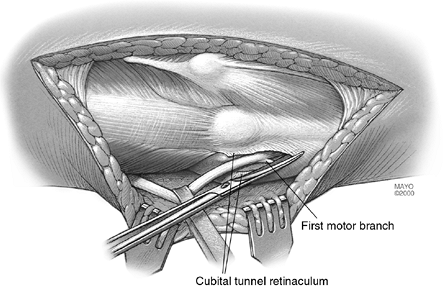
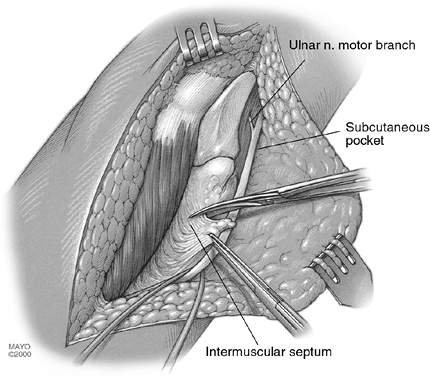
its bed (Fig. 1-17). The cubital tunnel
retinaculum is split and the nerve is released to the first motor
branch. A subcutaneous pocket is developed, the intermuscular septum is
removed (Fig. 1-18), and the nerve is
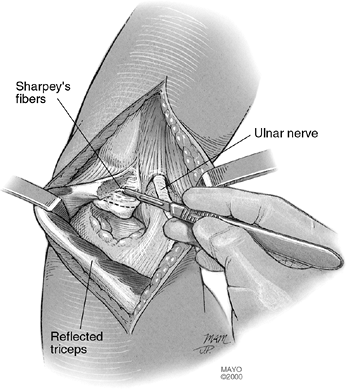
translated anteriorly. The triceps is released from the entire
posterior aspect of the distal humerus. The forearm fascia and ulnar
periosteum are elevated from the medial margin of the ulna. The Sharpey
fiber attachment of the triceps to the olecranon is released by sharp
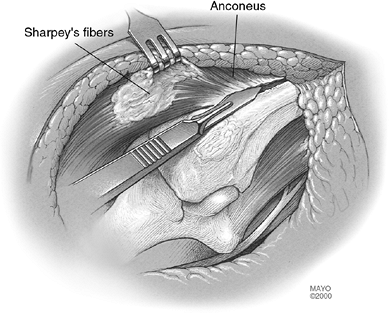
dissection (Fig. 1-19). The distal forearm
fascia and ulnar periosteum are elevated from the ulna. The lateral
margin of the proximal ulna is then identified and the anconeus is
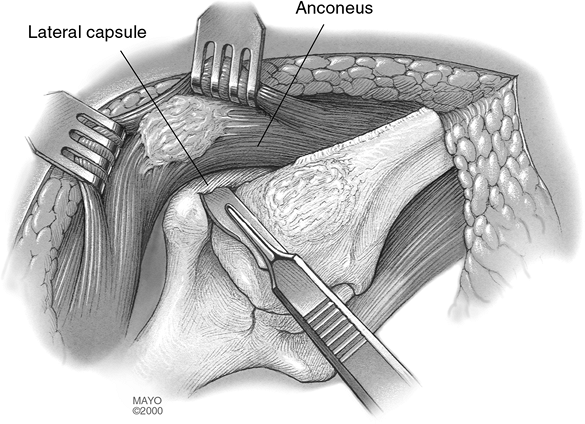
elevated from its ulnar bed (Fig. 1-20). The extensor mechanism and capsule continues to be reflected from the margin of the lateral epicondyle (Fig. 1-21).
