
Editors: Frassica, Frank J.; Sponseller, Paul D.; Wilckens, John H.
Title: 5-Minute Orthopaedic Consult, 2nd Edition
Copyright ©2007 Lippincott Williams & Wilkins
> Table of Contents > Tibial Spine Fracture
Tibial Spine Fracture
Jason W. Hammond MD
Peter R. Jay MD
Description
-
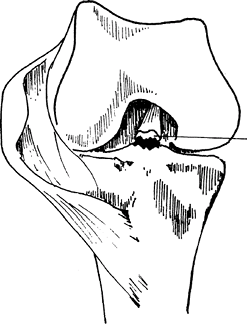
A fracture of the tibial spine or intercondylar eminence of the proximal tibia (Figs. 1 and 2)
-
Either the anterior tibial spine or, less commonly, the posterior tibial spine is affected; rarely are both involved.
-
The anterior tibial spine supplies part of the insertion for the ACL.
-
In the skeletally immature knee, the ACL
is thought to be stronger than the incompletely ossified tibial spine
to which it attaches.-
Thus, an avulsion of the tibial spine occurs instead of a torn ACL.
-
Occasionally, midsubstance ACL tears do occur in children.
-
A narrow femoral notch predisposes to midsubstance ACL injuries rather than tibial spine fractures (1).
-
-
-
Classification: The Meyers and McKeever classification (2) is based on the degrees of fracture displacement.
-
Type I: Minimally displaced
-
Type II: Displacement of the anterior portion of the fragment with a posterior hinge intact
-
Type III: Complete separation of the fragment with upward displacement and rotation
-
Epidemiology
Incidence
In 1 study, 4 times as common in children as in adults (3)
 |
|
Fig. 1. Tibial spine fracture.
|
Etiology
-
Fractures of the tibial spine result from violent twisting, varus-valgus injuries, or hyperextension.
-
Fractures may occur from direct contact with the adjacent femoral condyle.
-
Fall from a bicycle, athletic injury, or motor vehicle accident
Signs and Symptoms
History
-
History of trauma to the leg
-
Ask patients about other injuries.
Physical Exam
-
Pain, swelling, and effusion associated with hemarthrosis
-
Reluctance to bear weight
-
Lack of full extension secondary to bony block
-
Gently assess for knee stability
(anterior, posterior, varus, or valgus), which often is difficult to
detect in the acute setting because of guarding. -
Anterior laxity may be present.
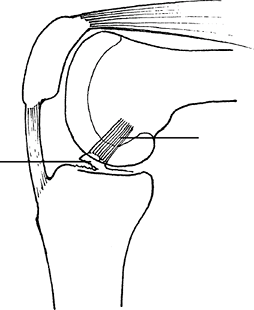 Fig. 2. A tibial spine fracture is best seen on the lateral radiograph and may involve only a small fragment of bone.
Fig. 2. A tibial spine fracture is best seen on the lateral radiograph and may involve only a small fragment of bone.
Tests
Imaging
-
Plain radiographs:
-
AP and lateral views of the knee usually are adequate.
-
Findings on the lateral radiograph are the foundation of the classification system and help to guide appropriate therapy.
-
A tunnel view or a radiograph parallel to the slant of the tibia can be helpful sometimes.
-
-
CT scanning may reveal other fracture lines or tibial plateau fracture.
-
MRI: Compared with tibial spine fractures
in children, those in adults have a higher incidence of concomitant
injuries (such as meniscal tears) requiring surgical treatment, and MRI
is recommended (4).
Pathological Findings
-
An avulsion at the insertion of the ACL
-
The ACL fans out and also inserts on the
anterior horn of the medial meniscus, which can be pulled into the
fracture site and can block reduction (5,6).
Differential Diagnosis
-
Isolated ligamentous injuries
-
Coincidental ligamentous injuries (ACL, OSD, MCL, LCL)
-
Patellar fracture
-
Patellar tendon rupture
-
Tibial tubercle fracture
-
Tibial plateau fracture
-
Isolated or coincidental meniscal injury
General Measures
-
Initial measures:
-
Ice, elevation, and immobilization should be initiated, even during evaluation.
-
If the hemarthrosis is causing severe pain, aspiration under sterile conditions helps relieve pressure in the knee.
-
-
Type I and II fractures:
-
Treat with closed reduction and an above-the-knee cylinder cast.
-
Placing the leg in full extension or hyperextension reduces the fragment.
-
The leg should be immobilized in a position between full extension and 10° of flexion.
-
The length of immobilization is 4–6 weeks.
-
-
-
Type III fractures:
-
Fractures should be reduced and immobilized.
-
Surgical treatment is recommended for most fractures to ensure reduction (7).
-
P.461
Activity
Patients may bear weight with the leg immobilized in extension.
Special Therapy
Physical Therapy
Physical therapy should begin after immobilization to work at ROM and strengthening of the leg.
Medication
First Line
Pain medications should be given as needed after fracture.
Surgery
-
Indicated for fractures that are not reduced.
-
Some clinicians have recommended surgical treatment for all type III tibial spine fractures.
-
Surgery can be accomplished via an open or arthroscopic approach.
-
The arthroscopic approach has become more popular.
-
-
Fractures should be reduced, and reduction should be maintained with internal fixation.
-
Sometimes reduction requires the removal of interfracture soft tissue.
-
-
Fixation can be with a screw or heavy suture, depending on the size of the fracture.
-
A recent biomechanical study has suggested that fixation with fiber wire is stronger than that with screws (8).
-
In children, screws should not cross the physis unless the child is nearing skeletal maturity.
