
Editors: Berquist, Thomas H.
Title: Musculoskeletal Imaging Companion, 2nd Edition
Copyright ©2007 Lippincott Williams & Wilkins
> Table of Contents > Chapter 15 – Miscellaneous Conditions
Chapter 15
Miscellaneous Conditions
Thomas H. Berquist
Bone Islands (Enostosis)
Key Facts
-
Bone islands are benign sclerotic areas in bone. They may be single or multiple.
-
Bone islands typically are noted incidentally on radiographs.
-
Lesions may be seen in patients from 7 to 78 years of age. There is no sex predilection.
-
The most common sites are the ribs, pelvis, and femora. Up to 32% may change in size.
-
Radiographic features:
-
Round, oval, or spiculated sclerotic areas typically (66%) are 0.5 to 1.5 cm.
-
Appearance usually is characteristic,
although the differential diagnosis could include blastic metastasis,
osteoma, osteoid osteoma, or infarct. -
Other imaging studies usually are not
required. Radionuclide bone scans typically are normal, but focal
increased tracer can occur. -
Magnetic resonance imaging (MRI) shows low signal intensity on T1- and T2-weighted sequences.
P.894 -
 |
|
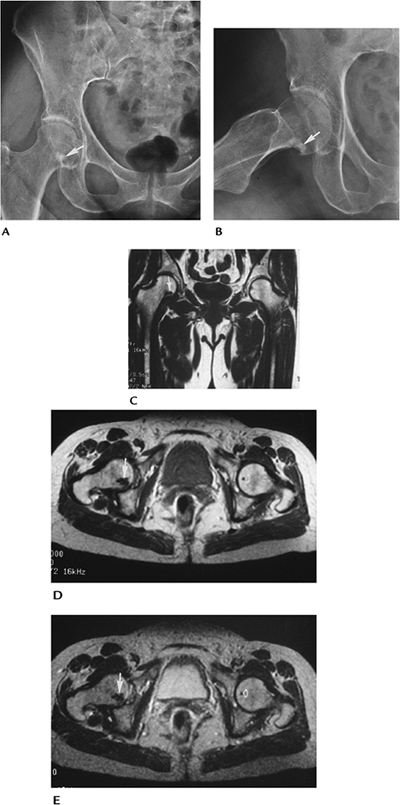
FIGURE 15-1 Bone island in the femoral neck in a 60-year-old man. Anteroposterior (AP) (A) and oblique (B) radiographs demonstrate a spiculated sclerotic focus (arrow). Coronal T1-weighted (C), axial proton density (D), and T2-weighted (E) images showing a low-intensity lesion on all sequences with irregular margins (arrow). There is a small bone island in the opposite femoral head (open arrow) on the axial images (D,E).
|
P.895
Suggested Reading
Hall FE, Goldberg RP, Davies JAK, et al. Scintigraphic assessment of bone islands. Radiology 1980;135:737–742.
P.896
Osteopoikilosis
Key Facts
-
Osteopoikilosis is a sclerotic bone dysplasia presenting in childhood. It has been detected in all bones except the skull.
-
Lesions are smaller than typical bone islands (2–10 mm).
-
The condition is considered an autosomal dominant chondrodysplasia.
-
Lesions may grow in children but stabilize or disappear in adults.
-
Most patients are asymptomatic, although 20% may present with joint pain.
-
Radiographic features:
-
Lesions are smaller and more well-defined than bone islands and involve the epiphysis and metaphysis.
-
Features are so characteristic that there usually is no difficulty in diagnosis.
-
Differential considerations include mastocytosis and tuberous sclerosis.
-
Radionuclide scans typically are normal but may be positive in growing lesions.
-
 |
|
FIGURE 15-2
Osteopoikilosis. AP radiograph of the pelvis and hips showing multiple small sclerotic foci in the proximal femora, ischia, and acetabuli. Note the femoral striations (arrows) (osteopathia striata is related to osteopoikilosis). |
Suggested Reading
Green AE, Ellowood WH, Collins JR. Melorheostosis and osteopoikilosis. AJR Am J Roentgenol 1962;87:1096–1117.
P.897
Osteopathia Striata
Key Facts
-
Osteopathia striata is a rare autosomal dominant inherited condition related to osteopoikilosis.
-
Patients usually are asymptomatic.
-
Radiographic features:
-
Distinct striations in the metaphysis of long bones parallel to the shaft. Striations may extend into the epiphysis.
-
Changes usually are bilateral.
-
The tibia is the most common site.
-
Radionuclide scans are normal.
-
P.898
 |
|
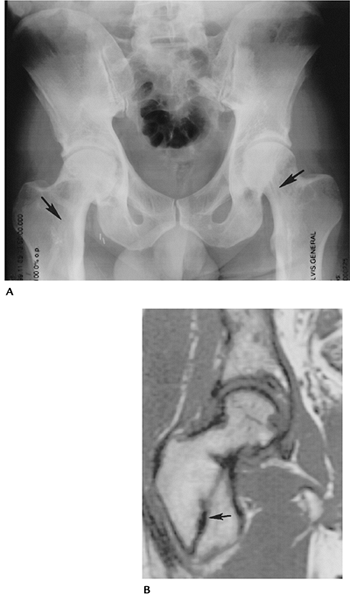
FIGURE 15-3 Osteopathia striata. (A) AP radiograph of the pelvis and hips showing linear striations in the femoral neck (arrows) with cortical thickening medially from associated melorheostosis. (B) Coronal T1-weighted magnetic resonance (MR) image of the right hip showing the low signal intensity linear sclerosis (arrow).
|
Suggested Reading
Hurt RL. Osteopathia striata. Voorhoeve disease. J Bone Joint Surg 1953;35B:89–96.
P.899
Melorheostosis
Key Facts
-
Melorheostosis causes bone sclerosis
involving one side of the cortex. The original description looked like
dripping candle wax, thus the term “melorheostosis.” -
Cause is unknown. Patients may be asymptomatic or present with pain in the involved region.
-
The condition may be present from birth
to late adult life. In 50% of cases, the condition is evident by 20
years of age. There is no sex predilection. -
The involved extremity may be shorter or, in some cases, longer. Muscle atrophy also is present in some cases.
-
Radiographic features:
-
The condition most commonly involves the long bones of the extremities. Most often it is unilateral.
-
Sclerosis and cortical thickening involve
one side of the involved bone or bones. Typically, the process extends
into the metaphysis or epiphysis, but soft tissue and joint involvement
can occur. Associated conditions include:-
Leg length discrepancy
-
Scleroderma
-
Neurofibromatosis
-
Osteopoikilosis
-
Osteopathia striata
-
Hemangiomas
-
-
P.900
 |
|
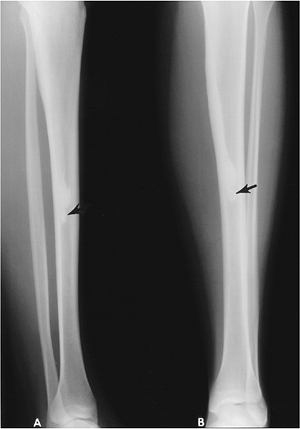
FIGURE 15-4 Melorheostosis. Lateral (A) and AP (B)
views of the tibia showing sclerosis along the posteromedial cortex resembling “dripping candle wax” that ends in the mid-diaphysis (arrow). |
P.901
 |
|
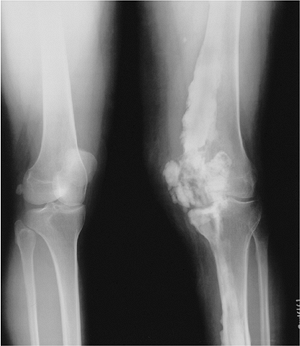
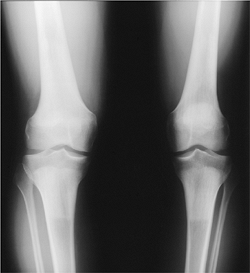
FIGURE 15-5
Melorheostosis. Standing views of the knees showing sclerosis and cortical thickening that crosses the joint into the soft tissues. The tibia also is involved. |
Suggested Reading
Morris JM, Samilson RL, Corey CL. Melorheostosis. J Bone Joint Surg 1963;45A:1191–1206.
P.902
Progressive Diaphyseal Dysplasia (Engelmann Disease)
Key Facts
-
Engelmann disease results in cortical
thickening in the diaphysis of long bones progressing proximally and
distally in the involved structure. -
Most patients present in infancy or early childhood. It is an autosomal dominant inherited condition.
-
Neuromuscular dystrophy and malnutrition are associated with this condition.
-
Radiographic features:
-
Symmetric distribution
-
Diaphyseal cortical thickening involving endosteal and periosteal surfaces
-
Normal epiphysis and metaphysis
-
Relative elongation of involved extremities
-
Muscle atrophy
-
Differential diagnosis: chronic infection, infantile cortical hyperostosis, fibrous dysplasia
-
P.903
 |
|
FIGURE 15-6 Engelmann disease. (A)
Radionuclide bone scan showing symmetric increased cortical uptake in the femora, tibiae, and upper extremities. AP radiographs of the femur (B) and tibia (C) showing marked diaphyseal cortical thickening with sparing of the metaphyses and epiphyses. |
Suggested Reading
Kumar
B, Murphy WA, Whyte MP. Progressive diaphyseal dysplasia (Engelmann
disease): Scintigraphic-radiographic-clinical correlations. Radiology 1981;140:87–92.
