
weight-bearing joint and may alter knee kinematics. Fractures range
from minimally displaced intra-articular injuries with minimal
soft-tissue embarrassment to fractures with significant soft-tissue
compromise, bicondylar and shaft involvement, and extensive articular
disruption. In an effort to preserve normal knee function, the
physician must strive to restore joint congruity, preserve the
mechanical axis, ensure joint stability, and restore knee motion. These
goals may be difficult to accomplish in the face of compromised soft
tissues, variable bone quality, and multiple medical comorbidities.
plateau fracture, the surgeon should individualize treatment with
respect to a variety of factors, such as the patient’s age, preexisting
levels of activity, medical conditions, and expectations. With regard
to injuries, the surgeon should consider the extent of fracture
comminution and joint impaction, associated injuries, and most
important, the condition of the soft tissue.
of low-energy tibial-plateau fractures varies widely among surgeons.
Numerous authors have reported satisfactory results using both
nonoperative and surgical methods for treatment of low-energy
tibial-plateau fractures in the elderly and others (1,2,3).
Low-energy tibial-plateau fractures that do not result in joint
instability, mal-alignment of the mechanical axis, or axial deformity
are best treated nonoperatively.
improve outcomes in the treatment of high-energy fractures,
particularly fractures that occur as a result of high-energy trauma
with severe soft tissue compromise in a young patient population. For
these complex fracture patterns, little controversy exists regarding
the need for operative management. Absolute indications for surgery in
these situations include open plateau fractures, fractures with an
associated compartment syndrome, and fractures with a vascular injury.
Relative indications for surgery include most displaced bicondylar
fractures,
displaced medial condyle fractures, coronal-plane posterior condylar
fracture-dislocations, and lateral plateau fractures that result in
axial joint instability (4–8).
reduction internal fixation (ORIF) is a compromised soft-tissue
envelope, which can occur in either open or closed fractures. For those
fractures, a ligamentotaxis reduction with the application of a
temporary external fixator is strongly recommended (7,8). Following the
resolution of soft tissue swelling, definitive open techniques that
decrease the risk of complications can be undertaken. The spectrum of
injuries to the tibial plateau is so great that no single method of
treatment has proven uniformly successful. However, by following the
principles of sound operative management, a congruous and stable knee
joint can be achieved.
presents with a painful, swollen knee and is unable to bear full weight
on the effected extremity. The magnitude of force delivered to the knee
determines the severity of fracture comminution, the amount of
articular impaction, and the degree of condylar and shaft displacement.
Therefore, the surgeon should determine whether the injury occurred as
the result of a high- or low-energy force.
integrity of the soft-tissue envelope particularly following
high-energy injuries. Superficial abrasions, deep contusions,
hemorrhagic blisters, and massive swelling indicate a severe
soft-tissue injury. The presence of some or all of these findings
precludes early ORIF techniques. If open wounds are present, their
relationship to the fracture site and the knee joint must be
ascertained. These areas should be avoided if a surgical approach is to
be undertaken (8).
and nerve function as well as the status of the compartments should be
evaluated and documented. Compartment pressure monitoring should be
done in many patients with high-energy fractures, especially displaced
medial plateau, bicondylar, and plateau fractures with shaft
dissociation.
ankle/brachial indices (ABI) should be obtained. ABIs consist of a
systolic blood pressure obtained at the palpated ankle over the
palpated posterior tibial artery and a systolic pressure obtained at
the elbow over the brachial artery. Under normal circumstances, the
ratio of ankle systolic pressure divided by brachial pressure should be
greater than 0.9. Values less than 0.9 are indicative of arterial
injury, and formal angiography is indicated to determine the level of
arterial disruption.
(AP) and lateral radiographs of the knee usually indicate a plateau
fracture. Routine radiographs should also include internal and external
oblique views. The oblique views often allow physicians to detect
subtle degrees of joint impaction or fracture lines not visible on the
AP or lateral views.
displaced fractures. Contemporary techniques require the surgeon’s
precise knowledge of the three dimensional anatomy of the fracture and
ligamentotaxis effect; therefore, use of distraction or traction films
is helpful in preoperative planning. Computed tomography (CT) scanning
with axial, coronal, and sagittal reconstructions is still the image
study of choice to delineate the extent and orientation of condylar
fracture lines as well as to determine the location and depth of
articular comminution and impaction. With low-energy fractures in
stable patients, the CT scan can be obtained in a routine preoperative
setting. However, for high-energy fractures that require early,
spanning, external fixation, the CT scan should be obtained following
the distraction treatment. Properly interpreted, CT scans can often
influence the choice of surgical approach, including the location of
surgical incisions and the insertion points of percutaneous plates
and/or screws (8) (Fig. 26.1).
 |
|
Figure 26.1. A1–3.
AP, lateral, and oblique injury x-rays demonstrating a bicondylar fracture pattern. Because of displacement and mal-alignment, the fracture morphology is not clearly seen. B. A traction radiograph restores length and allows identification of fracture components. C. A traction CT scan demonstrating the fracture morphology. Traction accomplished a near anatomic alignment of medial and lateral condyles, shaft axis alignment, and identified avulsion of the intracondylar eminence. |
injuries that can occur with tibial plateau fractures, magnetic
resonance imaging (MRI) scans can be very helpful. MRI has been shown
to be superior to CT scans in assessing soft-tissue injuries. In
addition to delineating the fracture and possible meniscal pathology,
MRI can detect associated soft-tissue lesions such as tears of the
medial collateral ligament or anterior cruciate ligament, which are
often seen with lateral plateau fractures. Likewise, tears of the
lateral collateral or cruciate ligaments associated with fractures of
the medial plateau can be detected through this imaging modality (Fig. 26.2) (9,10).
