
Editors: Tornetta, Paul; Einhorn, Thomas A.; Damron, Timothy A.
Title: Oncology and Basic Science, 7th Edition
Copyright ©2008 Lippincott Williams & Wilkins
> Table of Contents > Section
II – Specific Bone Neoplasms and Simulators > 6 – Bone Sarcomas >
6.6 – Vascular Sarcomas of Bone
II – Specific Bone Neoplasms and Simulators > 6 – Bone Sarcomas >
6.6 – Vascular Sarcomas of Bone
6.6
Vascular Sarcomas of Bone
Hannah D. Morgan
Vascular sarcomas of bone are extremely rare tumors for
which the nomenclature is confusing, as there are a myriad of terms in
the literature describing a spectrum of malignant vascular lesions.
There are three major categories: hemangioendothelioma, a low-grade endothelial malignancy of bone; epithelioid hemangioendothelioma, a histologically distinct subgroup of endothelial malignancies; and angiosarcoma, high-grade vascular tumors of bone (Table 6.6-1).
The differential diagnosis, treatment, and prognosis of these lesions
vary according to the age of the patient, anatomic location(s) of
disease, and histologic grade of each tumor.
which the nomenclature is confusing, as there are a myriad of terms in
the literature describing a spectrum of malignant vascular lesions.
There are three major categories: hemangioendothelioma, a low-grade endothelial malignancy of bone; epithelioid hemangioendothelioma, a histologically distinct subgroup of endothelial malignancies; and angiosarcoma, high-grade vascular tumors of bone (Table 6.6-1).
The differential diagnosis, treatment, and prognosis of these lesions
vary according to the age of the patient, anatomic location(s) of
disease, and histologic grade of each tumor.
Pathogenesis
Etiology
A potential predisposing factor is external-beam radiotherapy.
P.207
|
Table 6.6-1 Comparison of Vascular Sarcomas of Bone
|
||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
P.208
Epidemiology
-
Extremely rare
-
<1% of primary bone sarcomas
-
Epithelioid sarcomas: <100 cases reported
-
-
If the tumor occurs after radiotherapy, the onset is typically several years following completion of the therapy.
Classification
-
Hemangioendothelioma: low-grade endothelial malignancy of bone
-
Epithelioid hemangioendothelioma: low- to intermediate-grade endothelial malignancy of bone (Fig. 6.6-1)
-
Angiosarcoma: high-grade endothelial malignancy of bone
Diagnosis
Clinical Features
-
Localized pain and occasionally soft tissue swelling
-
Angiosarcomas are more likely than others to present with pathologic fracture.
-
-
25% to 30% of patients with bony vascular
malignancies present with multicentric disease, either clustered in one
limb or other anatomic location (“skipping joints”) or spread
throughout the skeleton.-
Patient must be questioned about additional sites of bone pain.
-
Radiologic Features
-
Lesions may be single or multiple—look for multifocal disease with skeletal survey or bone scan.
-
Tumors are typically lytic but may be mixed lytic and sclerotic.
-
May see bony expansion, cortical thinning, or endosteal erosion on plain radiographs or computed tomography (CT) scan
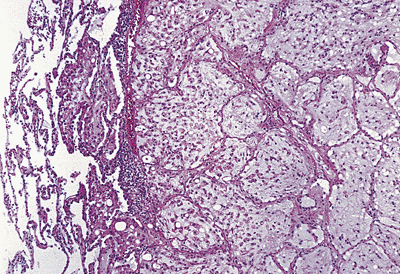 Figure 6.6-1 Metastatic epithelioid hemangioendothelioma. A nodule of tumor has spread within alveolar spaces. (From Rubin E, Farber JL. Pathology, 3rd ed. Philadelphia: Lippincott Williams & Wilkins, 1999.)
Figure 6.6-1 Metastatic epithelioid hemangioendothelioma. A nodule of tumor has spread within alveolar spaces. (From Rubin E, Farber JL. Pathology, 3rd ed. Philadelphia: Lippincott Williams & Wilkins, 1999.) -
Soft tissue mass is not usually a prominent feature of vascular bony malignancies.