B, Murphy WA, Whyte MP. Progressive diaphyseal dysplasia (Engelmann
disease): Scintigraphic-radiographic-clinical correlations. Radiology 1981;140:87–92.
P.904
Cleidocranial Dysplasia (Cleidocranial Dysostosis)
Key Facts
-
Cleidocranial dysplasia is an uncommon autosomal dominant disorder.
-
Patients present with delayed or
incomplete cranial ossification and hypoplastic or aplastic clavicles.
Delayed ossification may be evident in the axial skeleton and
extremities. -
The mandible may be large, and delayed tooth development is common.
-
Radiographic features:
-
Lack of midline ossification and wormian bones in the calvarium
-
Absent or hypoplastic clavicles
-
Delayed ossification in the spine, pelvis, and extremities
-
Femoral necks deformed or aplastic
-
P.905
 |
|
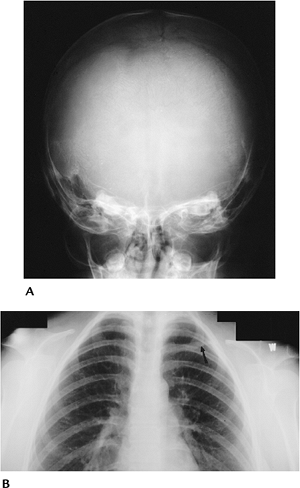
FIGURE 15-7 Cleidocranial dysplasia. (A) AP view of the skull showing multiple wormian bones along the suture lines. (B) AP view of the upper chest showing an absent right clavicle and small hypoplastic medial segment (arrow) on the left.
|
Suggested Reading
Jarvis JL, Keats TE. Cleidocranial dysostosis. A review of 40 new cases. AJR Am J Roentgenol 1974;121:5–16.
P.906
Osteopetrosis
Key Facts
-
Osteopetrosis is a disease of uncertain cause that leads to dense brittle bones.
-
There are multiple clinical forms of this condition.
-
Osteopetrosis infantile: autosomal
recessive with failure to thrive, hepatosplenomegaly, cranial nerve
dysfunction, blindness, and deafness. Death frequently occurs in early
years of life. -
Osteopetrosis tarda (delayed): autosomal
dominant. Patients usually are asymptomatic. Detection results from
mild anemia, cranial nerve palsies, or pathologic fractures. -
Osteopetrosis intermediate: autosomal recessive with features between infantile and tarda in severity.
-
-
Radiographic features:
-
Infantile: uniformly dense sclerotic bones with changes similar to rickets near the growth plates
-
Tarda: bone-within-a-bone appearance
-
Intermediate: diffuse bone sclerosis,
especially of the skull base. Bone-within-a-bone appearance. Avascular
necrosis of the femoral heads.
-
P.907
 |
|
FIGURE 15-8
Osteopetrosis intermediate. AP radiographs of the tibia and femora showing bone sclerosis with bone-within-a-bone appearance in the epiphyses. |
P.908
 |
|
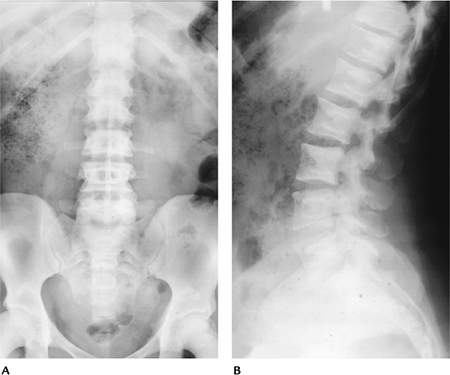
FIGURE 15-9 Osteopetrosis tarda. AP (A) and lateral (B) radiographs of the lumbar spine showing a bone-within-a-bone appearance.
|
Suggested Reading
Shapiro F, Glimcher MJ, Holtrop ME, et al. Human osteopetrosis. J Bone Joint Surg 1980;62A:384–399.
P.909
Mastocytosis
Key Facts
-
Mastocytosis is a systemic disease with mast cell accumulation in multiple organs affecting adult males and females.
-
Liver, spleen, lymph node, skeletal, and most commonly cutaneous organs are involved.
-
Patients present with skin lesions
resembling urticaria pigmentosa, also diarrhea, vomiting, flushing, or
intermittent shocklike episodes. -
Radiographic features occur in 70% of patients:
-
Osteopenia and bone destruction most common in the skull, spine, and ribs
-
Osteosclerosis, which may resemble metastasis, Paget disease, or myelofibrosis
-
Features may be focal or diffuse.
-
P.910
 |
|
FIGURE 15-10 Mastocytosis. (A)
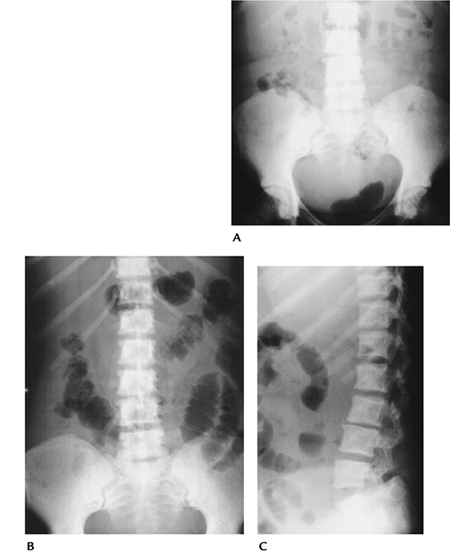
AP radiograph of the lumbar spine and pelvis showing generalized bone sclerosis and cortical thickening. There are more focal foci of sclerosis in the femoral heads. AP (B) and lateral (C) radiographs of the lumbar spine and pelvis in a different patient showing diffuse small sclerotic foci. |
Suggested Reading
McKenna MJ, Frame B. The mast cell and bone. Clin Orthop 1985;200:226–233.
P.911
Tuberous Sclerosis
Key Facts
-
Tuberous sclerosis is an autosomal dominant inherited disorder.
-
Characteristic features include seizure disorders, mental retardation, and cutaneous hamartomas.
-
Radiographic features:
-
Skull: foci of sclerosis and trabecular
prominence; calvarial thickening; intercerebral calcifications; brain
lesions in ventricles, white matter, and cortex 50% to 80%. -
Axial/appendicular skeleton: focal or
diffuse cystlike lesions or areas of sclerosis. Subperiosteal and
cortical lesions result in irregular cortical appearance. -
Extraskeletal lesions: Fifty percent have
renal cysts, angiolipomas, and aneurysms; 30% to 50% have rhabdomyomas
of the heart. Pulmonary lesions in 1% commonly lead to pneumothorax.
-
 |
|
FIGURE 15-11
Tuberous sclerosis. AP radiograph of the pelvis showing oval- or flame-shaped areas of sclerosis in both iliac wings. There is an impacted left femoral neck fracture with pin fixation unrelated to the bone changes of tuberous sclerosis. |
P.912
 |
|
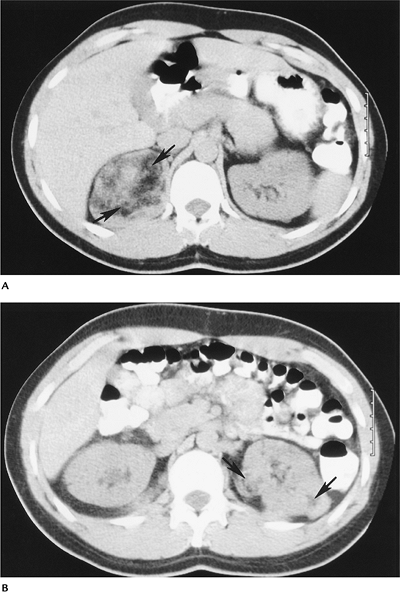
FIGURE 15-12 Tuberous sclerosis with renal angiomyolipomas. (A,B) Computed tomography (CT) images showing characteristic fat density masses (arrows), the largest in the right kidney.
|
P.913
 |
|
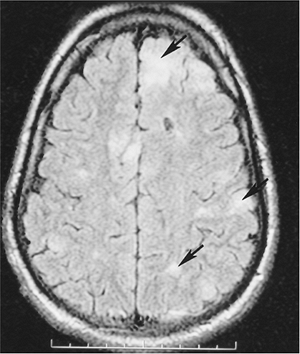
FIGURE 15-13 Tuberous sclerosis. Axial T2-weighted MR image showing multiple areas of signal abnormality (arrows) resulting from cortical tubers.
|
Suggested Reading
Medley BE, McLeod RA, Houser OW. Tuberous sclerosis. Semin Roentgenol 1976;11:35–54.
Wood B, Leiberman E, Larding B, et al. Tuberous sclerosis. AJR Am J Roentgenol 1992;158:750.