 |
|
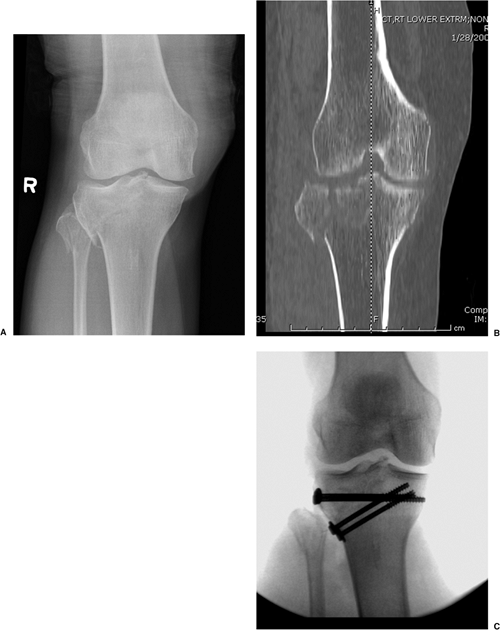
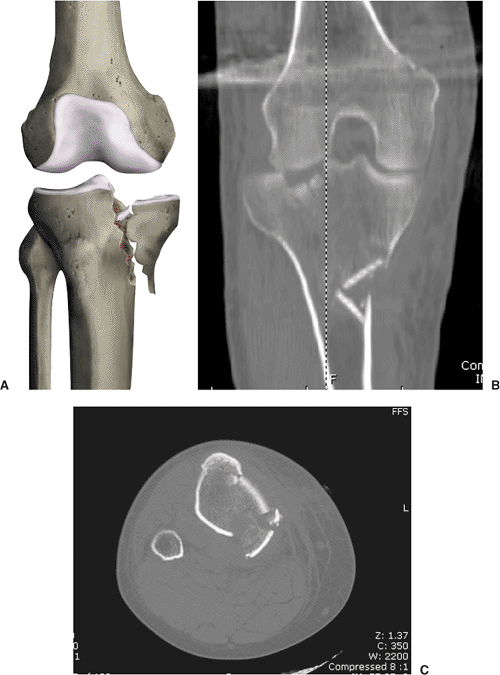
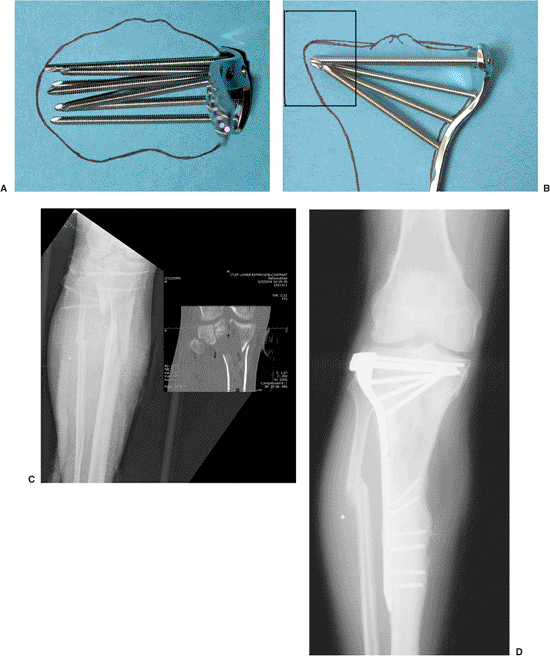
Figure 26.2. A. AP view of Schatzker type III fracture with demonstrated lateral articular impaction. B. CT scan demonstrates orientation and depth of articular impaction. C. MRI demonstrates not only depth of articular impaction but also denotes peripheral lateral-meniscal tear (square).
|
the proper implants, reduction tools, bone graft (or bone graft
substitutes), and fluoroscopic equipment are available for the surgical
procedure.
Schatzker classification in which these injuries are divided into six
distinct subtypes and associated treatment principles (6). In addition,
dividing these fractures into low-energy versus high-energy injuries
may help in determining the initial degree of soft-tissue compromise
(8). Depressed articular fragments will not reduce by manipulation,
traction, or ligamentotaxis techniques alone. If articular impaction
and subsequent defects are sufficient to produce axial joint
instability or mechanical axis deviation with weight bearing, the joint
surface should be surgically elevated and supported with graft material
and fixation hardware (6). Therefore, the surgical tactic and location
of incisions must optimize exposure and reduction techniques.
articular depression or step off that dictates nonoperative or surgical
treatment. Long-term studies with greater than 20-year follow-up have
shown an inconsistent relationship between residual osseous depression
of the joint surface and the development of osteoarthrosis. However, if
joint deformity or depression produces knee instability, the likelihood
of a poor outcome is significantly increased (2,3). When forming the
goals of surgery, the physician must address the factors that are
thought to determine outcomes:
-
integrity of the soft tissue envelope,
-
the degree of articular depression,
-
the extent of condylar separation or widening, and
-
the degree of diametaphyseal comminution and shaft dissociation association.
spinal anesthesia positioned supine on a radiolucent operating table.
Some surgeons prefer a table that has the ability to break so that the
knee can be flexed to approximately 90 degrees. We prefer a large
bolster or a bean bag patient positioner to elevate the operative
extremity when placed under the ipsilateral hip; it allows the knee to
be flexed to 90 degrees intraoperatively. A C-arm image intensifier is
positioned on the contralateral side. Trial images should be obtained
prior to prepping and draping to ensure that accurate AP, lateral, and
oblique fluoroscopic images are easily attainable without interference.
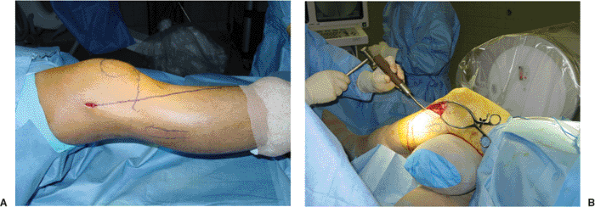
The entire extremity is then prepped and draped from toes to groin. If
an iliac crest bone graft is planned, then the ipsilateral crest is
also included in the initial prep and a sterile tourniquet is utilized (Fig. 26.3).
profile sizes, which are precontoured to match the proximal tibial
condylar anatomy. The large 4.5-mm and 6.5-mm implants are used less
frequently today. Peri-articular plates require less exposure than do
their predecessors. Because the majority of plateau fractures involve
the lateral condylar surface, a variant of a lateral parapatellar
incision is most commonly used for most lateral plateau fractures. This
incision can be utilized at its proximal extent to expose only the
lateral condyle, but it can also be easily extended proximally and
distally when more exposure is needed, such as in an Schatzker V or VI
injury.
of the medial fracture line determines the location of a possible
medial incision. Thus a medial or posteromedial incision may be
necessary when treating specific, isolated, medial condylar (Schatzker
IV) or bicondylar fracture patterns. With fracture dislocations of the
medial condyle in the coronal plane (1), the apex of the fracture line
is sometimes oriented directly posterior. In these cases, a direct
posterior exposure may be required for fracture stabilization (11).
 |
|
Figure 26.3. A,B.