If a medial column fracture has occurred, the tip of the olecranon is
removed and the fracture may be addressed. For semiconstrained total
elbow arthroplasty the lateral and medial collateral ligaments are
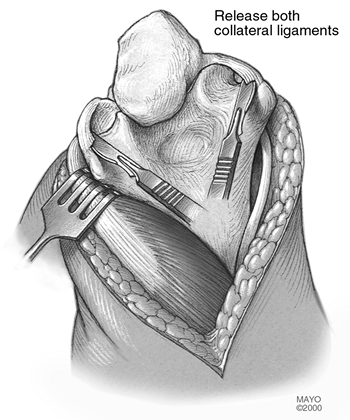
released and the extensor mechanism is reflected lateral to the
epicondyle. The elbow is flexed and the tip of the olecranon is removed
to expose the joint (Fig. 1-22).
the olecranon. The dissection is carried to the medial aspect of the
triceps 6 cm proximal and 4 cm distal to the tip of the olecranon. The
ulnar nerve is identified, and if a femoral translocation is carried
out, it is released from the margin of the triceps and elevated from
its bed (Fig. 1-17). The cubital tunnel
retinaculum is split and the nerve is released to the first motor
branch. A subcutaneous pocket is developed, the intermuscular septum is
removed (Fig. 1-18), and the nerve is
translated anteriorly. The triceps is released from the entire
posterior aspect of the distal humerus. The forearm fascia and ulnar
periosteum are elevated from the medial margin of the ulna. The Sharpey
fiber attachment of the triceps to the olecranon is released by sharp
dissection (Fig. 1-19). The distal forearm
fascia and ulnar periosteum are elevated from the ulna. The lateral
margin of the proximal ulna is then identified and the anconeus is
elevated from its ulnar bed (Fig. 1-20). The extensor mechanism and capsule continues to be reflected from the margin of the lateral epicondyle (Fig. 1-21).
If a medial column fracture has occurred, the tip of the olecranon is
removed and the fracture may be addressed. For semiconstrained total
elbow arthroplasty the lateral and medial collateral ligaments are
released and the extensor mechanism is reflected lateral to the
epicondyle. The elbow is flexed and the tip of the olecranon is removed
to expose the joint (Fig. 1-22).
 |
|
FIG. 1-17.
Through a posterior skin incision, the ulnar nerve has been identified and dissected from its bed at the margin of the triceps. The cubital tunnel retinaculum has been released with further dissection to the first motor branch. It is translocated anterior to the medial epicondyle to a subcutaneous pocket. |
 |
|
FIG. 1-18. The intermuscular septum is removed to avoid compression on the nerve with its new anterior course.
|
 |
|
FIG. 1-19. Incontinuity elevation of the insertion of the triceps from the olecranon.
|
 |
|
FIG. 1-20.
The forearm fascia and ulnar periosteum has been elevated from the ulna distally, the triceps from the posterior aspect of the humerus proximally, and the insertion in the triceps is further reflected from its insertion into the tip of the olecranon. Further reflection laterally allows identification of the anconeus, which is then elevated from its ulnar insertion. |
 |
|
FIG. 1-21.
The dissection continues laterally, allowing reflection of fibers of the extensor mechanism and the capsule from the lateral column. |
 |
|
FIG. 1-22.
By subluxing the extensor mechanism lateral to the lateral condyle, the lateral ulnar collateral ligament may be released. For total elbow arthroplasty the medial collateral ligament is also released, allowing complete exposure of the ulnohumeral joint. |
P.15
P.16
P.17
The Triceps
In every instance in which the triceps has been completely reflected either from lateral to medial (Fig. 1-14) or from medial to lateral (Fig. 1-21)
it is always securely reattached to the olecranon with a crisscross
type of suture. Drill holes about 3 cm in length are placed in a
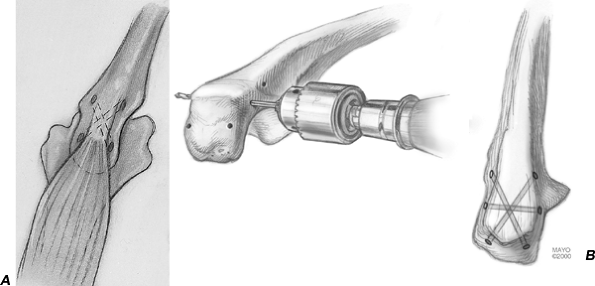
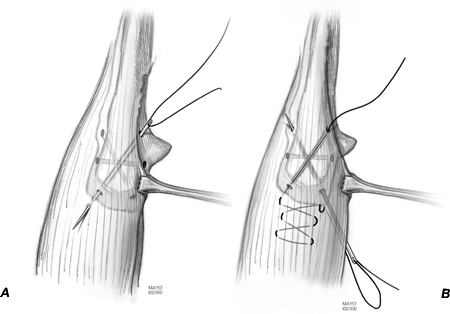
cruciate fashion in the olecranon from proximal to distal (Fig. 1-23A). A third transverse hole is drilled through the olecranon to secure a second stabilizing suture (Fig. 1-23B). The margin of the triceps is first grasped with an Alis clamp and brought over the olecranon (Fig. 1-24A).