P.914
Neurofibromatosis
Key Facts
-
Neurofibromatosis is one of the most common inherited (autosomal dominant) disorders.
-
Clinical triad includes skin lesions, mental retardation, and skeletal deformities.
-
More than 99% of cases are in the category of neurofibromatosis Type 1 or Type 2.
-
• Type 1 (two or more features) Six or more café-au-lait skin lesions
Two or more neurofibromas or one plexiform neurofibroma
Inguinal or axillary freckling
Optic glioma
Two or more iris hematomas
Osseous lesion
Parent, sibling, or child with Type 1• Type 2 (one feature) Bilateral eighth nerve masses • Type 2 in parent, sibling,
or child and an eighth nerve mass, or two of the following:
neurofibroma, meningioma, glioma schwannoma, or posterior capsular
lenticular capacity
-
-
Radiographic features:
-
Osseous features
-
Orbital and facial bone deformities
-
Spinal deformities (60%)
-
Scoliosis
-
Kyphoscoliosis
-
Vertebral scalloping
-
Pedicle erosion
-
Spindle ribs and transverse processes
-
Extremities
-
Bowing (especially tibia)
-
Pathologic fracture
-
Hypoplastic fibula
-
Pseudoarthrosis with pathologic fracture
-
-
Neural
-
Meningoceles
-
Cranial nerve tumors
-
Peripheral nerve neurofibromas and schwannomas
-
Malignant degeneration of neural lesions 2% to 29%
-
-
Other associated lesions
-
Neuroblastoma
-
Pheochromocytoma
-
Thyroid carcinoma
-
Wilms tumor
-
Rhabdomyosarcoma
-
Leukemia
-
P.915
 |
|
FIGURE 15-14 Neurofibromatosis Type 1. AP (A) and lateral (B) radiographs showing tibial bowing with a healed midtibial fracture.
|
P.916
 |
|
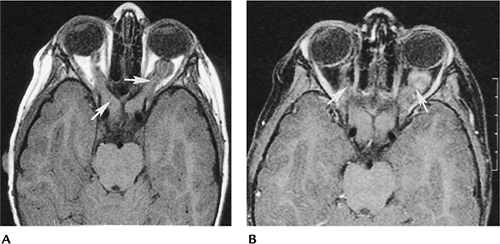
FIGURE 15-15 Neurofibromatosis Type 1. Axial precontrast (A) and postcontrast (B) images showing enlargement of both optic nerves (arrows) caused by optic nerve gliomas.
|
P.917
 |
|
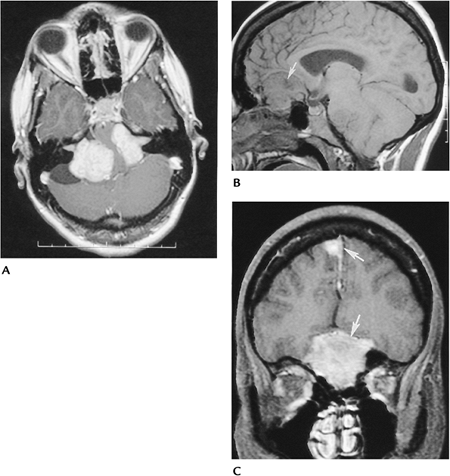
FIGURE 15-16 Neurofibromatosis Type 2. Bilateral vestibular nerve schwannomas and multiple meningiomas. (A)
Postcontrast axial MR image showing bilateral large vestibular nerve schwannomas extending into the internal auditory canals and compressing the pons. Sagittal (B) and coronal enhanced (C) T1-weighted images showing multiple meningiomas (arrows). |
Suggested Reading
Sevick RJ, Barkovich AJ, Edwards MS, et al. Evolution of white matter lesions in neurofibromatosis type 1: MR findings. AJR Am J Roentgenol 1992;159:171–175.
P.918
Ollier Disease (Enchondromatosis)
Key Facts
-
Ollier disease is a noninherited condition resulting in multiple asymmetrically distributed enchondromas.
-
Lesions lead to fractures in adults and children.
-
In adults, lesions may undergo malignant degeneration to chondrosarcoma (5%–30%).
-
Radiographic features:
-
Multiple lytic expanding lesions are located predominantly in the extremities.
-
Flat bones of the pelvis also may be involved.
-
Lesions may contain calcification.
-
P.919
 |
|
FIGURE 15-17 Ollier disease. (A) Posteroanterior (PA) chest radiographs showing multiple expanded calcified rib lesion (arrows). (B) PA view of the hand showing enchondromas in the second to fourth rays. AP radiographs of the pelvis (C) and femora (D) showing multiple enchondromas in the left femur. The largest expand the distal femur.
|
Suggested Reading
Milgram JW. The origins of osteochondromas and enchondromas. A histopathologic study. Clin Orthop 1983;174:264–284.
P.920
Maffucci Syndrome
Key Facts
-
Maffucci syndrome is a rare disorder with multiple enchondromas and soft tissue hemangiomas.
-
The syndrome occurs in males and females, beginning in childhood.
-
Half of the cases are unilateral. The hand is most commonly involved.
-
Enchondromas may undergo malignant transformation to chondrosarcoma.
-
Radiographic features:
-
Multiple expanding lytic lesions that may contain calcifications
-
Soft tissue masses (hemangiomas) with phleboliths are characteristic.
-
 |
|
FIGURE 15-18 Maffucci syndrome. Oblique radiograph showing multiple enchondromas and soft tissue masses with vascular calcifications.
|
Suggested Reading
Strang C, Ronnie I. Dyschondroplasia and hemangiomata (Maffucci’s syndrome). J Bone Joint Surg 1950;32B:376–383.
P.921
Hereditary Multiple Exostosis
Key Facts
-
Hereditary multiple exostosis is an autosomal dominant condition resulting in abnormal bone remodeling and bone deformities.
-
Patients present in childhood with palpable osseous masses, bone shortening, bowing, and joint deformities.
-
Osseous lesions relate to osteochondromas and are bilateral and near the physis.
-
Complications:
-
Pathologic fracture
-
Neurovascular injury
-
Bursa formation
-
Malignant degeneration (chondrosarcoma in 2% to 27%)
-
-
Radiographic features:
-
Osteochondroma-like lesions
-
Most common in the knee and proximal humerus
-
Lesions usually are bilateral and symmetric.
-
P.922
 |
|
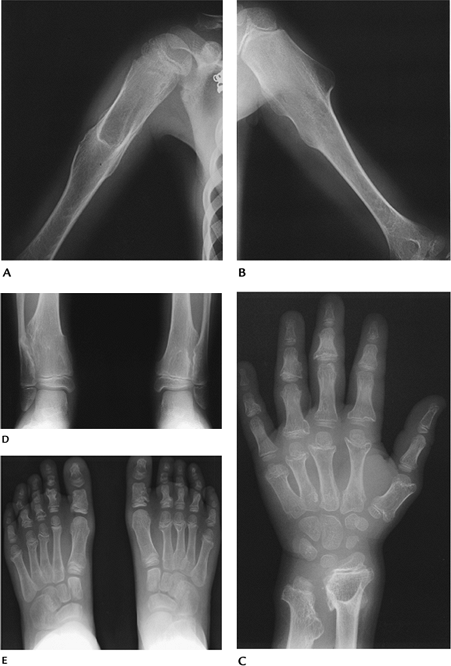
FIGURE 15-19 Hereditary multiple exostosis. Radiographs of the humeri (A,B), left hand and wrist (C), both ankles (D), and feet (E) demonstrate multiple exostoses with bone and joint deformities most obvious in the hand and wrist.
|
P.923
Suggested Reading
Wilner D. Radiology of bone tumors and allied disorders. Philadelphia: WB Saunders; 1982.
P.924
Epiphyseal Dysplasias
Key Facts
-
Epiphyseal dysplasias have two broad categories:
-
Spondyloepiphyseal dysplasia: platyspondyly and beaking of the vertebra
-
Multiple epiphyseal dysplasia: minimal or no spine abnormalities
-
-
Multiple epiphyseal dysplasia may present in the tarda (childhood) or congenital (first year of life) forms.
-
Multiple epiphyseal dysplasia tarda:
-
Both sexes equally affected
-
Bilateral symmetric involvement of hips, knees, ankles, shoulders, and wrists
-
No mental retardation
-
Present in early childhood with joint pain and gait disturbances
-
Early degenerative joint disease
-
-
Radiographic features:
-
Long bone epiphysis appears late
-
Irregular and fragmented when ossified
-
Slipped epiphysis, coxa vara, and joint deformities common
-
-
Multiple epiphyseal dysplasia congenita
has multiple types, including sex-linked and autosomal recessive forms
(latter more severe).-
Patients present with calcification of unossified epiphysis in the first year of life.
-
Dwarfism, sclerosis, skin lesions, and cataracts are common.
-
Mental retardation is present in more severe forms.