Position of knee in the operating room. The knee is elevated using a sterile bolster to allow flexion to at least 90 degrees. The ability to achieve 360-degree fluoroscopic visualization is mandatory. |
A preoperative MRI should be obtained to assess the integrity of the
lateral meniscus. If the meniscus is intact, a closed reduction and
percutaneous fixation with cannulated screws or noncannulated cortical
screws may be performed (9). Applying longitudinal traction with a
varus force may improve the reduction. As an alternative, a laterally
based femoral distractor can be used to restore length and alignment
through ligamentotaxis. When an acceptable reduction is obtained, the
fracture is held with a large pointed forceps placed percutaneously on
the medial and lateral condyles to compress the fracture line. Fixation
is usually accomplished with two or three 6.5- or 7.0-mm screws placed
through small stab incisions, or occasionally through use of multiple
3.5-mm cortical screws (12). The orientation of these screws should be
determined preoperatively and based either on the MRI or CT scan (Fig. 26.5).
meniscal tear or incarceration of the meniscus within the vertical
fracture line, or if a closed reduction fails to reduce the fracture
adequately, ORIF with meniscal repair or excision is indicated.
apposition (i.e., bone on bone stability following reduction) is not
found, a laterally directed buttress or antiglide plate should be used
instead of solitary, multiple, lag screws.
Preoperative imaging studies are important to determine the degree and
location of articular impaction as well as the orientation of the apex
of the condylar fracture line. In most cases, the depression is
anterior or central and is best approached through an anterolateral
incision. The joint surface is visualized through a submeniscal
arthrotomy. The lateral menisco-tibial ligament is incised
transversely, allowing elevation of the meniscus through the use of
several small traction sutures or small angled retractors (Fig. 26.7). A varus stress is applied to open the joint line for visualization of the articular surface of the lateral plateau.
degrees, which allows additional visualization of the joint surface
because the joint is distracted via the weight of the leg.
Alternatively a femoral distractor can be used to enhance joint
visualization through sustained distraction.
different techniques. In one method, the condylar fracture line is
wedged open like a book. The articular depression is directly
visualized and an impactor is inserted from below to disimpact and
elevate the
osteochondral
fragments. Once the articular fragments have been repositioned in a
congruent fashion, provisional Kirschner (K) wires are used to
temporarily stabilize the joint. The elevated osteochondral fragments
create a metaphyseal defect that requires support prior to reduction of
the condyle. This support is accomplished through placement of graft
material beneath the reduced fragment into the subchondral void. Many
alloplastic calcium phosphate and sulfate materials are now available
for use as substitutes for autograft bone in grafts (13,14). Following
graft placement, the split condyle is reduced and held with large
reduction forceps (Fig. 26.8). Fixation of the condyle is achieved with a peri-articular plate or lag screws.
 |
|
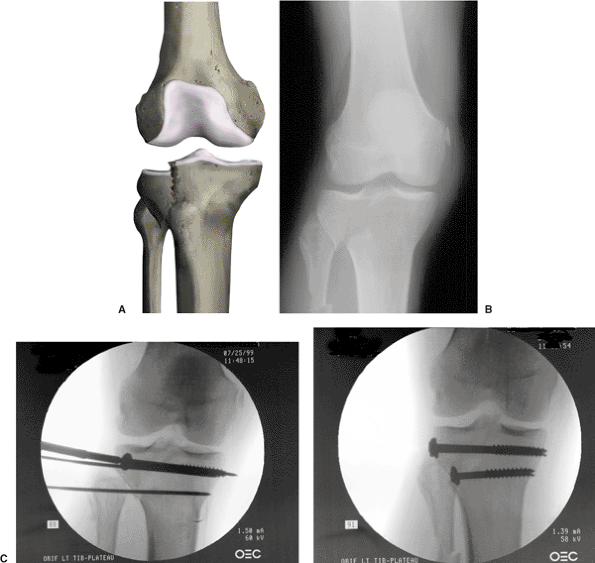
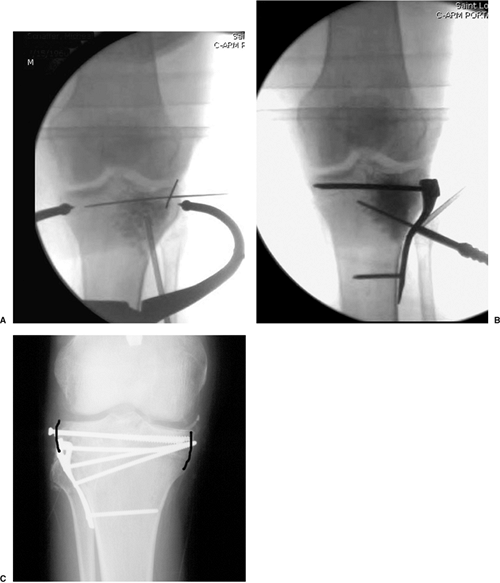
Figure 26.4. A. Schatzker type I fracture: split lateral tibial–condyle fracture without articular impaction. B. X-ray demonstrating Schatzker type I injury. C,D.
Closed reduction accomplished with distraction and varus stress. Guide wires are advanced, followed by cannulated screw fixation. The inferior screw acts as an antiglide washer at apex of fragment. |
 |
|
Figure 26.5. A. AP x-ray demonstrating a solitary split in the lateral condyle. B.
CT scan reveals a sagittal split in the lateral condylar fragment. CT information aids in the orientation of percutaneous screw placement. C. Fixation is accomplished percutaneously with small fragment screws and washers functioning as small antiglide plates. |
 |
|
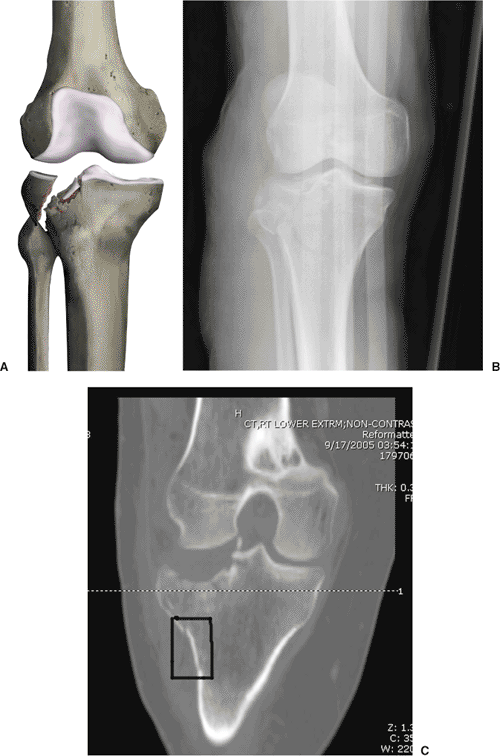
Figure 26.6. A.
