
Authors: Lewis, Steven L.
Title: Field Guide to the Neurologic Examination, 1st Edition
Copyright ©2004 Lippincott Williams & Wilkins
> Table of Contents > Section 2
– Neurologic Examination > Cranial Nerve Examination > Chapter 13
– Visual Field Examination
– Neurologic Examination > Cranial Nerve Examination > Chapter 13
– Visual Field Examination
Chapter 13
Visual Field Examination
PURPOSE
The purpose of the visual field examination is to assess
the function of the visual pathway that begins in the eyes and ends in
the occipital cortex, because lesions located along different regions
of this pathway produce characteristic visual field abnormalities.
the function of the visual pathway that begins in the eyes and ends in
the occipital cortex, because lesions located along different regions
of this pathway produce characteristic visual field abnormalities.
WHEN TO EXAMINE THE VISUAL FIELDS
Confrontational visual field testing is a quick and easy
way of discovering significant visual field loss, and it should be
performed on all patients as part of a standard neurologic examination.
way of discovering significant visual field loss, and it should be
performed on all patients as part of a standard neurologic examination.
NEUROANATOMY OF THE VISUAL FIELDS
The visual pathway is pictured in Figure 13-1.
The nasal (medial) part of each retina sees the temporal visual world,
and the temporal (lateral) part of each retina sees the nasal visual
world. Visual information from each retina travels through the optic
nerves into the optic chiasm. At the optic chiasm, the visual
information from the nasal part of each retina crosses to the other
side and continues as the optic tract, whereas the visual information
from the lateral part of each retina remains uncrossed, also continuing
as the optic tract. Each optic tract synapses in the lateral geniculate
nucleus. From the lateral geniculate nuclei, the visual information
continues onward toward the occipital cortex as the optic radiations.
Visual information from the lower retina (which sees the upper fields)
travels through the optic radiations that are located in the temporal
lobes, reaching the lower occipital cortex. Visual information from the
upper retina (which sees the lower fields) travels through the optic
radiations that are located in the parietal lobes, reaching the upper
part of the occipital cortex.
The nasal (medial) part of each retina sees the temporal visual world,
and the temporal (lateral) part of each retina sees the nasal visual
world. Visual information from each retina travels through the optic
nerves into the optic chiasm. At the optic chiasm, the visual
information from the nasal part of each retina crosses to the other
side and continues as the optic tract, whereas the visual information
from the lateral part of each retina remains uncrossed, also continuing
as the optic tract. Each optic tract synapses in the lateral geniculate
nucleus. From the lateral geniculate nuclei, the visual information
continues onward toward the occipital cortex as the optic radiations.
Visual information from the lower retina (which sees the upper fields)
travels through the optic radiations that are located in the temporal
lobes, reaching the lower occipital cortex. Visual information from the
upper retina (which sees the lower fields) travels through the optic
radiations that are located in the parietal lobes, reaching the upper
part of the occipital cortex.
EQUIPMENT NEEDED FOR THE VISUAL FIELD EXAMINATION
None.
HOW TO EXAMINE THE VISUAL FIELDS
-
Stand a few feet in front of the patient,
with your head at approximately the same level as the patient, looking
directly at the patient’s eyes. -
Instruct the patient to look at your nose
throughout the examination, and have the patient cover one eye with his
or her hand. Ask the patient to count the total number of fingers
you’ll be holding up. -
Check the visual fields by holding up
one, two, or five fingers in the vertical plane that is just between
you and the patient, checking each of the four quadrants. Test at least
four separate areas: the left and right upper visual fields and the
left and right lower visual fields. You do not need to hold the hands
far into the periphery, only approximately 1 ft away from the midline.
In most cases, you can quickly check both upper fields at the same time
(for example, by holding up one finger with your left hand and
P.44
two
fingers with your right hand, asking the patient to tell you the total
number of fingers you’re holding up), and then examine both lower
fields at the same time. If this is confusing to the patient, check
each quadrant separately.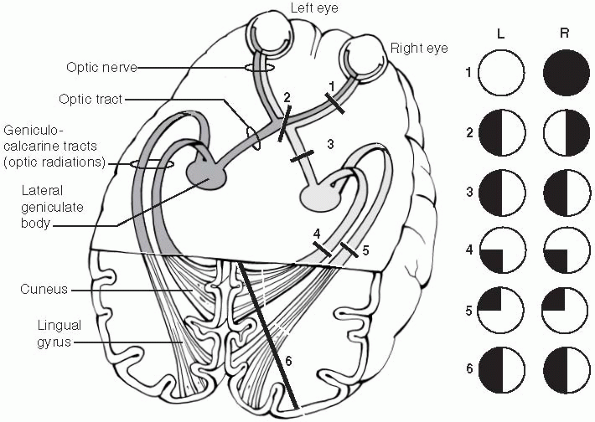 Figure 13-1
Figure 13-1
Illustration of the visual pathway from the eyes to the occipital
cortex. The characteristic visual field deficits that would occur due
to each of the numbered lesions at various regions of the visual
pathway are shown. See text for further details. (Redrawn from Gilman
S, Newman SW. Vision. In: Manter and Gatz’s essentials of clinical neuroanatomy and neurophysiology, 8th ed. Philadelphia: FA Davis Co, 1992:196.) -
Repeat the same process with the patient’s other eye closed.