-
-
Radiographic features:
-
Scattered epiphyseal calcifications
-
Shortened long bones
-
P.925
P.926
 |
|
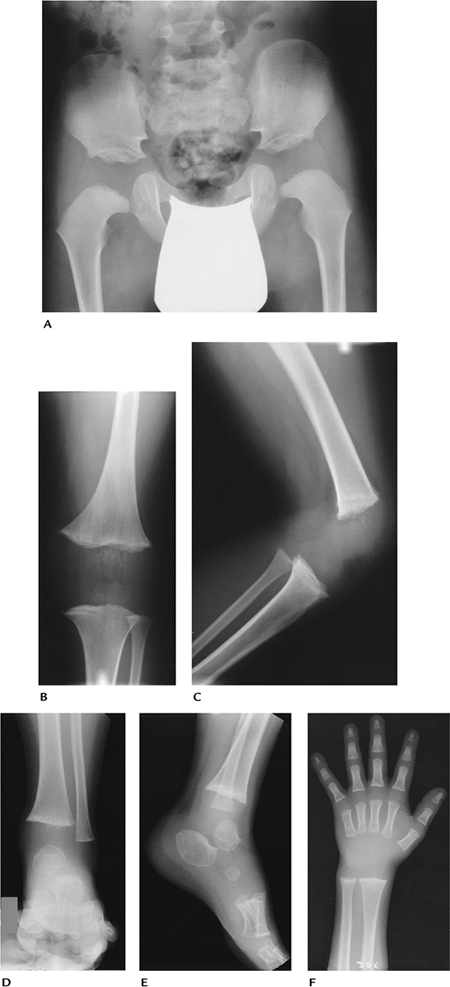
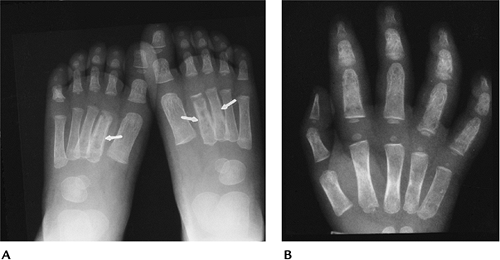
FIGURE 15-20 Multiple epiphyseal dysplasia. Radiographs of the hip (A), left knee (B,C), left foot and ankle (D,E), and left wrist (F) show lack of epiphyseal ossification centers with punctate calcifications in the knee.
|
P.927
 |
|
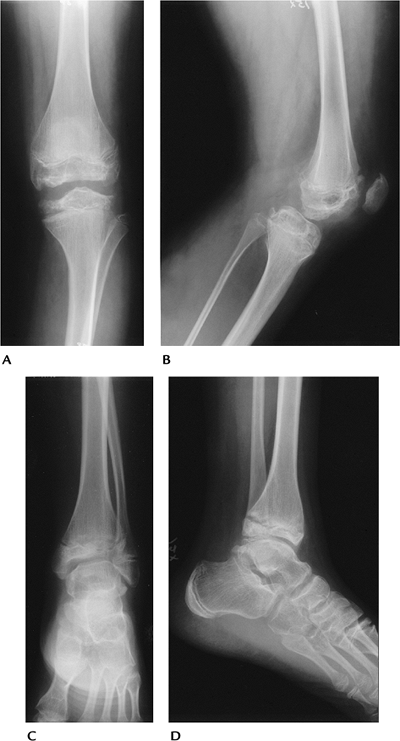
FIGURE 15-21 Multiple epiphyseal dysplasia in an adolescent. AP and lateral radiographs of the knee (A,B) and ankle (C,D) showing irregular epiphysis with joint deformities.
|
Suggested Reading
Berg PK. Dysplasia epiphyseal multiplex. AJR Am J Roentgenol 1966;97:31–38.
P.928
Metaphyseal Dysplasias
Key Facts
-
Metaphyseal dysplasias consist of a group
of conditions primarily affecting the metaphysis. However, the
diaphysis and epiphysis also may be abnormal. -
Spine involvement is uncommon.
-
Types of metaphyseal dysplasia:
-
Jansen Type: A rare autosomal dominant disorder presenting with dwarfism and bowing of the forearms and legs.
-
Radiographic features: small mandible,
prominent frontal sinuses; metaphyseal irregularity and widening
extremity bowing with flared metaphysis in childhood.
-
-
Schmid Type: autosomal dominant inheritance. Patients have short stature and bowing of the lower extremities.
-
Radiographic features: metaphyseal irregularity and physeal widening, especially in hips and knees.
-
-
McKusick Type: autosomal recessive
inheritance. Short stature, fine light hair, small hands, joint laxity,
and bowing of the lower extremities.-
Radiographic features: metaphyseal cupping and flaring most evident in the lower extremities. Small vertebral bodies.
-
-
Shwachman-Diamond Type: Patients present
with anemia, low white blood cell and platelet counts, and pancreatic
insufficiency. Failure to thrive and recurrent pneumonias are part of
the syndrome.-
Radiographic features: coxa vara, osteopenia, metaphyseal irregularity, and irregularity of vertebral bodies.
-
-
 |
|
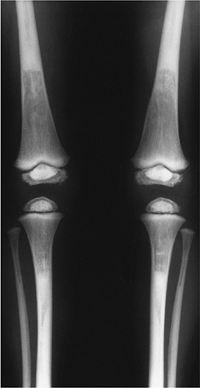
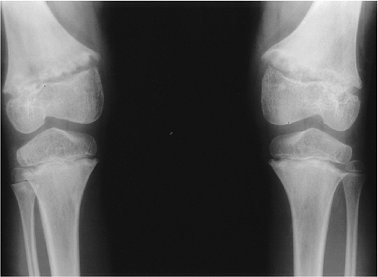
FIGURE 15-22 Metaphyseal dysplasia. Standing radiographs of the knees showing metaphyseal irregularity and flaring with femoral bowing.
|
Suggested Reading
McAlister
WH, Herman TE. Osteochondrodysplasias, dysostosis, chromosomal
aberrations, mucopolysaccharidoses, and mucolipidosis. In: Resnick D,
Kransdorf MJ, eds. Bone and joint imaging, 3rd ed. Philadelphia: Elsevier-Saunders; 2005:1298–1325.
WH, Herman TE. Osteochondrodysplasias, dysostosis, chromosomal
aberrations, mucopolysaccharidoses, and mucolipidosis. In: Resnick D,
Kransdorf MJ, eds. Bone and joint imaging, 3rd ed. Philadelphia: Elsevier-Saunders; 2005:1298–1325.
P.929
Marfan Syndrome
Key Facts
-
Marfan syndrome is a disorder of
connective tissue involving the skeleton, cardiovascular system, and
eyes. Inheritance is autosomal dominant. -
There is no sex predilection. Patients
typically are tall and thin with long limbs. The most evident length
disproportion is in the hands and feet. -
Patients may have pectus deformity, scoliosis, and joint laxity.
-
Cardiovascular abnormalities (aortic and mitral insufficiency and aortic aneurysms) may shorten life expectancy.
-
Ocular abnormalities include myopia and ectopic lentis, with cataract formation in later life.
-
Radiographic features:
-
Hands and feet—arachnodactyly, pes planus, digital deformities (e.g., hammer toe, claw toe)
-
Reduced muscle mass and fat around long bones; slender long bones.
-
Scoliosis in up to 60% of patients
-
Protrusio acetabuli
-
Pectus deformity and rib elongation
-
 |
|
FIGURE 15-23 Marfan syndrome. PA radiographs of the hands showing elongation and thin metacarpals and phalanges.
|
Suggested Reading
Goldman
AB. Heritable diseases of connective tissue, epiphyseal dysplasias, and
related conditions. In: Resnick D, Kransdorf MJ, eds. Bone and joint imaging, 3rd ed. Philadelphia: Elsevier-Saunders; 2005:1279–1297.
AB. Heritable diseases of connective tissue, epiphyseal dysplasias, and
related conditions. In: Resnick D, Kransdorf MJ, eds. Bone and joint imaging, 3rd ed. Philadelphia: Elsevier-Saunders; 2005:1279–1297.
P.930
Ehlers-Danlos Syndrome
Key Facts
-
Ehlers-Danlos syndrome is a familial connective tissue disorder.
-
Most patients present in childhood.
-
Patients present with fragile skin, joint laxity, and bleeding disorders.
-
Multisystem involvement may include ocular, pulmonary, gastrointestinal, genitourinary, and cardiovascular disorders.
-
Radiographic features:
-
Subcutaneous calcifications resembling phleboliths on the extensor surfaces of the forearms and legs
-
Joint effusions, hemarthrosis, and subluxations
-
Spinal deformity and scoliosis result from ligament laxity
-
Posterior vertebral scalloping secondary to dural ectasia
-
 |
|
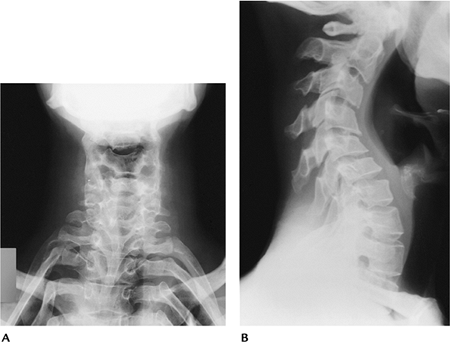
FIGURE 15-24 Ehlers-Danlos syndrome. AP (A) and lateral (B) radiographs of the cervical spine showing exaggeration of the cervical curves.
|
Suggested Reading
Goldman
AB. Heritable diseases of connective tissue, epiphyseal dysplasias, and
related conditions. In: Resnick D, Kransdorf MJ, eds. Bone and joint imaging, 3rd ed. Philadelphia: Elsevier-Saunders; 2005:1279–1297.