Schatzker type II injury: Comminution and impaction of the lateral articular surface occurs with a large wedge fracture of the lateral tibial condyle. B,C. AP radiograph and CT scan demonstrating the depth and orientation of articular impaction as well as the segmental, lateral-condylar, fracture lines (square). This information helps the surgeon determine the length of the incision. |
 |
|
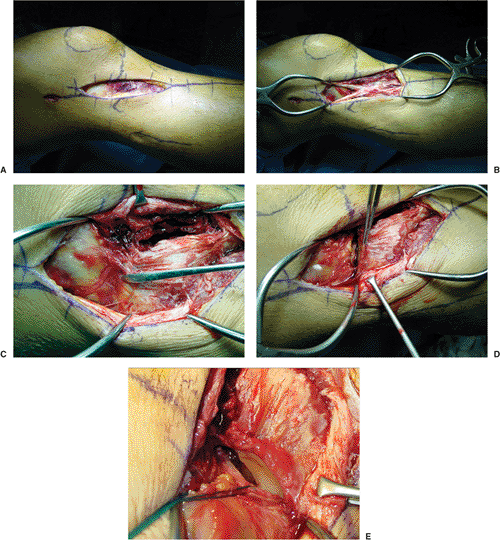
Figure 26.7. A.
Standard, lateral, utility incision: The incision begins 1 to 2 cm proximal to the joint line along the midaxillary line in the midportion of the fascia lata. It is carried distally over Gerdy’s tubercle and gently angled toward the lateral border of the anterior tibial crest. The incision can be extended proximally or distally as necessary. B. The fascia lata is split (retracted for demonstration) in the midline and centered over Gerdy’s tubercle. The anterior compartment fascia is incised in continuity just lateral to the anterior tibial crest. C. Retracting the anterior (clamp) and posterior portions of the fascia lata expose the major fracture line and capsular structures. The meniscal tibial ligament is identified (elevator). D. The menisco-tibial ligament has been incised below the level of the lateral meniscus. The tibial attachment of the ligament is preserved (forceps) to facilitate repair of the peripheral meniscal tear (just proximal to forceps, tear is visible). E. Sutures are attached to the meniscus and proximal capsule to facilitate meniscal retraction. The submeniscal arthrotomy allows direct joint visualization. Articular impaction, in continuity with the major fracture line, is visible. |
 |
|
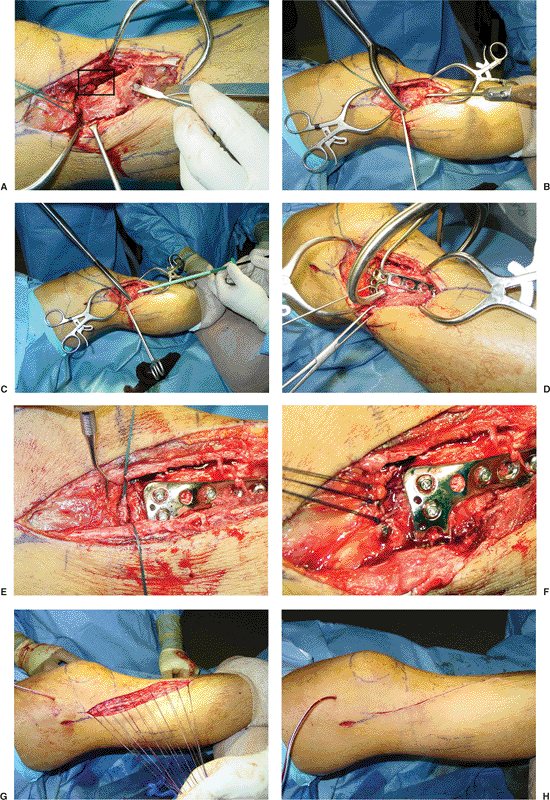
Figure 26.8. A.
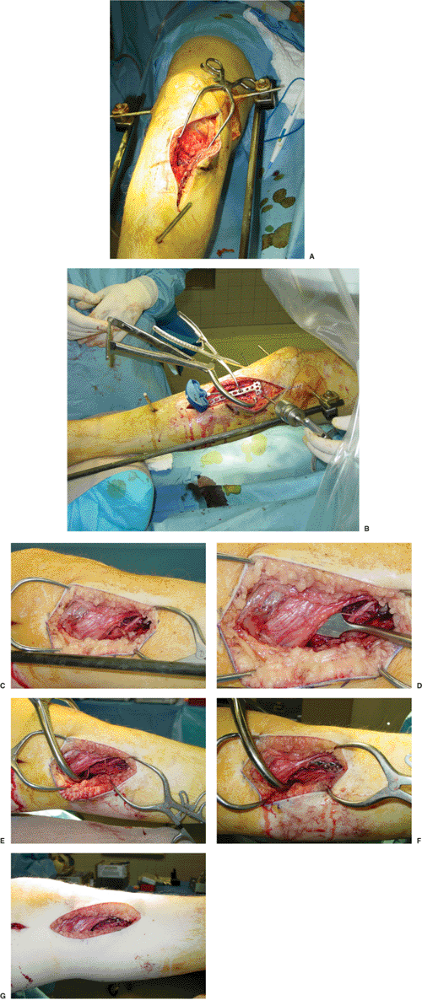
The proximal portion of the anterior compartment musculature is minimally reflected from the lateral condyle so access is gained to the condylar flare. The major fracture line can be gapped open to gain direct access to the articular impaction through the fracture line (square); this technique allows for joint elevation. In an alternative approach, a subcondylar window can be fashioned with multiple drill holes and a small osteotome. B. The condyle is reduced and compressed with a large reduction clamp placed percutaneously in the medial and lateral condyle. A curved impactor is used to elevate the depressed articular surface. C. The subchondral void is filled with an alloplastic bone-graft substitute, which can be applied in an indirect fashion (injected). The surface is continuously elevated until congruency is achieved. D. A precontoured plate is advanced distally in a submuscular fashion. The plate is held in place with large pointed forceps and temporary K wires. E. Following application of fixation hardware, the peripheral meniscal tear (sutures) is repaired to the capsule. F. The submeniscal arthrotomy is closed by suturing the meniscal-tibial ligament. G. The fascia lata is closed over suction drains. H. Skin closure is accomplished without tension. |
subchondral region as “raft screws.” These horizontally directed screws
should capture the intact medial cortex. The screws are supported on
either side of the impaction by the intact lateral and medial cortices,
much like I beams support horizontal rafters on a roof. These raft
screws help support the elevated articular surface and prevent late
subsidence (Fig. 26.9) (5). The surgeon should carefully repair the menisco-tibial ligament and meniscal tears when present.
