
Editors: Frassica, Frank J.; Sponseller, Paul D.; Wilckens, John H.
Title: 5-Minute Orthopaedic Consult, 2nd Edition
Copyright ©2007 Lippincott Williams & Wilkins
> Table of Contents > Polydactyly
Polydactyly
Dawn M. LaPorte MD
John J. Hwang MD
Description
-
Polydactyly is a duplication of the fingers or toes that is detected at birth (Fig. 1).
-
Classification:
-
Preaxial (involving thumb or great toe, Fig. 2): Wassel classification (1):
-
I: Bifid distal phalanx
-
II: Duplicated distal phalanx
-
III: Bifid proximal phalanx
-
IV: Duplicated proximal phalanx
-
V: Bifid metacarpal
-
VI: Duplicated metacarpal
-
-
Central
-
Postaxial (involving small finger or toe) (2):
-
Type A: Complete duplication with bony attachment to an adjacent digit
-
Type B: Rudimentary, incomplete duplication of the phalanges
-
-
-
Synonyms: Accessory digits, Split thumb
Epidemiology
-
Postaxial form occurs at a rate of 1 per 150 in African Americans versus 1 per 1,500 in Caucasians (3,4).
-
Preaxial form is more common in whites than in other races (3,4), and most cases are sporadic.
-
Central polydactyly is uncommon compared with border polydactyly.
-
No significant difference in reported occurrence between the genders (3,4)
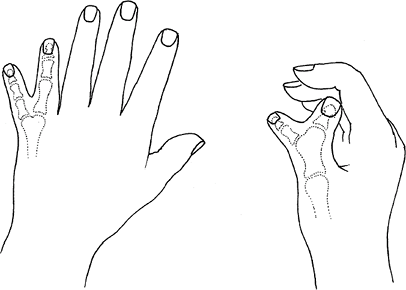 Fig. 1. Polydactyly involves variable skeletal duplications.
Fig. 1. Polydactyly involves variable skeletal duplications.
Risk Factors
African heritage is a risk factor.
Genetics
-
Postaxial polydactyly frequently is inherited as an autosomal dominant pattern but with variable penetrance.
-
Polydactyly of the index finger and polysyndactyly of the ring and long fingers probably are autosomal dominant conditions.
Etiology
The cause is unknown, unless the condition is associated with a syndrome.
Associated Conditions
-
Holt-Oram syndrome
-
Fanconi syndrome
-
Trisomy 13
-
Ellis-van Creveld syndrome
-
Grebe chondrodysplasia
Signs and Symptoms
Duplicated fingers or toes
Physical Exam
-
Check for active and passive movement at each joint.
-
Assess the stability of the digit.
-
Look for an angular deformity at each joint.
-
Look at the skin coverage and webbing.
-
All these factors are important in determining surgical treatment.
Tests
Imaging
Plain film radiography of the hand is indicated.
Pathological Findings
The digits may vary in the extent of development of the phalanges and tendons.
General Measures
-
Mild, type B postaxial polydactyly:
-
Treatment in the newborn:
-
Tie off the digit if it has no underlying skeletal connection.
-
In the presence of a skeletal connection, the “extra digit” should be electively removed surgically after 6 months of age.
-
-
This method is:
-
Safe
-
Not associated with bleeding complications
-
Associated with a satisfactory appearance
-
-
The rudimentary digit falls off in ~10 days.
-
-
Type A:
-
Requires operative ablation with transfer of any important parts to the adjacent finger.
-
Cosmetic concerns: Surgery is indicated to restore a normal appearance.
-
Polydactyly of the foot: Surgery often is needed to make normal shoe wear possible.
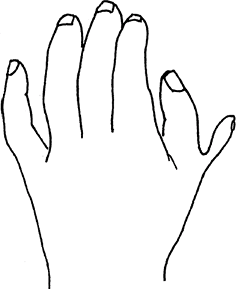 Fig. 2. Polydactyly is termed preaxial if it involves the thumb.
Fig. 2. Polydactyly is termed preaxial if it involves the thumb.
-
P.333
Surgery
Excision of the least developed digit, with preservation of the UCL and osteotomy, if indicated
Prognosis
-
Rudimentary, type-B postaxial polydactyly: Good
-
Other types of polydactyly (type A,
duplicated thumb): Possible risk of angular growth of the adjoining
digit or stiffness, but such problems rarely are symptomatic.
Complications
-
Small skin tag at the site of the polydactyly removal (rare)
-
Angular deformity possible after complex polydactyly reconstructions; possible “Z deformity” after thumb reconstruction
Patient Monitoring
For complex polydactyly, follow periodically with yearly checkups during growth.
References
1. Wassel HD. The results of surgery for polydactyly of the thumb. A review. Clin Orthop Relat Res 1969; 64:175–193.
2. Trumble
TE. Congenital hand deformities. In: Trumble TE, ed. Principles of Hand
Surgery and Therapy. Philadelphia: WB Saunders, 2000: 579–601.
TE. Congenital hand deformities. In: Trumble TE, ed. Principles of Hand
Surgery and Therapy. Philadelphia: WB Saunders, 2000: 579–601.
3. Frazier TM. A note on race-specific congenital malformation rates. Am J Obstet Gynecol 1960;80: 184–185.
4. Watson BT, Hennrikus WL. Postaxial type-B polydactyly. Prevalence and treatment. J Bone Joint Surg 1997;79A:65–68.
Additional Reading
Kozin SH. Deformities of the hand and fingers. Central polydactyly. In: Green DP, Hotchkiss RN, Pederson WC, et al., eds. Green’s Operative Hand Surgery, 5th ed. Philadelphia: Elsevier Churchill Livingstone, 2005:1393–1394.
Kozin SH. Deformities of the thumb. In: Green DP, Hotchkiss RN, Pederson WC, et al., eds. Green’s Operative Hand Surgery, 5th ed. Philadelphia: Elsevier Churchill Livingstone, 2005:1445–1468.
Kozin SH. Deformities of the hand and fingers. Ulnar polydactyly. In: Green DP, Hotchkiss RN, Pederson WC, et al., eds. Green’s Operative Hand Surgery, 5th ed. Philadelphia: Elsevier Churchill Livingstone, 2005:1392–1393.
Codes
ICD9-CM
-
755.0 Polydactyly (general)
-
755.01 Polydactyly (fingers)
-
755.20 Polydactyly (toes)
Patient Teaching
Inform patients with complex or preaxial polydactyly about the possibility of angular deformity of the thumb during growth.
FAQ
Q: If 1 child is born with polydactyly, is there an increased risk of it occurring in additional children?
A:
Postaxial polydactyly (ulnar side) frequently is inherited in an
autosomal-dominant pattern, but it has a variable penetrance pattern.
Postaxial polydactyly (ulnar side) frequently is inherited in an
autosomal-dominant pattern, but it has a variable penetrance pattern.
Q: Is the treatment for ulnar and radial polydactyly the same?
A:
No. Ulnar polydactyly frequently can be treated with surgical ablation,
whereas a duplicated thumb most often requires a more technical
reconstructive procedure with creation of a new ligament and possible
osteotomy.
No. Ulnar polydactyly frequently can be treated with surgical ablation,
whereas a duplicated thumb most often requires a more technical
reconstructive procedure with creation of a new ligament and possible
osteotomy.