AB. Heritable diseases of connective tissue, epiphyseal dysplasias, and
related conditions. In: Resnick D, Kransdorf MJ, eds. Bone and joint imaging, 3rd ed. Philadelphia: Elsevier-Saunders; 2005:1279–1297.
P.931
Osteogenesis Imperfecta
Key Facts
-
Osteogenesis imperfecta is an inherited connective tissue disorder affecting multiple organ systems.
-
There are four clinical features:
-
Osteoporosis with pathologic fractures
-
Blue sclera
-
Dentinogenesis
-
Premature otosclerosis
-
-
Classically, the disorder is considered
as either congenita or tarda form. More recently, a new classification
was developed based on clinical, radiographic, and genetic features
(Sillence classification).Type I Most common; mildest form Type II Lethal; in utero fractures Type III Rare; majority have fractures at birth Type IV Most variable osseous features -
Radiographic features:
-
Diffuse osteoporosis
-
Thin, gracile bones (Types I and IV)
-
Short, thick extremities (Types II and III)
-
Fractures; lower extremity most common
-
Pseudoarthrosis
-
Pelvis narrow; triradiate
-
P.932
 |
|
FIGURE 15-25
Osteogenesis imperfecta Type II. Radiograph of a newborn with short, thick osteoporotic extremities and multiple fractures that occurred in utero. |
P.933
 |
|
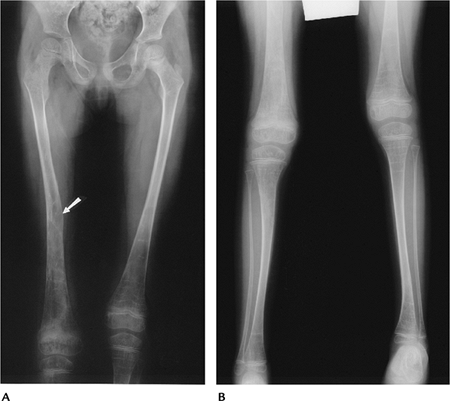
FIGURE 15-26 Osteogenesis imperfecta Type I (tarda). AP radiographs of the femora (A) and legs (B) showing thin, gracile osteoporotic bones with a healed fracture (arrow) in the right femur.
|
Suggested Reading
Sillence D. Osteogenesis imperfect: An expanding panorama of variants. Clin Orthop 1981;159:11–25.
P.934
Achondroplasia
Key Facts
-
Achondroplasia presents in two forms:
-
Heterozygous (most common): evident at birth. Dwarfism with normal lifespan.
-
Homozygous (lethal): rare. Patients die in early infancy.
-
-
Patients with typical achondroplasia
present with short limbs, more pronounced proximally (rhizomelic
micromelia); large head; prominent buttocks; thoracic kyphosis; and
exaggerated lumbar lordosis. Hands are short. Spinal changes frequently
lead to spinal stenosis. -
Radiographic features:
-
Large skull with small foramen magnum
-
Lumbar interpedicular distance stays the same or decreases from L1 to L5 (normally increases).
-
Pedicles short and posterior vertebral line concave
-
Square iliac bones with small sacrosciatic notches and flat acetabular angles
-
Short proximal long bones with metaphyseal flaring
-
Shortening of the bones in the hands and feet
-
P.935
 |
|
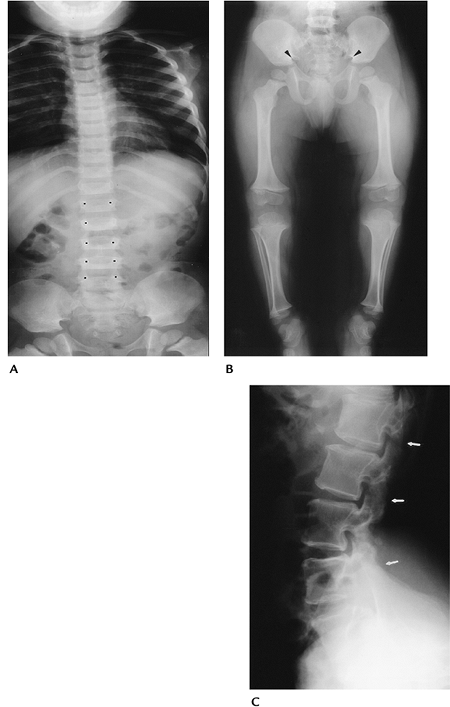
FIGURE 15-27 Achondroplasia. (A) AP radiograph of the spine showing no change in lumbar interpedicular distance (black dots) progressing from L1 to L5. (B) AP radiograph of the pelvis and lower extremities showing small sciatic notches (arrowheads), flattening of the acetabular angles, iliac squaring, and short tubular bones with metaphyseal flaring in the knees. (C)
Lateral radiograph of the spine in an older patient showing short pedicles and concave posterior vertebral margins. The narrowed spinal canal has resulted in laminectomies (arrows). |
Suggested Reading
Langer LO, Baumann PA, Gorlin RJ. Achondroplasia. AJR Am J Roentgenol 1967;100:12–26.
P.936
Mucopolysaccharidoses
Key Facts
-
Mucopolysaccharidoses (MPS) constitute a
group of disorders that present with dwarfism and clinical, laboratory,
and radiographic features that differentiate the conditions. -
There are seven separate categories of MPS, with Hurler (MPS-IH) and Morquio syndrome (MPS-IV) most well known radiographically.
-
Table 15-1 summarizes features and enzyme deficiencies in MPS syndromes.
-
Hurler syndrome (MPS-IH):
-
Autosomal recessive manifesting in first years of life
-
Mental retardation, corneal clouding, deafness, cardiac disease
-
Death in first decade from cardiac disease
-
-
Radiographic features:
-
Macrocephaly, J-shaped sella
-
Widening of anterior ribs
-
Hypoplastic vertebra at thoracolumbar junction
-
C1–2 subluxation
-
Shortening and widening of long bones
-
Pointing of proximal metacarpals
-
-
Morquio syndrome (MPS-IV):
-
Severe dwarfism
-
Spinal kyphoscoliosis
-
Joint laxity
-
Prominent mandible and lower face
-
Short neck
-
Mentally normal
-
Corneal clouding and deafness
-
-
Radiographic features:
-
Round vertebral bodies with small anterior beak
-
Anterior sternal bowing, increased AP chest diameter, wide ribs
-
Coxa valga, flared iliac wings, increased acetabular angles
-
Wide metacarpals with proximal pointing, irregular carpal bones
-
Metaphyseal flaring in long bones
-
P.937
|
TABLE 15-1 MUCOPOLYSACCHARIDOSES
|
||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
||||||||||||||||||||||||||||||
P.938
 |
|
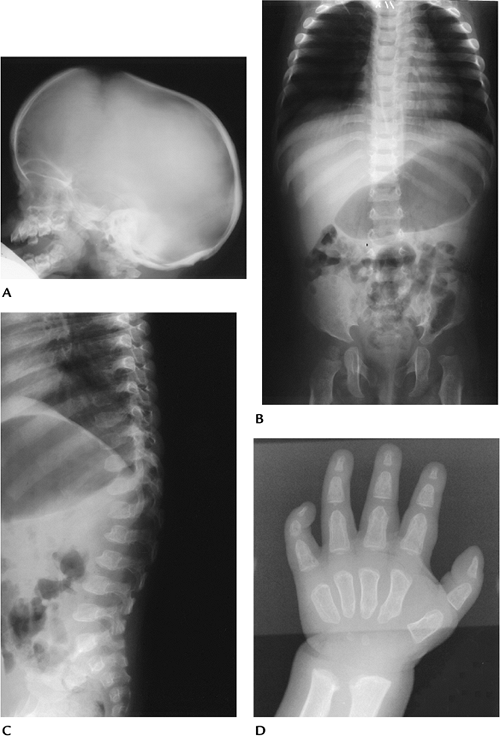
FIGURE 15-28 Hurler Syndrome (MPS-IH). (A) Lateral radiograph of the skull shows a large “J”-shaped sella and underdeveloped mastoids. Sinuses are hypoplastic. (B) AP radiograph of the spine and pelvis demonstrates expanded anterior ribs, hypoplastic ilia, and coxa valga. (C) Lateral radiograph of the spine shows hypoplastic vertebrae at the thoracolumbar junction with anterior beaking. (D) Hand radiograph demonstrates thick short metacarpals and phalanges with pointing of the proximal metacarpals.
|
P.939
 |
|
FIGURE 15-29
Morquio syndrome (MPS-IV). Radiograph of the hand showing slanting of the radial and ulnar articular surfaces and small irregular carpal bones. The bones of the hand are short and widened. |
Suggested Reading
Blighton D. Heritable disorders of connective tissue, 5th ed. St. Louis: CV Mosby; 1993.
