
III – Shoulder Reconstruction > Part B – Evaluation and Treatment of
Shoulder Disorders > 30 – Surgical Exposures of the Shoulder
beach-chair or lateral decubitus position. In the beach-chair position,
the head of the bed is elevated approximately 60 degrees. It is lowered
if a concealed axillary approach is planned. The patient is shifted to
the ipsilateral side of the bed, allowing the arm to be put through a
full range of motion without coming into contact with the table. The
head and neck are placed in neutral position and secured with tape to
the head holder. A short arm board is placed on the table just above
the elbow, which can be supplemented after draping by a sterile
bolster. A hydraulic arm positioner can also be used as an alternative
to the short arm board. For the posterior approaches, the patient is
typically placed in a lateral decubitus position.
as cosmetically acceptable as possible. Although the most cosmetically
acceptable incisions follow the Langer skin tension lines, it is also
important to keep in mind sensory dermatomes to avoid neuromas and
hypesthetic areas. Supraclavicular nerves supply sensation to the
superoanterior shoulder, the axillary nerve supplies skin over the
middle deltoid, and the posterior rami of cervicothoracic spinal nerves
supply posterior skin from trapezius to scapula. The vascularity of the
shoulder area is excellent, so flap viability is high despite extensive
undermining in the plane of the deep muscle fascia. Small incisions
also afford a great deal of exposure owing to the mobility of the
shoulder joint, since seemingly hidden pathology can often be brought
into view simply by rotating the arm.
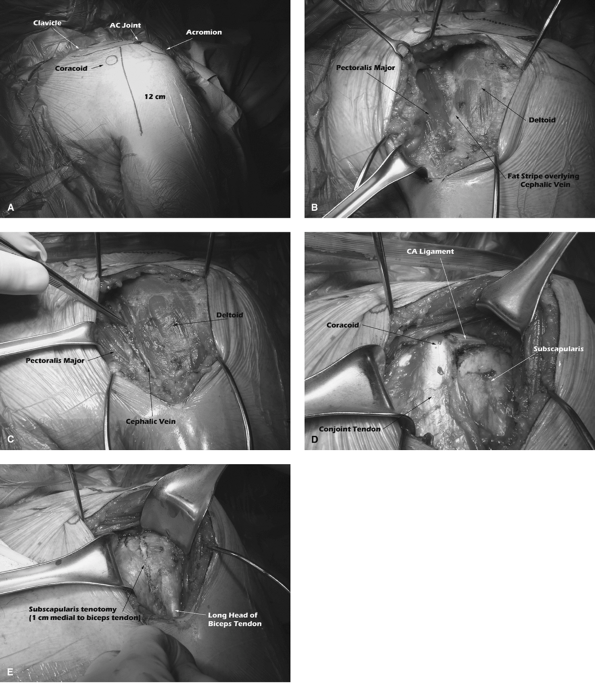
It exploits the internervous plane between the axillary (deltoid) and
medial/lateral pectoral nerves (pectoralis major). The standard
incision is made from just inferior to the clavicle, over the coracoid
process, extending down the arm to the area of the deltoid insertion in
an oblique fashion. Needle-tipped electrocautery is used to create
full-thickness flaps medially and laterally. This dissection extends
superiorly to the clavicle and inferiorly to the insertion of
pectoralis major. Two Gelpi retractors are placed in the superior and
inferior aspects of the wound. The deltopectoral interval is then
identified. It is typically highlighted by a stripe of fat overlying
the cephalic vein, which should be carefully preserved. It is most
convenient to retract the vein laterally with the deltoid, because
there are fewer venous tributaries from the pectoralis than from the
deltoid. Once the vein is freed from the pectoralis and hemostasis is
achieved, the subdeltoid space is identified. The easiest way to
identify this interval accurately is to begin in the subacromial space
and sweep laterally and distally. A Richardson retractor is then placed
beneath the deltoid, and the pectoralis tendon is identified.
proximal 5 to 10 mm of the pectoralis tendon may require release but
should be repaired at the end of the case. Care should be taken when
releasing the pectoralis tendon to avoid injury to the long head of
biceps tendon running immediately laterally. A second Richardson
retractor is then placed deep to the pectoralis muscle, revealing the
clavipectoral fascia. This fascia is then incised just lateral to the
conjoint tendon, and a medium Richardson retractor is placed to retract
the conjoint tendon medially. Whereas both the short head of biceps and
coracobrachialis are tendinous proximally, at the distal portion
of
the wound the short head of biceps muscle belly lies medial to the
tendon of coracobrachialis, so, as the medium Richardson retractor is
placed, care should be taken to avoid placing it in the interval
between the short head of biceps muscle belly and coracobrachialis.