reduced first and held with the large, pointed, reduction forceps. Once
the condylar fracture lines have been reduced, the impacted articular
surface is addressed indirectly. A 1-cm cortical window in the
subcondylar flare is fashioned by connecting multiple, small drill
holes with a small osteotome. The cortex is impacted directly into the
metaphysis using a small curved impactor. Under fluoroscopic guidance,
the impactor is directed to engage from below the depressed
osteochondral fragment. The surgeon must disimpact and elevate the
fracture fragments en masse by placing graft material continuously
beneath the fracture fragment. The pressure from the impactor
distributed over a relatively large surface area minimizes
fragmentation or splitting of the articular surface. The joint surface
is slowly elevated as visualized indirectly by fluoroscopy or directly
through the submeniscal exposure. Once articular congruency has been
reestablished provisional K wire fixation is utilized. A peri-articular
or percutaneous plate with raft screws can be passed directly through
the proximal aspect of the incision and distal screws applied through
small percutaneous stab wounds (see Fig. 26.8).
occur after a low-energy valgus-stress injury in elderly patients with
osteoporotic bone. The articular surface of the lateral plateau is
impacted without an associated lateral condylar fracture. A
preoperative MRI or CT scan will specifically locate the area of
impaction and orientation of the impacted osteochondral fragments. In
additional, MRI is helpful in identifying meniscal pathology or
incarceration of the meniscus within the depressed articular surface.
less invasive than it has been in the past. This fracture is now
treated with small incisions made while the surgeon uses an image
intensifier or arthroscopic visualization of the articular surface (Fig. 26.10).
A small lateral incision is made over the metaphyseal region of the
lateral condyle, and exposure is limited to develop a small,
subcondylar, metaphyseal, cortical window. This exposure can also be
developed in percutaneous fashion. The window must be of sufficient
size to allow grafting and elevation of the fragment from below and the
surgeon to assess the reduced surface from above or through
arthroscopic visualization. Once reduction of the joint is confirmed,
the graft is stabilized by percutaneous raft screws placed in a
subchondral location (12,15). As an alternative, cannulated screws can
be utilized.
 |
|
Figure 26.9. A. Fluoroscopic visualization shows articular surface elevation and graft placement. B.
Raft screws are placed through the proximal portion of the plate, capturing the intact medial cortex and thus providing support for the elevated articular surface. C. Solitary raft screws placed in a subchondral location support the articular surface. The screws are supported by the reconstructed lateral cortex and the intact medial cortex (black lines). |
 |
|
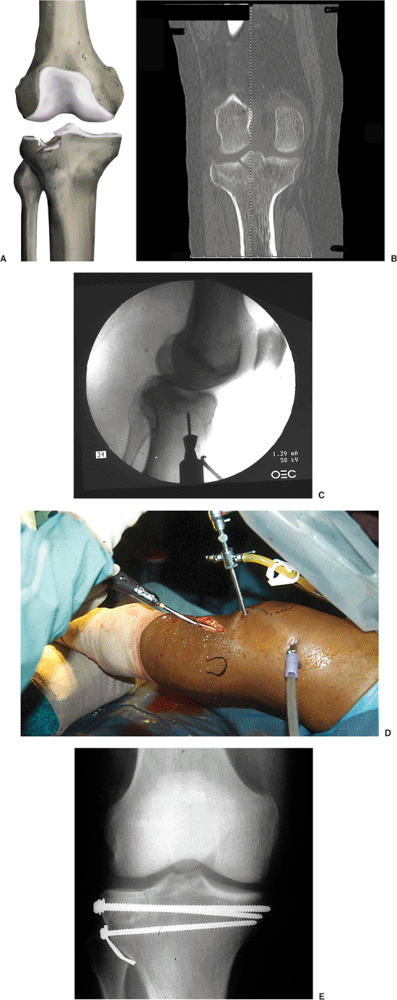
Figure 26.10. A. A Schatzker type III injury involves impaction and comminution of the lateral articular surface. B.
CT scan of Schatzker type III injury that demonstrates central impaction of the lateral articular surface and preservation of an intact lateral-condylar rim. This particular pattern is amenable to arthroscopic-assisted fixation. C. A subchondral window is produced through the use of a cannulated drill with guide wire localized via arthroscopic visualization. D. The articular surface is elevated through use of a bone impactor followed by percutaneous raft-screw fixation. E. Follow-up x-rays demonstrate healed subchondral surface and maintenance of fracture reduction. |
usually caused by high-energy trauma and are often associated with
neurovascular injuries and significant fracture displacement. They
frequently occur with other injuries, such as knee dislocations with
ligamentous disruption. A high index of suspicion is necessary to avoid
overlooking a limb-threatening injury with this fracture pattern. In
fractures with minimal comminution or displacement, closed reduction
can be attempted with large reduction forceps. Successful fixation
through use of multiple percutaneous screws is usually sufficient.
However, most medial plateau fractures are grossly unstable with
comminution in the
region
of the intercondylar eminence and at the distal apex of the condylar
fragment (6). For comminuted fracture patterns, a buttress plate rather
than lag screws are needed. When the intercondylar eminence is avulsed
and includes the anterior cruciate ligament, percutaneous treatment is
contraindicated (Fig. 26.11).
apex of the medial-condylar fracture line. The location is highly
variable and may be directed posteriorly, posteromedially, medially, or
anteromedially. The orientation and location of the medial fracture
line dictates
the
location of the surgical incision. To improve the surgical exposure, a
preoperative CT evaluation is imperative so the surgeon can place the
incision as close to the apex of the major condylar fracture line as
possible.
 |
|
Figure 26.11. A.
