
Editors: Frassica, Frank J.; Sponseller, Paul D.; Wilckens, John H.
Title: 5-Minute Orthopaedic Consult, 2nd Edition
Copyright ©2007 Lippincott Williams & Wilkins
> Table of Contents > Triangular Fibrocartilage Complex Tear
Triangular Fibrocartilage Complex Tear
Barry Waldman MD
Dawn M. LaPorte MD
Description
-
The TFCC:
-
A group of ligaments and cartilaginous
structures that stabilize the distal radioulnar joint during pronation
and supination of the forearm -
Extends from the ulnar styloid to the sigmoid notch of the distal radius
-
Central portion:
-
More cartilaginous than its periphery
-
Acts as a meniscal homolog, similar to the menisci of the knee joint
-
-
-
Injury to the TFCC may result in acute or chronic wrist pain, often on the ulnar side.
-
A few wrists contain a true meniscus with a free edge that can be seen arthroscopically.
-
Synonym: Ulnar-sided wrist pain
Epidemiology
Incidence
-
Uncommon
-
Peak incidence: 30–60 years of age
Risk Factors
-
Jobs that require:
-
Repeated, loaded pronation and supination of the wrist
-
Heavy lifting
-
Etiology
-
Hyperpronation or dorsiflexion of the wrist may result in a tear of the TFCC, equivalent to a distal dislocation of the ulna (Fig. 1).
-
It may be associated with fracture of the distal radius or ulna or both.
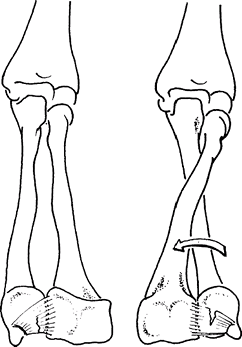 Fig. 1. TFCC tear may occur with forearm rotation.
Fig. 1. TFCC tear may occur with forearm rotation.
Signs and Symptoms
-
Most common complaint is ulnar-sided wrist pain, especially with repeated pronation and supination
-
Clicking
-
History of:
-
Hyperpronation or dorsiflexion injury to the wrist (acute cases)
-
Repeated pronation and supination (chronic cases)
-
Physical Exam
-
Localize the area of pain carefully (e.g., use the tip of the index finger to isolate the area of tenderness precisely).
-
Examine each joint of the wrist and hand for ROM and to detect crepitus, pain, or snaps.
-
TFCC compression test:
-
Provocative maneuver, for which elicited pain is a positive test
-
Axially load while rotating the ulnar-deviated wrist.
-
A click may reproduce the patient’s symptoms, causing pain.
-
-
Palpate the extensor carpi ulnaris while flexing and extending and while pronosupinating the wrist to rule out subluxation.
-
Assess the neurovascular status of the hand and forearm.
Tests
-
Arthrography of the wrist may be indicated.
-
A tear of the TFCC allows dye to extrude
into the radioulnar joint, which does not normally communicate with the
radiocarpal joint.
-
-
Some patients may require later injections of the distal radioulnar or midcarpal joint for full evaluation.
Imaging
-
Radiography:
-
AP and lateral radiographs of the wrist
-
Radiographs of the wrist in pronation and supination may be helpful in assessing radioulnar joint instability.
-
Ulnar height should be assessed on “0 rotation” views.
-
In the normal wrist, the distal radial and ulnar joint surfaces should be at the same level on the AP radiograph.
-
Positive variance of the ulna may result from fracture or instability of the distal radioulnar joint.
-
-
-
CT scan of both wrists in pronation and supination also can aid in diagnosis of instability.
Differential Diagnosis
-
Fracture of the radius, ulna, or any of the carpal bones
-
Rupture or tendinitis of the extensor carpi ulnaris, flexor carpi ulnaris, or the carpal ligament
-
Extensor carpi ulnaris subluxation
-
Arthritis of the ulnocarpal, pisotriquetral, or distal radioulnar joint
-
Lunotriquetral ligament injury
-
Ulnar artery thrombosis
-
Ulnar impaction syndrome
General Measures
-
Injury with fractures:
-
Reduce and immobilize the fracture.
-
Assess the distal radioulnar joint for reduction whenever distal forearm or wrist fractures are manipulated.
-
Acutely repair the TFCC when operative care of the fracture is indicated.
-
-
Injuries without fracture:
-
Try nonoperative treatment with a below-the-elbow cast in neutral rotation and analgesics for 6 weeks.
-
Slowly reintroduce gentle ROM when the cast is removed.
-
Patients with continued pain and instability may require additional assessment and subsequent operative repair.
-
Special Therapy
Physical Therapy
Patients with reduced ROM after TFCC injury or fracture may benefit from stretching exercises.
Medication
Analgesics are indicated.
Surgery
-
Repair of the ruptured TFCC can be attempted arthroscopically or with an open procedure if sufficient tissue is present.
-
Tears in the central area of the TFCC without instability may require arthroscopic débridement.
-
Variance of the ulnar height may need to be addressed through shortening of the ulna.
-
Reconstruction of the distal radioulnar joint with a tendon or band of fascia lata may be used to stabilize the joint.
-
In severe cases, with advanced radioulnar arthritis, fusion of the joint (Sauve-Kapandji procedure) may be considered (1).
P.471
Prognosis
-
The prognosis is fair to good.
-
Some persistent pain may occur even with adequate repair.
Complications
Posttraumatic arthritis can occur, often delayed by years or even decades.
References
1. Carter PB, Stuart PR. The Sauve-Kapandji procedure for post-traumatic disorders of the distal radio-ulnar joint. J Bone Joint Surg 2000;82B:1013–1018.
Additional Reading
Aulicino PL, Siegel JL. Acute injuries of the distal radioulnar joint. Hand Clin 1991;7:283–293.
Culp
RW, Osterman AL, Kaufmann RA. Wrist arthroscopy: Operative procedures.
In: Green DP, Hotchkiss RN, Pederson WC, et al., eds. Green’s Operative Hand Surgery, 5th ed. Philadelphia: Elsevier Churchill Livingstone, 2005:781–803.
RW, Osterman AL, Kaufmann RA. Wrist arthroscopy: Operative procedures.
In: Green DP, Hotchkiss RN, Pederson WC, et al., eds. Green’s Operative Hand Surgery, 5th ed. Philadelphia: Elsevier Churchill Livingstone, 2005:781–803.
Shih JT, Lee HM, Tan CM. Early isolated TFCC tears: Management by arthroscopic repair. J Trauma 2002;53:922–927.
Codes
ICD9-CM
842.00 Wrist pain
FAQ
Q: Do all TFCC tears need to be repaired?
A:
Partial tears may respond well to splint immobilization and
anti-inflammatory medicine or corticosteroid injection. Central tears
of the TFCC can be treated with arthroscopic débridement. Complete TFCC
tears and tears resulting in distal radial ulnar joint instability
require repair.
Partial tears may respond well to splint immobilization and
anti-inflammatory medicine or corticosteroid injection. Central tears
of the TFCC can be treated with arthroscopic débridement. Complete TFCC
tears and tears resulting in distal radial ulnar joint instability
require repair.
Q: How are TFCC tears repaired?
A:
An open repair is performed for a complete peripheral tear. If the
distal radial ulnar joint is stable, arthroscopic repair can be
considered.
An open repair is performed for a complete peripheral tear. If the
distal radial ulnar joint is stable, arthroscopic repair can be
considered.