P.940
Dyschondrosteosis (Leri-Weill Syndrome)
Key Facts
-
This common syndrome is an autosomal dominant disorder with mesomelic extremity shortening and Madelung deformity.
-
The condition is more common in females.
-
The condition affects the forearm and legs.
-
Radiographic features:
-
Shortened dorsally, bowed radius
-
Distal ulna often subluxed
-
V-shaped radioulnar articular surfaces
-
Shortening of the tibia and fibula
-
Coxa valga
-
Shortening of the bones in the hands and feet
-
P.941
 |
|
FIGURE 15-30 Dyschondrosteosis (Leri-Weill syndrome). AP (A) and lateral (B)
radiographs of the forearm showing Madelung deformity with bowing of the radius and a V-shaped radioulnar articular surface with carpal bones collapsed centrally. |
Suggested Reading
Langer LO. Dyschondrosteosis of the inherited bone dysplasias with characteristic roentgenographic features. AJR Am J Roentgenol 1965;95:178–185.
P.942
Pachydermoperiostosis
Key Facts
-
Pachydermoperiostosis, or primary hypertrophic osteoarthropathy, constitutes 3% to 5% of hypertrophic osteoarthropathies.
-
Patients present with clubbing on the
hands and feet, enlargement of the tabular bones caused by bony
proliferation, and pain and swelling in the joints. -
The condition has an autosomal dominant inheritance and is more common in black males.
-
Cortical thickening may lead to marrow failure and extramedullary hematopoiesis.
-
Radiographic features:
-
Clubbing in the hands and feet
-
Irregular bony proliferation in the long
bones involving the diaphysis, metaphysis, and epiphysis (the last not
seen in second-degree hypertrophic osteoarthropathy)
-
P.943
 |
|
FIGURE 15-31 Pachydermoperiostosis (primary hypertrophic osteoarthropathy). Radiographs of the hands (A,B)
demonstrate widening and bony proliferation involving the phalanges and metacarpals with involvement of the radial and ulnar epiphyses. Radiographs of the forearms (C,D) show cortical thickening and irregularity with widening of the radius and ulna. |
P.944
Suggested Reading
Neiman HL, Gompels BM, Martel W. Pachydermoperiostosis with bone marrow failure and gross extramedullary hematopoiesis. Radiology 1974;110:533–554.
P.945
Secondary Hypertrophic Osteoarthropathy
Key Facts
-
Secondary hypertrophic osteoarthropathy
has replaced the term “pulmonary hypertrophic osteoarthropathy” because
there are numerous nonpulmonary causes. -
Pulmonary disorders are commonly involved (50% of patients with mesothelioma, 12% of patients with bronchogenic carcinoma).
-
Gastrointestinal disorders, cystic
fibrosis, and congenital heart disease also are associated with
hypertrophic osteoarthropathy. -
Patients frequently present with joint pain.
-
Radiographic features (Table 15-2):
-
Smooth periostitis
-
Tibiae, fibulae, radii, and ulnae most commonly are involved.
-
Proximal extremities also may be involved.
-
|
TABLE 15-2 PERIOSTITIS
|
||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
P.946
 |
|
FIGURE 15-32 Secondary hypertrophic osteoarthropathy. AP (A) and lateral (B) radiographs in a patient with chronic pulmonary disease showing periosteal new bone along the lateral tibia (arrows), posterior tibia (open arrows), and medial tibia (arrowhead).
|
Suggested Reading
Segal AM, McKenzie AH. Hypertrophic osteoarthropathy. A 10-year retrospective analysis. Semin Arthritis Rheum 1982;12:220–231.
P.947
Vitaminosis: Vitamin A
Key Facts
-
Vitamin A is essential for chondrogenesis and longitudinal bone growth.
-
Radiographic features typically are not present with low levels of vitamin A.
-
Hypervitaminosis A may present as an acute or chronic disorder.
-
Acute: rare today. May be seen with
ingested overdoses of polar bear, shark, or chicken liver. Patients
present with headache, vertigo, and symptoms of increased intracranial
pressure. -
Chronic: Patients present with anorexia,
pruritus, tender subcutaneous nodules over the long bones, fissuring of
the legs, and bleeding.
-
-
Radiographic features:
-
Findings confined to the growing skeleton and more often seen with the chronic form
-
Smooth wavy periostitis along the ulna and metatarsals (Table 15-2)
-
Hyperostosis and metaphyseal deformities
-
Suggested Reading
Ruby LK, Mital MA. Skeletal deformities following chronic hypervitaminosis A. J Bone Joint Surg 1974;56:1283–1287.
P.948
Vitaminosis: Vitamin C
Key Facts
-
Vitamin C is required for collagen and matrix formation.
-
Vitamin C is excreted by the kidneys, so excess serum vitamin C is rare.
-
Vitamin C deficiency is uncommon today, but may cause skeletal changes in children and adults.
-
Clinical features are most common in infants and children.
-
Patients present with failure to thrive, petechiae, and hemorrhaging caused by reduced intracellular cement in capillaries.
-
Radiographic features are most dramatic in infants and children.
-
Most significant changes occur at the metaphysis, physis, and epiphysis.
-
Zone of provisional calcification is thick and sclerotic.
-
Lucent zone (scurvy line) on metaphyseal side of this band
-
Corner sign—beaklike metaphyseal extension with lucent metaphyseal changes
-
Marked periosteal evolution caused by hemorrhages
-
“Ring” epiphyses result from dense provisional zones of calcification at their margins.
-
Osteoporosis in adults
-
Features may return to normal with vitamin C therapy.
-
 |
|
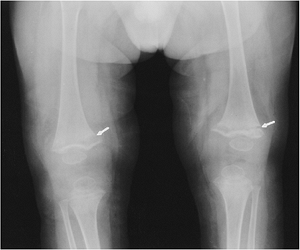
FIGURE 15-33
Hypovitaminosis C in a 10-month-old. Radiographs of the knees showing ringed epiphyses and metaphyseal condensation with fractures (arrows) proximally. |
P.949
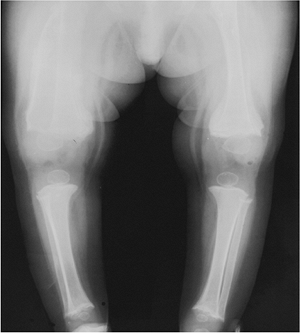 |
|
FIGURE 15-34
Hypovitaminosis C in an 8-month-old. AP radiographs of the lower extremities showing healing subperiosteal hemorrhages, more evident along the femora. |
Suggested Reading
Resnick D, Kransdorf MJ. Hypervitaminosis and hypovitaminosis. In: Resnick D, Kransdorf MJ, eds. Bone and joint imaging, 3rd ed. Philadelphia: Elsevier-Saunders; 2005:1022–1027.
P.950
Vitaminosis: Vitamin D
Key Facts
-
Vitamin D is essential for calcium and phosphorus balance.
-
Hypovitaminosis D (osteomalacia and rickets) was discussed in Chapter 14.
-
Vitamin D intoxication (hypervitaminosis) can be seen in patients treated for skeletal disorders and adults with Paget disease.
-
Patients present with anorexia, vomiting, fever, and abdominal and skeletal pain.
-
Radiographic features are primarily
related to hypercalcemia and metastatic calcification. Calcifications
may occur in vasculature, articular regions, and abdominal viscera. -
Patterns of calcification are not specific (Table 15-3).
|
TABLE 15-3 CONDITIONS ASSOCIATED WITH SOFT TISSUE CALCIFICATION
|
|||
|---|---|---|---|
|
P.951
 |
|
FIGURE 15-35 Vitamin D intoxication. AP radiograph of the foot showing dense amorphous periarticular soft tissue calcification.
|
Suggested Reading
Resnick D, Kransdorf MJ. Hypervitaminosis and hypovitaminosis. In: Resnick D, Kransdor MJ, eds. Bone and joint imaging, 3rd ed. Philadelphia: Elsevier-Saunders; 2005:1022–1027.
P.952
Tumoral Calcinosis
Key Facts
-
Idiopathic tumoral calcinosis typically occurs in males in their 20s and 30s. The condition is more common in black males.
-
Trauma is reported in some cases, and 30% to 40% have a family history.