In Schatzker type IV injuries, the medial condyle fracture is often associated with intracondylar comminution and fragmentation. B. Coronal reconstruction demonstrates comminution at the intercondylar eminence and involves the lateral articular surface, which must also be addressed through surgery. C. Transverse CT cuts reveal that the apex of the medial condylar fracture is directed posteromedially. Therefore, the incision should be directed in this region and the plate positioned along the posteromedial tibial border. |
plate located over the apex of the condylar fracture line. An
anteromedial fracture location requires that the anterior pes anserine
tendons be posteromedially reflected in continuity with the superficial
portion of the medial collateral ligament. The plate lies in contact
with the entire metaphyseal surface without entrapping the underlying
soft tissue. If the apex is more medially directed, the inferior margin
of the pes can be reflected anteriorly and a plate positioned on the
posteromedial aspect of the tibia anterior to the medial gastrocnemius
muscle (Fig. 26.12).
the knee, a direct exposure of the posterior medial condyle is
accomplished through a posterior approach. The patient is placed prone
and a direct medial incision is placed along the posteromedial border
of the proximal tibia. The exposure is accomplished by lateral
retraction of the medial gastrocnemius and popliteus muscles. This
provides direct visualization of the entire posterior aspect of the
proximal tibia and facilities direct application of a posterior plate (Fig. 26.13) (11).
types V and VI are usually the result of high-energy forces that may
compromise the surrounding soft tissues (Fig. 26.14).
A staged approach is usually required for successful treatment of these
injury patterns (5,7,8). Bridging external fixators should be applied
rapidly to restore length and stability. Distraction CT or MRI scans
are much more valuable after application of a bridging external
fixator. Careful preoperative planning is required and definitive
surgery is not undertaken until the soft tissues have recovered. In
many cases, surgery may be delayed for 2 or 3 weeks while soft tissues
heal (Fig. 26.15).
implants, the necessity for extensile exposure of the upper tibia can
be minimized. The routine use of both a medial and lateral plate has
also decreased because of the development of locking plates, which
allow the stabilization of many medial-condylar fragments from the
lateral side alone. In addition, many of these newer implant systems
are designed for percutaneous insertion and thus extensile approaches
can be avoided.
and the shaft is displaced from the metaphysis. Many locked-plating
systems can stabilize the metaphyseal diaphyseal fracture through
indirect percutaneous techniques in which one or two femoral
distractors maintain the reduction. Large, percutaneously applied,
reduction forceps may reduce or improve the position of the
intercondylar fracture lines. Based upon preoperative imaging studies,
articular impaction is elevated through the surgeon’s use of cortical
windows placed either medially or laterally in the subcondylar regions.
proximal aspect of the lateral condyle. Cannulated or 3.5-mm screws can
be used to secure the intercondylar reduction after which the condyles
must be attached to the tibial shaft. If the soft tissues allow, a
locking plate can be slid in a submuscular fashion along the lateral
aspect of the shaft. The locking plates are designed to bridge the zone
of comminution at the diametaphyseal junction. Many of these implant
systems have outriggers that are used to place screws into the distal
portions of the plate via small percutaneous incisions (Fig. 26.16)
(16). If the condylar fracture fragments are not comminuted and the
condyles are well reduced, the medial condyle can be controlled with a
laterally based locking plate with locked screws. However, coronal
splits of the posterior aspect of the medial condyle cannot be
stabilized with a lateral plate alone and require independent fixation.
Little data are available to assess accurately the performance and
ability of these locking plates to prevent varus deformities of the
medial condylar fragment. If anatomic cortical contact can be obtained
following reduction, then a laterally based locking plate can be used
to maintain both the lateral and medial condylar reduction. However, if
the apex of the medial condyle is comminuted or located posteriorly,
then this fragment requires support to prevent late varus deformity.
This stability is accomplished by placement of an extra periosteal
antiglide buttress or small locking plate. A locking plate on the
medial side can
be
placed with the use of unicortical locking screws. The implant is
placed at the apex of the medial tibial condyle as determined by
preoperative CT scan. Care should be taken to limit dissection through
the second incision and to avoid creation of large skin flaps (Fig. 26.17).
 |
|
Figure 26.12. A.
The medial exposure is directed at the medial aspect of the tibia at the apex of the medial condyle fracture (comminution at the base of the medial fragment determines the location of plate). B. Reduction is accomplished with large reduction forceps and a Schantz pin used as a joystick. A trocar is used to insert the bone graft substitute. The plate is positioned directly at the apex of the condylar fracture, bridging the area of comminution. C,D. A posteromedial incision is located just posterior to the medial tibial border. The inferior edge of the pes is mobilized, and the interval between the medial gastrocnemius is mobilized (elevator). E–G. The apex of the fracture is localized and reduction forceps are placed percutaneously to reduce the medial condyle. A contoured plate is then advanced along the medial condylar flare in an extraperiosteal fashion. Following screw application, the surgeon allows the pes to cover the plate, and the wound is easily closed. |
|
Figure 26.13. A. Sagittal CT cuts reveal a posteriorly directed medial-condyle fracture. B.
The apex of the fracture line is directly posterior. This placement precludes use of lag screw fixation from front to back. A posterior buttress plate is required to maintain the reduction. C. Direct posterior approach allows the surgeon to retract the medial head of the gastrocnemius (under retractor) laterally, exposing the soleus and posteromedial border of the tibia. D. The soleus muscle is incised along the medial border of the tibia and then retracted laterally exposing the posterior fracture lines. E. A buttress plate is applied directly to the posterior tibia the posterior capsule, which can also be incised to allow limited visualization of the joint. F1,2. A reconstruction plate is contoured to buttress the posterior fracture line. G. A small T plate is directed posteriorly to prevent displacement of this unstable condylar fracture. |
 |
|
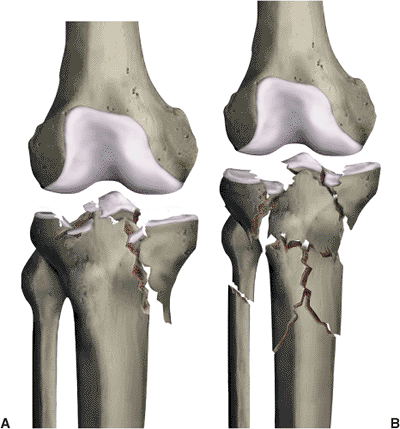
Figure 26.14. A. A Schatzker type V fracture pattern involves both condyles with lateral joint impaction (high-energy fracture pattern). B.