NORMAL FINDINGS
Normally, patients should be able to count fingers in
all visual fields of each eye: the left upper quadrant, left lower
quadrant, right upper quadrant, and right lower quadrant.
all visual fields of each eye: the left upper quadrant, left lower
quadrant, right upper quadrant, and right lower quadrant.
ABNORMAL FINDINGS
-
An inability to count fingers in a visual field, or visual fields, is abnormal.
-
Visual field defects can occur from
dysfunction of the visual pathway anywhere from the eyes to the
occipital cortex. The typical visual field deficits that occur due to
lesions at different regions of the visual pathway are illustrated in Figure 13-1 and discussed below. -
Visual fields are characteristically
charted by drawing a circle representing the visual field of the left
eye and another circle representing the visual field of the right eye.
These are drawn as if you are the patient looking out: The left eye
field is drawn on the left and the right eye field is drawn on the
right. Intact visual fields are drawn as empty circles. Any abnormality
of a visual field is indicated by filling in that portion of the
P.45
circle.
Therefore, a patient with difficulty seeing in the left visual field of
both eyes would be drawn as shown for lesion 3 of Figure 13-1. -
Visual field deficits that involve one eye only are called monocular defects and occur due to dysfunction anterior to the optic chiasm, such as the optic nerve. Lesion 1 of Figure 13-1 shows a lesion of the right optic nerve causing right eye (i.e., monocular) blindness.
-
Bilateral temporal visual field defects
(bitemporal hemianopsias) occur from lesions at the optic chiasm, due
to dysfunction of the crossing fibers that arise from the nasal aspects
of each retina. Lesion 2 of Figure 13-1 shows a lesion at the optic chiasm causing a bitemporal hemianopsia. -
Visual field deficits that involve the same visual field of both eyes are called homonymous visual field defects
and are due to lesions posterior to the optic chiasm. Homonymous visual
field defects can involve one entire side of each eye (right or left
homonymous hemianopsias) or just the upper or lower quadrant (right or
left upper or lower quadrantanopsias). -
Homonymous visual field defects involving
an entire field (left or right homonymous hemianopsias) can arise due
to a lesion of the optic tract, both the upper and lower optic
radiations, or the occipital cortex. Lesion 3 of Figure 13-1 shows a left homonymous hemianopsia due to a lesion of the right optic tract. Lesion 6 of Figure 13-1 shows a left homonymous hemianopsia due to a lesion of the right occipital cortex. -
Homonymous quadrantanopsias occur due to
a lesion involving one of the (upper or lower) optic radiations or a
lesion involving just the upper or the lower part of the occipital
cortex. Lesion 4 of Figure 13-1 shows a left
lower quadrantanopsia due to a lesion of the right parietal optic
radiations, and lesion 5 shows a left upper quadrantanopsia due to a
lesion of the right temporal optic radiations.
ADDITIONAL POINTS
-
Despite its simplicity and the rapidity
with which it can be performed, confrontational visual field testing is
a sensitive screening test that can detect significant visual field
abnormalities produced by brain or optic nerve lesions. -
It is optimal to perform confrontational
visual field testing of each eye individually, especially so that
monocular field defects can be detected. For an even more rapid
screening test of a patient who has no visual symptoms, however, it is
occasionally reasonable to cheat by performing confrontational visual
field testing with both of the patient’s eyes open, although this would
not exclude monocular defects. -
Patients with nondominant (usually right) hemisphere lesions may exhibit a phenomenon known as visual field extinction, also called extinction on double-simultaneous stimulation.
These patients may have normal visual fields when asked to count
fingers in the left or right fields separately, but they may ignore the
left-sided stimuli when fingers are held up in both fields
simultaneously. This finding is particularly suggestive of a right
parietal lesion and is discussed further in Chapter 31, Examination of Cortical Sensation.