-
Radiographs or CT reveals periarticular
calcium masses, often forming multiple lobules. The hips, shoulders,
elbows, and ankles are most commonly involved. -
Differential diagnosis includes collagen vascular disorders, chronic renal disease, hyperparathyroidism, and sarcoidosis (Table 15-3).
 |
|
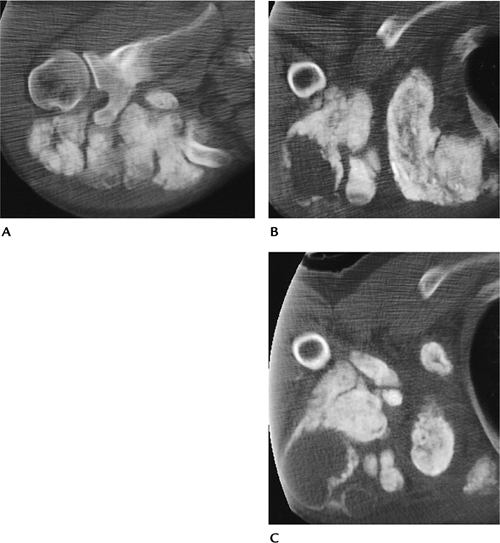
FIGURE 15-36 Tumoral calcinosis. CT images (A–C) of the shoulder demonstrate large loculated calcium masses.
|
Suggested Reading
Kolawole TM, Bohrer SP. Tumoral calcinosis with fluid–fluid levels in tumoral masses. AJR Am J Roentgenol 1974;120:461–465.
P.953
Heavy Metal Disorders
Key Facts
-
Skeletal disorders may be related to lead, aluminum, or copper.
-
Lead intoxication occurs in neonates
whose mothers have lead intoxication or by ingesting lead-containing
paints or inhaling lead-containing fumes. Clinical features may be
acute, with neurologic symptoms, seizures, and abdominal pain, or
chronic, with fatigue and anemia. Radiographic features occur late.
Dense metaphyseal bands are evident radiographically. -
Aluminum intoxication may be seen in
patients on dialysis or those taking aluminum hydroxide. Osteomalacia
is seen radiographically, but features are not specific. -
Copper deficiency is seen in infants undergoing total parenteral therapy. Radiographic features are similar to those of rickets.
 |
|
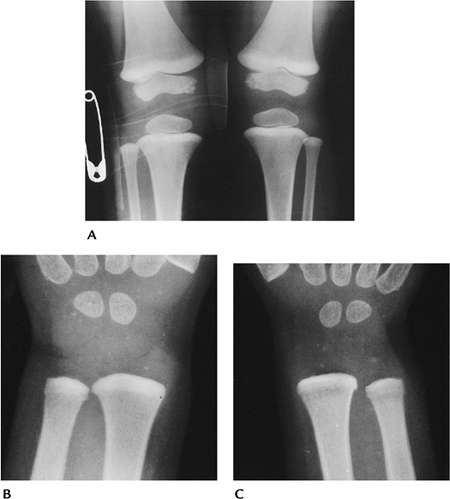
FIGURE 15-37 Lead poisoning. AP radiographs of the knees (A) and both wrists (B,C) showing dense, thick metaphyseal bands.
|
P.954
 |
|
FIGURE 15-38
Heavy metal intoxication. AP radiographs of the knees demonstrate broad bands of sclerosis in the diaphyseal-metaphyseal regions of the tibias and femurs. |
Suggested Reading
Blickman JG, Wilkinson RH, Graef JW. The radiographic lead band revisited. AJR Am J Roentgenol 1986;146:245–247.
P.955
Hemoglobinopathies/Anemias: Basic Concepts
Key Facts
-
Fetal hemoglobin (HbF) comprises 60% to 90% of hemoglobin at birth.
-
Adult hemoglobin (HbA) usually replaces HbF at 4 months of age.
-
HbA consists of paired polypeptide chains. There are two α chains (141 amino acids) and two β chains (146 amino acids).
-
Variations in amino acids on either chain
result in a spectrum of clinical diseases, including sickle cell anemia
and thalassemia.
Suggested Reading
Musely JE. Skeletal changes in the anemias. Semin Roentgenol 1974;9:169–184.
P.956
Hemoglobinopathies/Anemias: Sickle Cell Anemia
Key Facts
-
Sickle cell anemia has differing clinical and radiographic features, depending on the hemoglobin structure.
-
Sickle cell anemias:
• Homozygous (HbS-S) α Chain is normal. Valine replaces glutamic acid on the α chain. Present in 1.3% of U.S. African Americans. • Heterozygous (HbC-S) S gene from one parent and C gene from the other. Present in 1.3% of U.S. African Americans. • Sickle-thalassemia One S gene and one thalassemia gene inherited. -
Clinical symptoms are most common in the homozygous form.
-
Symptoms rare during first 6 months
-
Painful swelling of hands and feet (dactylitis) at 6 months to 2 years
-
Sickle cell crisis in 20s and 30s, with bone pain, fever, anemia, and abdominal pain
-
-
Radiographic features are predominately related to bone infarction, marrow hyperplasia, and complications such as osteomyelitis.
-
Marrow hyperplasia—osteopenia and cortical thinning
-
Vascular occlusion—bone infarction
-
Dactylitis (6 months to 2 years)—osteolytic changes and periosteal reaction
-
Growth deformity—metaphyseal and epiphyseal deformity
-
Vertebral ischemia—H-shaped vertebral body (also seen in thalassemia, Gaucher disease, and hereditary spherocytosis)
-
Osteomyelitis—more than 50% of cases are the result of Salmonella; Staphylococcus is the second most common.
-
P.957
 |
|
FIGURE 15-39 Sickle cell dactylitis. AP radiographs of the feet (A) and right hand (B) showing necrosis of metatarsals with periosteal reaction (arrows) and similar changes in the hand.
|
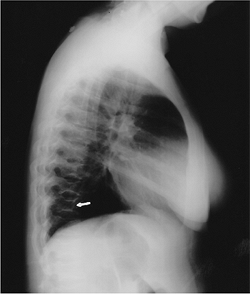 |
|
FIGURE 15-40 H-shaped vertebrae. Lateral radiograph of the thoracic spine showing H-shaped vertebral bodies (arrow) caused by endplate ischemic changes.
|
Suggested Reading
Diggs LW. Bone and joint lesions in sickle cell anemia. Clin Orthop 1967;52:119–144.
P.958
Hemoglobinopathies/Anemias: Thalassemia
Key Facts
-
Thalassemia (Cooley anemia) is a term
derived from Greek meaning “the sea” because the original patients were
of Mediterranean origin. -
Several forms of thalassemia are recognized.
α Thalassemia Abnormal α chain. May affect fetus. β Thalassemia Abnormal β chain. Manifests after HbF is replaced by HbA. Homozygous Thalassemia major Heterozygous Thalassemia minor -
Thalassemia major is diagnosed early and
life expectancy is reduced. α Major (complete absence of α chain) is
most severe; infants die in utero. β Thalassemia is diagnosed in
infancy or early childhood, and anemia is severe. Patients rarely live
beyond their teens. -
Patients with thalassemia minor have mild anemia and splenomegaly.
-
Radiographic features:
-
Marrow hyperplasia—osteopenia, “hair-on-end” appearance in the skull
-
H-shaped vertebrae similar to sickle cell anemia
-
Cortical thinning, marrow expansion, Erlenmeyer flask deformities in femora
-
Growth deformities and pathologic fractures
-
Extramedullary hematopoiesis
-
P.959
 |
|
FIGURE 15-41 Thalassemia major. (A) Lateral radiograph of the skull demonstrating the “hair-on-end” appearance. AP (B) and lateral (C)
radiographs of the knee show marrow expansion, thin cortex with sparse trabeculae, and the Erlenmeyer flask deformity in the femur (B). Radiograph of the hand (D) demonstrating marrow hyperplasia with cystic lesions. Axial CT image (E) shows expansion of the ribs and soft tissue masses caused by extramedullary hematopoiesis. |
P.960
Suggested Reading
Caffey J. Cooley anemia. A review of roentgenographic findings in the skeleton. AJR Am J Roentgenol 1957;78:381–391.
P.961
Sarcoidosis
Key Facts
-
Sarcoidosis is a granulomatous disease of
unknown origin. The presence of noncaseating granulomas suggests
infection is the likely cause. -
Multiple organ systems are affected (Table 15-4). Symptoms are most common when patients are in their 20s to 40s.
-
Pulmonary involvement (bilateral hilar
and right paratracheal adenopathy with or without infiltrates) is
common (90%), but patients may be asymptomatic. -
Other common symptoms include uveitis,
iritis, erythematous rash, and malaise. Fever, weight loss, and
hepatosplenomegaly also are common. -
Musculoskeletal involvement (5%–13%) may be osseous, articular, or muscular in nature.
-
Radiographic features:
-
Subcutaneous nodules (5%)
-
Lacelike or cystic changes in the hands and feet (5%)
-
Axial skeleton and long bone lesions may be lytic or sclerotic
-
Muscle granulomas (often asymptomatic, seen on MRI)
-
Joint swelling and narrowing may occur.