This Schatzker type VI fracture involves both condyles as well as complete dissociation of the metaphyseal region from the shaft. |
 |
|
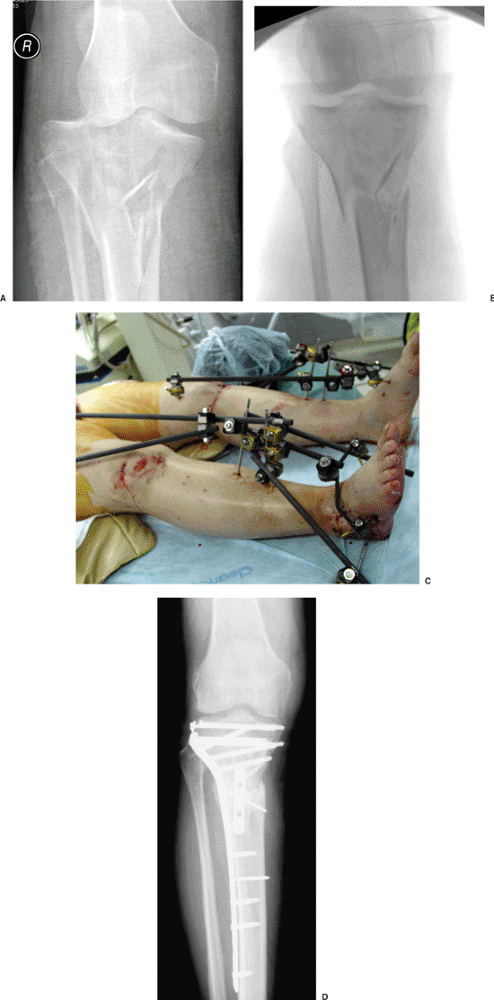
Figure 26.15. A. A high-energy fracture with bicondylar and shaft involvement. B.
Immediate application of a temporary external fixator via ligamentotaxis realigns the metaphyseal condylar fragments as well as the shaft dissociation. C,D. Bilateral high-energy plateau fractures are shown in a polytrauma patient who has spanning external fixators bridging both knees to allow soft-tissue recovery. Definitive fixation was accomplished with a limited lateral approach to reconstruct the lateral condyle. The shaft extension was spanned successfully through use of percutaneous application of a locking plate that also supported the medial condyle. |
 |
|
Figure 26.16. A,B.
Locking plates perform the raft function by supporting the subchondral reconstruction with multiple parallel screws spanning the fracture from lateral plate to medial cortex. Because of the locking function and orientation of all metaphyseal screws, potential varus deformity of the medial condyle is decreased (square). Many of these plates have outriggers that allow shaft screws to be applied in a percutaneous manner. C,D. Complex Schatzker VI fracture treated with a long peri-articular locking plate healed without varus deformation. The shaft extension was stabilized without direct exposure because the surgeon placed the distal screws via a percutaneous approach with an outrigger device. |
present, additional incisions are contraindicated to avoid wound
problems, and a ring fixator is indicated for stabilization of these
complex injuries. It cannot be overemphasized that when extreme
soft-tissue compromise is present, formal or even limited open
reduction and plate osteosynthesis should be abandoned in favor of
small tension wire or hybrid external-fixation techniques.
dressing from the toes to groin. A cephalosporin is administered for 24
to 48 hours after surgery. A suction drain is maintained for at least
24 hours or until drainage is less then 30 mL per 8 hour interval.
damaged at the time of injury and wound closure was achieved without
tension, a continuous passive motion (CPM) machine is recommended. If
significant swelling or tension on the suture line is present the CPM
is delayed until the swelling has subsided. The bulky dressing is
removed at 48 hours and a hinged knee brace that allows gradual
increase in range of motion is applied. If a meniscal
tear
was present and repaired, the range of motion is usually limited for
the first 3 weeks with flexion stops at 60 degrees. This protects the
peripheral meniscal rim and allows early healing prior to initiation of
full, unrestricted range of motion.
 |
|
Figure 26.17. A. X-ray following application of a spanning external fixator for a high-energy plateau fracture with bicondylar involvement. B.
Distraction CT demonstrating bicondylar involvement. The scan also helps localize proposed incision for medial condylar fixation. C. The lateral condyle is approached through a standard lateral approach, allowing reduction and elevation of the depressed joint surface through this incision. D. The medial incision is located based on CT data. The plate is located between the pes anserine and medial gastrocnemius. Although the incision is sizable, soft-tissue stripping is minimized. E. Large reduction forceps are used to manipulate the bicondylar fracture line and to compress the plates to bone for secure fixation. F,G. A lateral contoured plate is advanced in submuscular fashion with distal screws placed in percutaneous fashion. The medial condyle was stabilized with a small reconstruction plate and unicortical locking screws. |
strengthening as well as non–weight-bearing gait training with crutches
or a walker. Patients are seen at 2 weeks for suture removal and at
monthly intervals thereafter. Once the wound is healed, active and
active-assisted range of motion is initiated. The goal is to achieve at
least 90 degrees of knee flexion by the 4th week after surgery. Weight
bearing of up to 50% of body weight is initiated at 8 to 12 weeks if
radiographic evidence show subchondral healing, metaphyseal
consolidation, and incorporation of the subchondral void; this evidence
is especially important when bone graft or bone graft substitutes have
been utilized to fill the subchondral defect.
bearing must be delayed for 10 to 12 weeks. In low-energy injuries,
patients can usually bear full weight by 12 to 14 weeks. Most patients
can expect to resume most simple activities between 4 to 6 months.
Running and vigorous athletic activities are often delayed up to 1 year
after injury. The patient and surgeon alike can expect a good,
functional outcome for most type I, II, and III injuries.
metaphyseal-diaphyseal junction in the type V and VI injuries, the
fracture is often slow to consolidate. If union is not progressing, the
area should be bone grafted before initiation of weight bearing. The
timing of the bone graft is based on the status of the soft tissues.