Disposition
Issues for Referral
Tibial spine fractures should be referred to an orthopaedic surgeon.
Prognosis
-
Functional results of both screw and suture fixation are excellent if the fracture is reduced (9,10).
-
Measurement of ACL function with a KT-1000 arthrometer has shown excellent stability after fixation (11,12).
-
Excessive or symptomatic knee laxity may require ACL reconstruction (13).
Complications
-
Loose bodies
-
ACL laxity
-
Knee arthritis
-
Knee stiffness
-
Postoperative wound infection
-
DVT
Patient Monitoring
-
The patient should be followed closely to rule out fracture displacement.
-
After healing, the knee should be examined for ACL laxity.
References
1. Kocher
MS, Mandiga R, Klingele K, et al. Anterior cruciate ligament injury
versus tibial spine fracture in the skeletally immature knee: A
comparison of skeletal maturation and notch width index. J Pediatr Orthop 2004;24:185–188.
MS, Mandiga R, Klingele K, et al. Anterior cruciate ligament injury
versus tibial spine fracture in the skeletally immature knee: A
comparison of skeletal maturation and notch width index. J Pediatr Orthop 2004;24:185–188.
2. Meyers MH, McKeever FM. Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg 1959;41A:209–220; disc. 220–222.
3. Molander ML, Wallin G, Wikstad I. Fracture of the intercondylar eminence of the tibia: A review of 35 patients. J Bone Joint Surg 1981;63B:89–91.
4. Ishibashi
Y, Tsuda E, Sasaki T, et al. Magnetic resonance imaging aids in
detecting concomitant injuries in patients with tibial spine fractures.
Clin Orthop Relat Res 2005;434:207–212.
Y, Tsuda E, Sasaki T, et al. Magnetic resonance imaging aids in
detecting concomitant injuries in patients with tibial spine fractures.
Clin Orthop Relat Res 2005;434:207–212.
5. Kocher MS, Micheli LJ, Gerbino P, et al. Tibial eminence fractures in children: Prevalence of meniscal entrapment. Am J Sports Med 2003;31:404–407.
6. Lowe
J, Chaimsky G, Freedman A, et al. The anatomy of tibial eminence
fractures: Arthroscopic observations following failed closed reduction.
J Bone Joint Surg 2002;84A: 1933–1938.
J, Chaimsky G, Freedman A, et al. The anatomy of tibial eminence
fractures: Arthroscopic observations following failed closed reduction.
J Bone Joint Surg 2002;84A: 1933–1938.
7. Mulhall
KJ, Dowdall J, Grannell M, et al. Tibial spine fractures: An analysis
of outcome in surgically treated type III injuries. Injury 1999;30: 289–292.
KJ, Dowdall J, Grannell M, et al. Tibial spine fractures: An analysis
of outcome in surgically treated type III injuries. Injury 1999;30: 289–292.
8. Bong
MR, Romero A, Kubiak E, et al. Suture versus screw fixation of
displaced tibial eminence fractures: A biomechanical comparison. Arthroscopy 2005;21:1172–1176.
MR, Romero A, Kubiak E, et al. Suture versus screw fixation of
displaced tibial eminence fractures: A biomechanical comparison. Arthroscopy 2005;21:1172–1176.
9. Ahn JH, Yoo JC. Clinical outcome of arthroscopic reduction and suture for displaced acute and chronic tibial spine fractures. Knee Surg Sports Traumatol Arthrosc 2005;13:116–121.
10. Hunter RE, Willis JA. Arthroscopic fixation of avulsion fractures of the tibial eminence: Technique and outcome. Arthroscopy 2004;20: 113–121.
11. Ahmad
CS, Stein BE, Jeshuran W, et al. Anterior cruciate ligament function
after tibial eminence fracture in skeletally mature patients. Am J Sports Med 2001;29:339–345.
CS, Stein BE, Jeshuran W, et al. Anterior cruciate ligament function
after tibial eminence fracture in skeletally mature patients. Am J Sports Med 2001;29:339–345.
12. Senekovic
V, Veselko M. Anterograde arthroscopic fixation of avulsion fractures
of the tibial eminence with a cannulated screw: Five-year results. Arthroscopy 2003;19:54–61.
V, Veselko M. Anterograde arthroscopic fixation of avulsion fractures
of the tibial eminence with a cannulated screw: Five-year results. Arthroscopy 2003;19:54–61.
13. Horibe S, Shi K, Mitsuoka T, et al. Nonunited avulsion fractures of the intercondylar eminence of the tibia. Arthroscopy 2000;16:757–762.
Additional Reading
Accousti WK, Willis RB. Tibial eminence fractures. Orthop Clin North Am 2003;34:365–375.
Lubowitz
JH, Elson WS, Guttmann D. Part II: Arthroscopic treatment of tibial
plateau fractures: intercondylar eminence avulsion fractures. Arthroscopy 2005;21:86–92.
JH, Elson WS, Guttmann D. Part II: Arthroscopic treatment of tibial
plateau fractures: intercondylar eminence avulsion fractures. Arthroscopy 2005;21:86–92.
Codes
ICD9-CM
823.05 Avulsion of tibial spine
Patient Teaching
Activity
-
After injury, patients should be mobilized gradually.
-
Nonoperative treatment requires the leg to be left in extension for 4–6 weeks, followed by a gradual increase in knee motion.
-
Mobilization after surgery should be gradual and depends on the rigidity of fixation.
-
Often, a knee brace is used and flexion is increased gradually over time.
FAQ
Q: What is the risk of ACL laxity with need for ligament reconstruction?
A: With reduction of the fracture, the risk of ACL laxity is quite low. If the fracture is not reduced, the risk is much higher.