-
Magnetic resonance imaging (MRI) shows marrow involvement and proximity of lesion to neurovascular structures.
Treatment
Surgical Indications and Contraindications
Surgical treatment of vascular bony malignancies depends
on the grade of the lesion (low, intermediate, or high), the anatomic
location of the tumor (whether it is surgically accessible or not), the
size of the lesion, and whether the lesion is solitary or multifocal.
on the grade of the lesion (low, intermediate, or high), the anatomic
location of the tumor (whether it is surgically accessible or not), the
size of the lesion, and whether the lesion is solitary or multifocal.
-
Hemangioendothelioma
-
Solitary and accessible: may be cured with surgical resection, with or without adjuvant therapy
-
Multifocal: typically treated with radiation therapy
-
Bisphosphonates may play a role when bone loss is significant.
-
-
Epithelioid hemangioendothelioma
-
Unifocal or localized multifocal lesions: should undergo wide resection when possible
-
If wide excision is not possible because
of patient factors or multifocal disease, chemotherapy, radiation
therapy, and radiofrequency ablation therapy have all been employed.
-
-
Angiosarcoma
-
Should be resected with a wide or radical surgical margin when disease and patient factors permit
-
Surgically inaccessible or multicentric lesions: radiotherapy has been employed
-
Effectiveness of chemotherapy has not been proved, although it is commonly used.
-
Preoperative Planning
Preoperative planning is as for other bone sarcomas (see Chapter 4, Treatment Principles).
Surgical Goals and Approaches
-
Ideally, lesion should be resected with wide margins.
-
Bony defect reconstruction (see Chapter 4)
Techniques
-
Resect and reconstruct according to principles of bone sarcoma surgery (see Chapter 4).
-
Amputation may be necessary for extensive multifocal disease or for tumors involving major neurovascular structures.
Complications
Results and Outcome
-
Hemangioendothelioma
-
Important prognostic variables: degree of tumor differentiation (grade) and multifocality (extent)
-
Multifocal tumors tend to be lower grade with better prognosis.
-
-
Overall the prognosis is good
-
Risk of recurrence: as much as 15%
-
In rare instances, tumor may metastasize.
-
-
-
Epithelioid hemangioendothelioma
-
Important prognostic variables: grade and extent (as above)
-
Intermediate risk of both local recurrence and metastasis, somewhat greater than that in patients with hemangioendothelioma
-
-
Angiosarcoma
-
High risk of local recurrence and metastasis
-
Long-term survival: 20%
-
Postoperative Management
The postoperative management of these tumors depends on the type of bony reconstruction performed after surgical resection (see Chapter 4).
Radiation therapy, when indicated, should be started when the wound is
healing satisfactorily, typically about 2 weeks following surgery.
Radiation therapy, when indicated, should be started when the wound is
healing satisfactorily, typically about 2 weeks following surgery.
Suggested Reading
Aflatoon K, Staals D, Bertoni F, et al. Hemangioendothelioma of the spine. Clin Orthop 2004;418:191–197.
Evans
HL, Raymond AK, Ayala AG. Vascular tumors of bone: a study of 17 cases
other than ordinary hemangioma, with an evaluation of the relationship
of hemangioendothelioma of bone to epithelioid hemangioma, epithelioid
hemangioendothelioma, and high-grade angiosarcoma. Hum Pathol 2003;34:680–689.
HL, Raymond AK, Ayala AG. Vascular tumors of bone: a study of 17 cases
other than ordinary hemangioma, with an evaluation of the relationship
of hemangioendothelioma of bone to epithelioid hemangioma, epithelioid
hemangioendothelioma, and high-grade angiosarcoma. Hum Pathol 2003;34:680–689.
Lezama-del Valle P, Gerald WL, Tsai J, et al. Malignant vascular tumors in young patients. Cancer 1998;83(8):1634–1639.
O’Connell JX, Nielsen GP, Rosenberg AE. Epithelioid vascular tumors of bone: a review and proposal of a classification scheme. Adv Anat Path 2001;8:74–82.
Wenger DE, Wold LE. Malignant vascular lesions of bone: radiographic and pathologic features. Skeletal Radiol 2000;29:619–631.