A No. 5 nonabsorbable suture is introduced with a straight needle from
distal lateral to proximal medial for the modified Kocher and from
distal medial to proximal lateral for the Mayo exposure. The suture is
first brought through the tip of the olecranon and passes through the
triceps tissue at its anatomic attachment site with the elbow in 90
degrees (Fig. 1-24A). A Bunnell type of
crisscross suture is then placed in the triceps tendon, after which the
suture enters the opposite hole in the olecranon now being passed from
proximal to distal. After the suture has emerged from the second hole
in the olecranon it is brought back over the top of the ulna through
the soft-tissue distal expansion of the extensor sleeve (Fig. 1-24B).
Care is taken to tie this stitch off to the side of the subcutaneous
border of the ulna to avoid irritation or skin erosion. The second
suture is placed transversely across the ulna, again, beginning on the
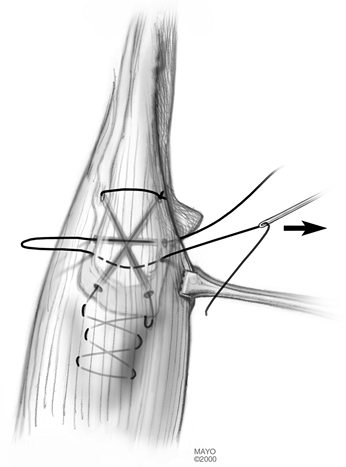
side from which the triceps reflection began (Fig. 1-25).
It is simply brought back across the triceps tendon in a transverse
fashion to snugly stabilize the triceps insertion against the
olecranon. All sutures are tied with the elbow in 90 degrees of
flexion, again with the knots off the subcutaneous border.
it is always securely reattached to the olecranon with a crisscross
type of suture. Drill holes about 3 cm in length are placed in a
cruciate fashion in the olecranon from proximal to distal (Fig. 1-23A). A third transverse hole is drilled through the olecranon to secure a second stabilizing suture (Fig. 1-23B). The margin of the triceps is first grasped with an Alis clamp and brought over the olecranon (Fig. 1-24A).
A No. 5 nonabsorbable suture is introduced with a straight needle from
distal lateral to proximal medial for the modified Kocher and from
distal medial to proximal lateral for the Mayo exposure. The suture is
first brought through the tip of the olecranon and passes through the
triceps tissue at its anatomic attachment site with the elbow in 90
degrees (Fig. 1-24A). A Bunnell type of
crisscross suture is then placed in the triceps tendon, after which the
suture enters the opposite hole in the olecranon now being passed from
proximal to distal. After the suture has emerged from the second hole
in the olecranon it is brought back over the top of the ulna through
the soft-tissue distal expansion of the extensor sleeve (Fig. 1-24B).
Care is taken to tie this stitch off to the side of the subcutaneous
border of the ulna to avoid irritation or skin erosion. The second
suture is placed transversely across the ulna, again, beginning on the
side from which the triceps reflection began (Fig. 1-25).
It is simply brought back across the triceps tendon in a transverse
fashion to snugly stabilize the triceps insertion against the
olecranon. All sutures are tied with the elbow in 90 degrees of
flexion, again with the knots off the subcutaneous border.
 |
|
FIG. 1-23. A: The first step of the triceps repair consists of drill holes placed in a cruciate fashion through the proximal ulna. B: A second transverse tunnel is made in the olecranon.
|
 |
|
FIG. 1-25.