-
 |
|
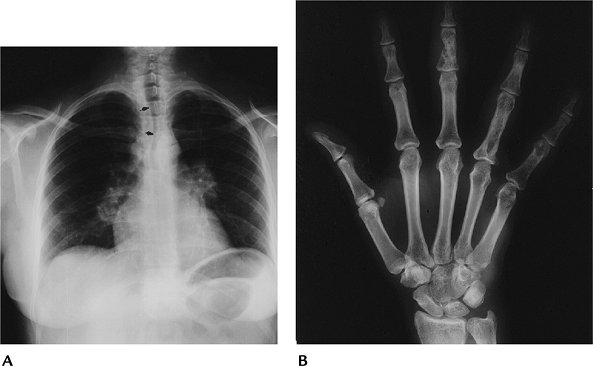
FIGURE 15-42 Sarcoidosis. (A) PA radiograph of the chest showing bilateral hilar and right paratracheal adenopathy. Note the tracheal deviation (arrows). (B)
Radiograph of the right hand showing lacelike trabecular pattern and cystic changes in the third middle phalanx and fourth proximal phalanx. |
P.962
 |
|
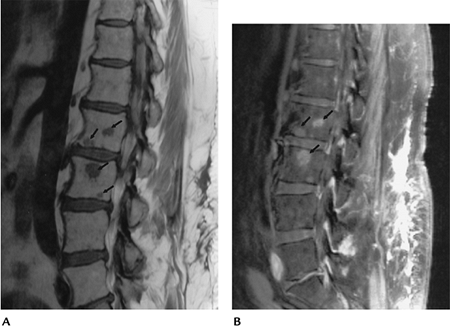
FIGURE 15-43 Sagittal T1- (A) and T2-weighted (B) images of the spine demonstrate multiple lesion (arrows) that would be difficult to differentiate from metastasis.
|
P.963
Suggested Reading
Gunter B. Sarcoidosis. Orthopedics 1995;18:214–218.
Moore SL, Teirstein AE. Musculoskeletal sarcoidosis: Spectrum of appearances at MR imaging. Radiographics 2003;23:1389–1399.
P.964
Diffuse Idiopathic Skeletal Hyperostosis
Key Facts
-
Diffuse idiopathic skeletal hyperostosis
(DISH) is an ossifying diathesis of uncertain cause, but distinct in
clinical and radiographic features from other disorders such as
ankylosing spondylitis. -
Clinical symptoms occur, predominantly in
the elderly, but symptoms (tendinitis, restricted range of joint
motion, and difficulty swallowing with cervical spine involvement)
often are mild compared with radiographic features. -
DISH commonly involves the thoracic
spine, but the cervical and lumbar spine also may be involved.
Extraspinal changes are most common in the pelvis, knees, elbows, heel,
hand, and wrist. -
Heterotopic ossification is common in patients with DISH after hip and knee surgery.
-
Radiographic features:
-
Spine (three criteria): (i) flowing
ossification anterolaterally involving at least four contiguous
vertebrae; (ii) preserved disc height; and (iii) absence of bony
ankylosis. -
Extraspinal features: whiskering at sites of tendon or ligament attachment. Prominent enthesophytes.
-
P.965
 |
|
FIGURE 15-44 DISH. (A)
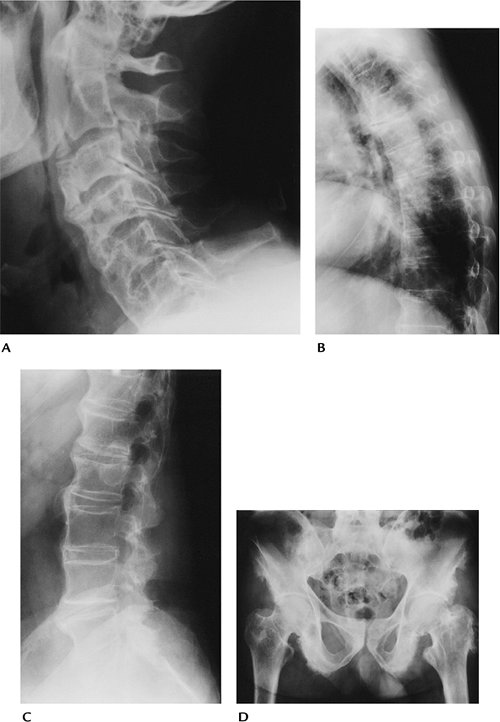
Lateral view of the cervical spine with prominent anterior ossification causing dysphagia. The disc spaces are preserved and at least four segments are involved. (B) Lateral radiograph of the thoracic spine with flowing osteophytic ossification and preserved disc spaces. (C) Lateral view of the lumbar spine with anterior ossification and normal disc spaces. (D) AP radiograph of the pelvis with ischial whiskering and prominent enthesophytes, especially on the left greater trochanter. |
P.966
Suggested Reading
Resnick
D, Niwayama G. Radiographic and pathologic features of spinal
involvement in diffuse idiopathic skeletal hyperostosis (DISH). Radiology 1976;119:559–568.
D, Niwayama G. Radiographic and pathologic features of spinal
involvement in diffuse idiopathic skeletal hyperostosis (DISH). Radiology 1976;119:559–568.
P.967
Gorham Disease (Massive Osteolysis)
Key Facts
-
Gorham disease is of unknown cause. However, pathologic features suggest a vascular derangement.
-
The condition can be seen in males and females at any age, but most are diagnosed before age 40 years.
-
Patients present with pain and swelling in the involved region.
-
Spinal and extra-axial involvement can occur.
-
Radiographic features are dramatic with
progressive osteopenia and fragmentation of bone that can spread to
adjacent osseous or articular structures. -
Serious complications are uncommon unless the spine or chest (respiratory compromise) is involved.
 |
|
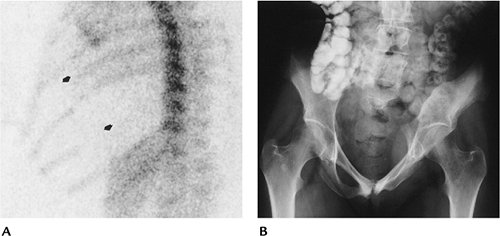
FIGURE 15-45 Gorham disease. (A) Radionuclide bone scan showing absent (no uptake) tenth and distal eighth ribs (arrows). (B) AP radiograph of the pelvis in a different patient with osteolysis of the medial left ilium.
|
Suggested Reading
Heyden G, Kindblom LG, Nielsen JM. Disappearing bone disease. A clinical and histologic study. J Bone Joint Surg 1977;59A:57–61.
P.968
Nonaccidental Trauma (Battered Child Syndrome)
Key Facts
-
More than 200,000 incidents of child abuse are reported yearly in the United States.
-
Most cases occur in children aged less than 6 years. Up to 70% have radiographic abnormalities.
-
Clinical evaluation should include a
skeletal survey to search for single or multiple fractures.
Radionuclide bone scans also are useful in this regard. CT or MRI is
useful when neurologic or central nervous system injury is suspected
clinically. -
Extraskeletal findings include cutaneous
hemorrhage or bruising, malnutrition, chest and internal abdominal
injuries, and subdural hematomas. -
Common fracture sites include the ribs, humerus, femora, tibia, hand, and skull, in order of decreasing frequency.
-
Bilateral fractures and abundant calluses are clues to the diagnosis.
P.969
 |
|
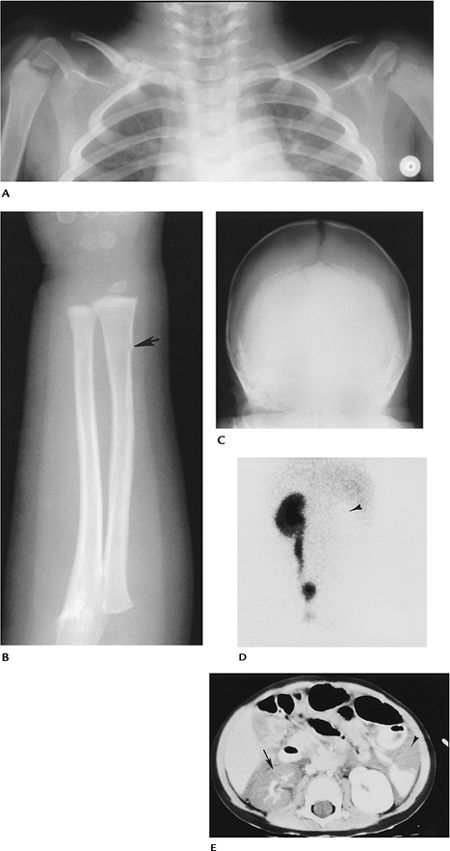
FIGURE 15-46 Nonaccidental trauma. (A) Radiograph of the clavicles shows a fracture of the right midclavicle with abundant callus formation. (B) Radiograph of the forearm shows a subtle torus fracture (arrow). (C) AP radiograph of the skull demonstrating a skull fracture. (D) Renogram in a 14-month-old shows no perfusion in the left kidney (arrowhead). (E) CT image demonstrating fluid in the abdomen with renal (arrow) and splenic (arrowhead) injuries.
|
P.970
Suggested Reading
Dias MS, Backstrom J, Falk J, et al. Serial radiography in the infant shaken impact syndrome. Pediatr Neurosurg 1998;29:77–85.
Kogutt MS, Swischuk LE, Fagan CJ. Patterns of injury and significance of uncommon fractures in battered child syndrome. AJR Am J Roentgenol 1974;121:143–149.
Mogbo KI, Slovis TL, Canady AI, et al. Appropriate imaging in children with skull fractures and suspicion of abuse. Radiology 1998;208:521–524.