Grafting at 8 to 12 weeks is usually safe. Patients with Schatzker V or
VI injuries often need 12 to 18 months before they are able to resume
many of their routine daily activities. Functional outcomes in these
severe injuries are guarded, and patients rarely resume competitive
athletics. Functional range of motion with painless ambulation, normal
alignment of mechanical axis, and the resumption of daily activities
remain the goal.
dissection through traumatized soft tissues often contribute to early
wound breakdown and infection. Spanning fixation techniques and delayed
surgery can minimize these complications. If wound breakdown occurs,
aggressive irrigation and debridement of all devitalized skin, muscle,
and bone is mandatory. If the wound can be closed without tension, then
closure over suction drains is recommended. If a deep infection with
purulence is encountered, the wound should be packed opened and
re-débrided every 48 hours. A vacuum-assisted closure (VAC) sponge
system is helpful in managing large open wounds. Once a
culture-negative wound has been obtained, secondary wound closure
should be accomplished. In many cases, especially if a wound VAC system
has been utilized, delayed primary closure can be completed. However,
in some cases, closure will require a lateral or medial gastrocnemius
rotational flap. Occasionally, a free tissue transfer is necessary.
the fracture site. If the hardware is loose, it should be removed and
the limb stabilized with a joint-spanning external fixator. This often
results in compromised knee function or even a knee fusion as severe
intra-articular sepsis combined with instability results in rapid
chondrolysis with destruction of the knee joint.
type V and VI fractures, specifically at the diaphyseal-metaphyseal
junction. These injuries should be bone grafted. Revision fixation may
also be necessary. Occasionally, nonunion occurs with late collapse of
the articular surface or varus deformity of the metaphyseal-diaphyseal
junction. If the mechanical axis is affected, then a corrective
osteotomy may be required. If the patient is older and the articular
mal-alignment results in significant shift of the mechanical axis,
revision to a total knee arthroplasty may be appropriate.
of motion has been delayed. Arthroscopic lysis of adhesions combined
with gentle manipulation under anesthesia may be helpful for patients
who failed to achieve 90 degrees of knee flexion in the first 4 weeks
after surgery. Heterotopic ossification rarely occurs in tibial plateau
fractures but does occur in concert with coexistent
fracture-dislocations of the knee. In these cases, the heterotopic bone
should be monitored until obvious maturity has occurred and no other
bone formation is visible. CT scans help to delineate the orientation
and location of heterotopic bone.
concert with knee manipulations. Although results are encouraging,
patients usually end up with some degree of residual knee stiffness.
sustained multiple injuries including a closed, Schatzker VI,
bicondylar, tibial-plateau fracture with significant swelling,
soft-tissue contusion, and a compartment syndrome (Fig. 26.18).
The patient was taken emergently for spanning external fixation and 4
compartment fasciotomies thru lateral and medial incisions. A
postoperative, distraction, CT scan demonstrated comminution at the
base of the medial condylar fracture with the apex directed
posteromedially. Minimal impaction of
the
lateral joint surface is visualized, and overall metaphyseal and shaft
reduction has been accomplished with the spanning frame. Seventeen days
after injury, a lateral exposure was used to expose the lateral
condyle. Using percutaneous joysticks and large reduction forceps, the
intracondylar fracture was reduced and held temporarily with K wires.
 |
|
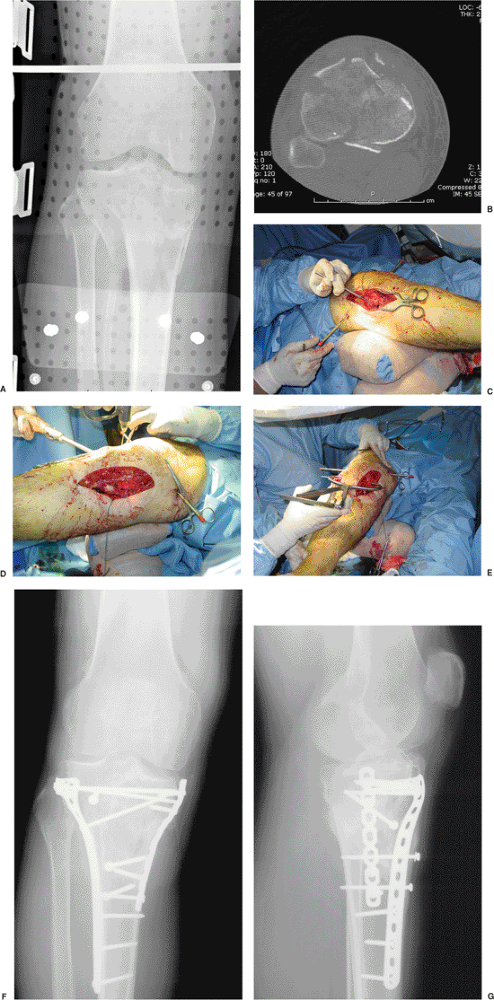
Figure 26.18. A,B.
Initial injury film reveals a Schatzker V/VI fracture with associated compartment syndrome. The patient was taken to the operating room for spanning external fixation and fasciotomies. Intraoperative imaging demonstrates ligamentotaxis reduction and shaft realignment. C1,2. Distraction CT scan demonstrates bicondylar fracture with medial condylar comminution and coronal split. D,E. Follow-up at 1 year demonstrates condylar healing and maintenance of the mechanical axis without varus deformity. Intra-articular congruency has been maintained. |
fracture through the medial condyle; this was reduced and compressed
with a small tenaculum forceps placed percutaneously. This fracture was
stabilized with a front-to-back lag screw. A lateral, peri-articular,
locking plate was then advanced down the proximal shaft in a
submuscular fashion. The proximal raft screws were placed across both
the lateral and medial condyles. The distal screws were placed via
small percutaneous stab wounds to limit the lateral exposure. Because
the distraction CT demonstrated extensive comminution at the base of
the medial condyle, a posteromedial locking plate was positioned at the
apex of the medial fracture line. The medial plate was located
posteriorly to the pes along the posteromedial border of the proximal
tibia.
excellent joint congruency maintained at 1 year follow-up. The patient
was able to resume daily activities and continue his occupation as a
student.
SV, Nevins RT, Sallis JG, et al. Impact of MRI on treatment plan and
fracture classification of tibial plateau fractures. J Orthop Trauma October 2002;16(9):632–637.
YS, Yuan LJ, Hung SS, et al. Arthroscopic-assisted reduction with
bilateral buttress plate fixation of complex tibial plateau fractures. Arthroscopy November 2003;19(9):974–984.
PA, Zlowodzki M, Kregor PJ. Treatment of proximal tibia fractures using
the less invasive stabilization system: surgical experience and early
clinical results in 77 fractures. J Orthop Trauma September 2004; 18(8):528–535.