A transverse suture is then typically placed across the proximal ulna, further securing the triceps mechanism to its ulnar insertion. |
 |
|
FIG. 1-24. A:
The triceps is reduced and a No. 5 nonabsorbable suture begins from distal to proximal, starting on the side of the reflected extensor mechanism, thus medially for the Mayo approach and laterally for the extensile Kocher approach. B: The suture is crisscrossed in the triceps tendon and then brought back through the other drill hole in the ulna. The suture is tied to the margin of the ulna, taking care to avoid the subcutaneous border. |
P.18
P.19
Closure
For both medial and lateral exposures, if an interval
has been entered it is reapproximated. On the lateral side, a running-0
absorbable suture is used to close Kocher’s interval. The common
extensor and common flexor muscles are reattached. If needed, two holes
are placed in the supracondylar ridge and the ECRL, and the remaining
portion of the common extensor tendon are reattached directly to bone.
has been entered it is reapproximated. On the lateral side, a running-0
absorbable suture is used to close Kocher’s interval. The common
extensor and common flexor muscles are reattached. If needed, two holes
are placed in the supracondylar ridge and the ECRL, and the remaining
portion of the common extensor tendon are reattached directly to bone.
Skin closure is with staples, although sometimes a
subcuticular stitch is used, particularly in females. The aftercare
varies dramatically, depending upon the pathology being addressed, and
this is discussed in the appropriate chapter. It is worthy of note,
however, that I typically splint the elbow in extension with an
anterior splint. This protects the incision and may help reduce the
tendency to develop flexion contracture.
subcuticular stitch is used, particularly in females. The aftercare
varies dramatically, depending upon the pathology being addressed, and
this is discussed in the appropriate chapter. It is worthy of note,
however, that I typically splint the elbow in extension with an
anterior splint. This protects the incision and may help reduce the
tendency to develop flexion contracture.
P.20
Medial Extensile Exposures (5)
Comment: It is suggested the medial extensile exposure now be termed the medial column approach, as it is analogous to that of the lateral side (Hotchkiss R, Personal Communication, April 1999).
The procedure is indicated if there is access to the
coronoid with intact radial head and anterior capsule release, ulnar
nerve dissection is required, there is a need to preserve the
posterolateral ulnohumeral ligament complex, anterior and posterior
access to the joint is needed, or conversion to triceps-sparing
exposure of Bryan-Morrey anticipated.
coronoid with intact radial head and anterior capsule release, ulnar
nerve dissection is required, there is a need to preserve the
posterolateral ulnohumeral ligament complex, anterior and posterior
access to the joint is needed, or conversion to triceps-sparing
exposure of Bryan-Morrey anticipated.
It is less desirable if there is need of excision of heterotopic bone on the lateral side or access to radial head is needed.
Surgery
The patient is usually supine, supported by a hand or
elbow table. The patient’s head may require support, and a roll is
placed under the scapula.
elbow table. The patient’s head may require support, and a roll is
placed under the scapula.
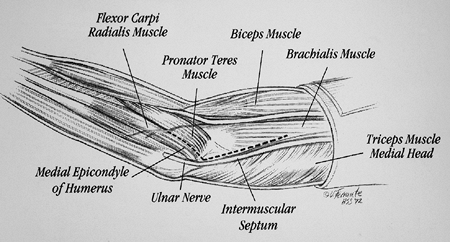
The deep exposure may be accessed through a midline
posterior incision or a posterior medial incision. The key to this
exposure is identification of the medial supracondylar ridge of the
humerus, the medial intermuscular septum, the origin of the flexor
pronator muscle mass, and the ulnar nerve (Fig. 1-26).
posterior incision or a posterior medial incision. The key to this
exposure is identification of the medial supracondylar ridge of the
humerus, the medial intermuscular septum, the origin of the flexor
pronator muscle mass, and the ulnar nerve (Fig. 1-26).
The subcutaneous skin is elevated and the medial
intermuscular septum is identified. Anterior to the septum, running
just on top of the fascia (and not in the subdermal tissue), the medial
antebrachial cutaneous nerve is identified and protected. It may
occasionally be necessary to divide this nerve to gain full exposure
and adequately mobilize the ulnar nerve, especially in revision
surgery. If the patient has had previous surgery, the ulnar nerve is
usually most easily identified proximally before proceeding distally.
If a previous anterior transposition was performed, the nerve should be
carefully identified both proximally and distally before proceeding.
intermuscular septum is identified. Anterior to the septum, running
just on top of the fascia (and not in the subdermal tissue), the medial
antebrachial cutaneous nerve is identified and protected. It may
occasionally be necessary to divide this nerve to gain full exposure
and adequately mobilize the ulnar nerve, especially in revision
surgery. If the patient has had previous surgery, the ulnar nerve is
usually most easily identified proximally before proceeding distally.
If a previous anterior transposition was performed, the nerve should be
carefully identified both proximally and distally before proceeding.
The surface of the flexor pronator muscle mass origin is
visualized by elevating and sweeping the subcutaneous tissue laterally
as a flap with the medial antebrachial cutaneous nerve.
visualized by elevating and sweeping the subcutaneous tissue laterally
as a flap with the medial antebrachial cutaneous nerve.
 |
|
FIG. 1-26. Landmarks for the medial extensile exposure include the medial epicondyle, intramuscular septum, and ulnar nerve.
|
P.21
The medial intermuscular septum is identified anteriorly
and posteriorly and then released for a distance of about 5 cm
proximally (Fig. 1-27).
and posteriorly and then released for a distance of about 5 cm
proximally (Fig. 1-27).
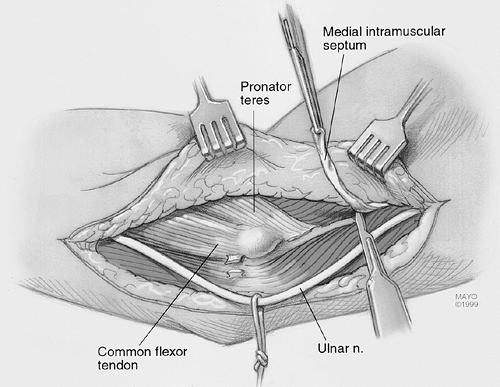
Locate the medial supracondylar ridge and begin
elevating the anterior muscle with a periosteal elevator.
Subperiosteally elevate enough of the anterior structures of the distal
humeral region to allow the placement of a wide retractor. The median
nerve, brachial artery, and vein are superficial to the brachialis
muscle and are not identified. The flexor pronator muscle mass is
divided in line with its fibers, leaving a portion of flexor carpi
ulnaris tendon attached to the epicondyle (Fig. 1-28).
A small cuff of fibrous tissue of the origin can be left on the
supracondylar ridge as the muscle is elevated to facilitate
reattachment when closing. The muscle is elevated from the capsule
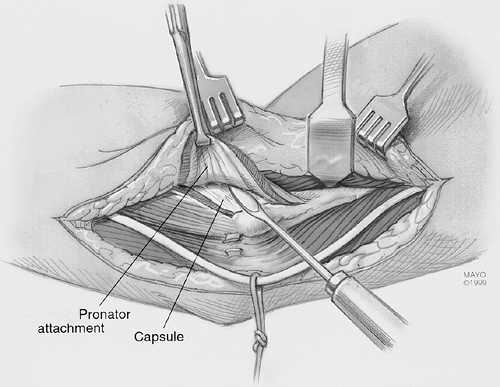
encountering the brachialis muscle laterally. A proximal, transverse
incision in the lacertus fibrosis may also be needed to adequately
mobilize this layer of muscle. The muscle is elevated from the capsule
as the dissection proceeds laterally and distally, exposing the entire
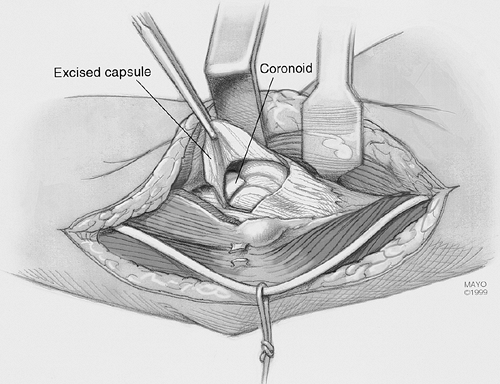
anterior capsule (Fig. 1-29). At this stage the
pathology is addressed. If necessary the posterior capsule may be
exposed by elevating the triceps from its lateral distal humeral
attachment (Fig. 1-30).
elevating the anterior muscle with a periosteal elevator.
Subperiosteally elevate enough of the anterior structures of the distal
humeral region to allow the placement of a wide retractor. The median
nerve, brachial artery, and vein are superficial to the brachialis
muscle and are not identified. The flexor pronator muscle mass is
divided in line with its fibers, leaving a portion of flexor carpi
ulnaris tendon attached to the epicondyle (Fig. 1-28).
A small cuff of fibrous tissue of the origin can be left on the
supracondylar ridge as the muscle is elevated to facilitate
reattachment when closing. The muscle is elevated from the capsule
encountering the brachialis muscle laterally. A proximal, transverse
incision in the lacertus fibrosis may also be needed to adequately
mobilize this layer of muscle. The muscle is elevated from the capsule
as the dissection proceeds laterally and distally, exposing the entire
anterior capsule (Fig. 1-29). At this stage the
pathology is addressed. If necessary the posterior capsule may be
exposed by elevating the triceps from its lateral distal humeral
attachment (Fig. 1-30).
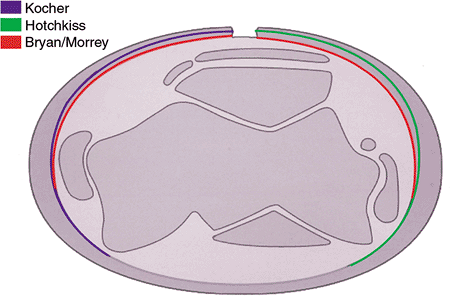
We have found that the described surgical exposures to
the elbow are sufficient, so virtually all the reconstructive
procedures can be adequately performed. All may be executed after a
posterior skin incision (Fig. 1-31). The
surgeon should be aware that the classic extensile approach described
by Kocher implies that the anterior capsule has been incised and the
lateral collateral ligament has been released (6).
The Mayo (R. S. Bryan) modification of the Kocher approach consists of
reflection and release of the extensor mechanism from the tip of the
olecranon in a fashion similar to that described for the Mayo approach (1) (see Fig. 1-11).
This permits much better exposure of both humeral and ulnar articular
surfaces. However, if reflected, the triceps must be securely
reattached to bone. Further, when the Mayo modified Kocher release has
been performed, the ulnar nerve must be exposed and released as
necessary to avoid compression with varus angular forearm manipulation.
the elbow are sufficient, so virtually all the reconstructive
procedures can be adequately performed. All may be executed after a
posterior skin incision (Fig. 1-31). The
surgeon should be aware that the classic extensile approach described
by Kocher implies that the anterior capsule has been incised and the
lateral collateral ligament has been released (6).
The Mayo (R. S. Bryan) modification of the Kocher approach consists of
reflection and release of the extensor mechanism from the tip of the
olecranon in a fashion similar to that described for the Mayo approach (1) (see Fig. 1-11).
This permits much better exposure of both humeral and ulnar articular
surfaces. However, if reflected, the triceps must be securely
reattached to bone. Further, when the Mayo modified Kocher release has
been performed, the ulnar nerve must be exposed and released as
necessary to avoid compression with varus angular forearm manipulation.
 |
|
FIG. 1-27. The dissection is carried to the intramuscular septum, which is released.
|
 |
|
FIG. 1-28.
The medial aspect of the brachialis is identified and elevated from the distal humerus. The flexor and pronator muscle mass are identified. The pronator component is released and elevated. |
 |
|
FIG. 1-29. The entire sleeve of soft tissue is elevated from the capsule.
|
 |
|
FIG. 1-30. The posterior column is exposed by elevating the triceps and anconeus from the posterior aspect of the lateral column.
|
 |
|
FIG. 1-31.
The posterior skin incision allows ready exposure of the medial and lateral aspects of the joint by mobilization of the cutaneous flaps medially and laterally. |
P.22
P.23
P.24
Modification of the Mayo approach has been described by Wolfe and Ranawat (12)
in which the triceps is removed with a wafer of bone rather than being
reflected sharply from the olecranon. Finally, conversion or extension
between the Mayo and the Hotchkiss experience is readily accomplished
if needed.
in which the triceps is removed with a wafer of bone rather than being
reflected sharply from the olecranon. Finally, conversion or extension
between the Mayo and the Hotchkiss experience is readily accomplished
if needed.
Results
There have been limited attempts to document the
efficacy of one or the other of the various types of triceps-sparing
approaches. In the original description we compared the clinical result
of the Mayo approach to that of the triceps splitting or transverse
release of the triceps attachment (1). There
were no triceps disruptions after approximately 75 procedures done with
the triceps being released in continuity (Mayo approach) compared with
an approximately 20% complication rate when the triceps was released
transversely. Wolfe and Ranawat (12) have also
observed no instances of triceps insufficiency with their modification
of this approach. The use of the Mayo medial exposure was also shown to
have improved triceps strength after total elbow arthroplasty (8).
This manner of exposing the elbow was found to be associated with
approximately 20% greater extension strength than with the Campbell
(Van Gorder) type of exposure.
efficacy of one or the other of the various types of triceps-sparing
approaches. In the original description we compared the clinical result
of the Mayo approach to that of the triceps splitting or transverse
release of the triceps attachment (1). There
were no triceps disruptions after approximately 75 procedures done with
the triceps being released in continuity (Mayo approach) compared with
an approximately 20% complication rate when the triceps was released
transversely. Wolfe and Ranawat (12) have also
observed no instances of triceps insufficiency with their modification
of this approach. The use of the Mayo medial exposure was also shown to
have improved triceps strength after total elbow arthroplasty (8).
This manner of exposing the elbow was found to be associated with
approximately 20% greater extension strength than with the Campbell
(Van Gorder) type of exposure.
An additional consideration in those with rheumatoid
arthritis is the thin olecranon that compromises healing if an
osteotomy is carried out (3). The transverse osteotomy of McAusland is associated with an approximately 5% nonunion rate (7).
Although for fractures the chevron osteotomy may improve these results
and decrease the nonunion rate, I personally have not had the clinical
need to osteotomize the olecranon in the last 14 years, and this should
be avoided if the olecranon has been thinned.
arthritis is the thin olecranon that compromises healing if an
osteotomy is carried out (3). The transverse osteotomy of McAusland is associated with an approximately 5% nonunion rate (7).
Although for fractures the chevron osteotomy may improve these results
and decrease the nonunion rate, I personally have not had the clinical
need to osteotomize the olecranon in the last 14 years, and this should
be avoided if the olecranon has been thinned.
Complications
One beauty of the previously described exposures is that
they are relatively free of complication. Today most problems are
related to the pathology rather than to the surgical approach.
they are relatively free of complication. Today most problems are
related to the pathology rather than to the surgical approach.
Difficult ankylosis release procedures are associated
with a significant amount of swelling as often occurs in patients
undergoing total elbow arthroplasty. Wound healing is generally not a
problem, however, and is related to the presence of prior incisions and
the magnitude of the dissection, as is typical for release of the stiff
elbow.
with a significant amount of swelling as often occurs in patients
undergoing total elbow arthroplasty. Wound healing is generally not a
problem, however, and is related to the presence of prior incisions and
the magnitude of the dissection, as is typical for release of the stiff
elbow.
The infection rate after total elbow arthroplasty has
been reduced at our institution from a high of 11% in 1970 to
approximately 3% over the last 10 years (8).
This reduction is coincident with adopting the Mayo approach to the
elbow, but other technique changes have occurred in this period,
including using antibiotic-impregnated cement and splinting the elbow
in extension.
been reduced at our institution from a high of 11% in 1970 to
approximately 3% over the last 10 years (8).
This reduction is coincident with adopting the Mayo approach to the
elbow, but other technique changes have occurred in this period,
including using antibiotic-impregnated cement and splinting the elbow
in extension.
Injury to the ulnar nerve appears to be more common in
those instances in which the ulnar nerve is not exposed and the elbow
is flexed on the medial collateral ligament, as with the classical
extensile Kocher approach (2,11).
Simply exposing the ulnar nerve, although it decreases this
complication, does not completely obviate it. The theoretical
disadvantage of the Mayo approach, which allows translocation of the
ulnar nerve, is that this maneuver devascularizes the nerve and the
dissection itself may cause ulnar nerve irritation. Having used this
particular exposure in more than 500 cases, the incidence of permanent
ulnar nerve injury with motor dysfunction is less than 1%. I am
therefore comfortable exposing and moving the ulnar nerve in a
subcutaneous pocket as an essential and integral part of the Mayo
triceps-sparing approach.
those instances in which the ulnar nerve is not exposed and the elbow
is flexed on the medial collateral ligament, as with the classical
extensile Kocher approach (2,11).
Simply exposing the ulnar nerve, although it decreases this
complication, does not completely obviate it. The theoretical
disadvantage of the Mayo approach, which allows translocation of the
ulnar nerve, is that this maneuver devascularizes the nerve and the
dissection itself may cause ulnar nerve irritation. Having used this
particular exposure in more than 500 cases, the incidence of permanent
ulnar nerve injury with motor dysfunction is less than 1%. I am
therefore comfortable exposing and moving the ulnar nerve in a
subcutaneous pocket as an essential and integral part of the Mayo
triceps-sparing approach.
Although posterior interosseous nerve palsy is known to occur with some approaches to the radial nerve (4,10), the complication is virtually unheard of when the joint is exposed through Kocher’s interval.
Triceps disruption is very uncommon with either the Mayo
modified extensile Kocher exposure or the Mayo medial-to-lateral type
of approach.
modified extensile Kocher exposure or the Mayo medial-to-lateral type
of approach.
P.25
The incidence of triceps disruption therefore is less than 1% in our experience (9).
If, however, the triceps should become disrupted after either of the
procedures described earlier, if adequate tissue is present, it may be
reattached as described for the primary procedure. If the remaining
tissue is inadequate, triceps power is restored by either an anconeus
slide or an Achilles tendon allograft reconstruction (see Chapter 11).
If, however, the triceps should become disrupted after either of the
procedures described earlier, if adequate tissue is present, it may be
reattached as described for the primary procedure. If the remaining
tissue is inadequate, triceps power is restored by either an anconeus
slide or an Achilles tendon allograft reconstruction (see Chapter 11).
Recommended Readings
1. Bryan RS, Morrey BF. Extensive posterior exposure of the elbow: a triceps-sparing approach. Clin Orthop 1982;166:188.
2. Ewald FC, Jacobs MA. Total elbow arthroplasty. Clin Orthop 1984;182:137.
3. Inglis AE, Ranawat CS, Straub LR. Synovectomy and debridement of the elbow in rheumatoid arthritis. J Bone Joint Surg 1971;53A:652.
4. Kaplan EB. Surgical approaches to the proximal end of the radius and its use in fractures of the head and neck of the radius. J Bone Joint Surg 1941;23:86.
5. Kasparyan NG, Hotchkiss RN. Dynamic skeletal fixation in the upper extremity. Hand Clin 1997;13:643–663.
6. Kocher T. Text-book of operative surgery, 3rd ed. London: A and C Black; 1911.
7. Morrey BF. Surgical exposures of the elbow. In: Morrey BF, ed. The elbow and its disorders. Philadelphia: WB Saunders; 1985.
8. Morrey BF, Askew LJ, An KN. Strength function after elbow arthroplasty. Clin Orthop 1988;234:43–50.
9. Morrey BF, Bryan RS. Complications of total elbow arthroplasty. Clin Orthop 1982;170:204–212.
10. Strachan JH, Ellis BW. Vulnerability of the posterior interosseous nerve during radial head resection. J Bone Joint Surg 1971;53B:320.
11. Trancik T, Wilde AH, Borden LS. Capitellocondylar elbow arthroplasty. Two to eight year experience. Clin Orthop 1987;112:175.
12. Wolfe SW, Ranawat CS. The osteo-anconeus flap: an approach for total elbow arthroplasty. J Bone Joint Surg 1990;72A:684.