With the conjoint tendon retracted medially, the coracoid and the
coracoacromial ligament are identified. Ideally, the coracoacromial
ligament should be preserved because it is an important part of the
coracoacromial arch, but occasionally the leading edge must be released
to facilitate superior exposure. A Darrach retractor is then placed
beneath the deltoid and used to gently lever the humeral head
anteriorly. The anterior bursa is completely removed, affording clear
visualization of the subscapularis.
 |
|
Figure 30-1 The standard deltopectoral approach. A: Standard deltopectoral incision. B: The deltopectoral interval with overlying fat stripe. C: The cephalic vein identifies the deltopectoral interval. D: The conjoint tendon overlying the subscapularis. E: Incision of the subscapularis tendon.
|
demarcates the upper border of the subscapularis, and the lower border
is recognized by the adjacent leash of vessels. These vessels are
controlled with cautery or ligation. Many options exist regarding
treatment of the subscapularis. The subscapularis can be removed from
the humerus directly from bone, beginning just medial to the biceps
tendon, which is advantageous if there is significant stiffness and
loss of external rotation, since the subscapularis can be repaired back
to bone more medially. The subscapularis tendon can also be divided 1
cm medial to its insertion, or a thin osteotomy of the lesser
tuberosity can be performed, leaving the subscapularis attached to the
bony fragment. The arthrotomy is continued superiorly through the
rotator interval. Care must be taken to protect the axillary nerve and
posterior circumflex humeral artery, which run under the muscular
portion of the subscapularis toward the quadrangular space.
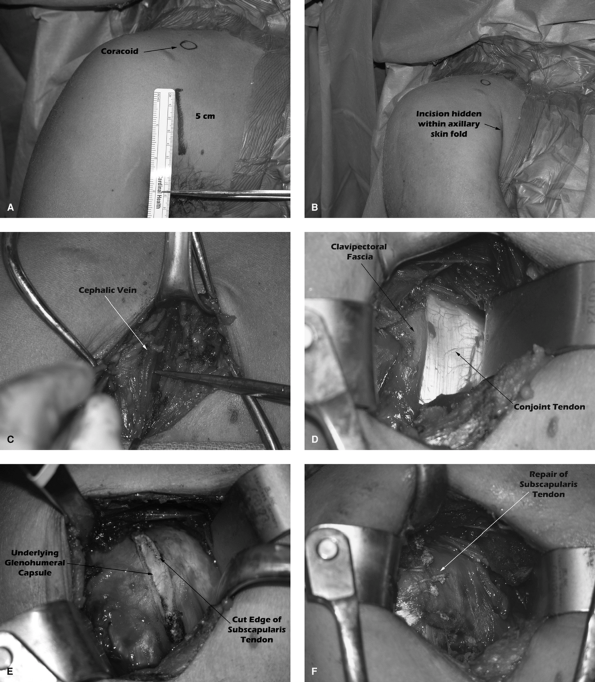
This can be used for shoulder arthroplasty or for anterior
stabilization procedures. Here, the incision strictly follows the
Langer lines. Whereas the traditional deltopectoral approach is
approximately 15 cm in length, the concealed axillary incision begins 3
to 5 cm inferior to the coracoid and extends only 5 to 7 cm into the
axillary crease. Skin flaps are widely elevated, and the deltopectoral
interval is identified. The rest of the approach is the same as in the
deltopectoral. This approach may not give sufficient exposure of the
tuberosities for large rotator cuff tears or for fracture cases.
exits the skin in a 5-cm arc centered just lateral to the coracoid
process. In addition, the average diameter of the humeral head at the
surgical neck is 49 mm. These facts suggest that the minimum incision
length for shoulder arthroplasty is at least 5 cm. A 5-cm incision
centered just lateral to the coracoid process can be used in shoulder
arthroplasty and allows better access to the tuberosities for fracture
cases than the concealed axillary incision. Again, wide subcutaneous
flaps are created and the deltopectoral interval is identified. The
cephalic vein is retracted laterally with the deltoid muscle. The
remainder of the exposure is similar to the standard deltopectoral
approach. Since glenoid exposure is often difficult even with
traditional incisions, minimally invasive approaches should be reserved
for only select patient populations. It is most appropriate for thin
patients with good range of motion.
needs to be more extensile than the standard deltopectoral approach.
The deltopectoral approach is extended distally by extending the
incision along the lateral border of the biceps. The interval between
biceps and brachialis is identified, and the biceps is retracted
medially. Because the brachialis has dual innervation, it can be split
longitudinally along its midline. The periosteum is then split, and
subperiosteal dissection allows safe exposure of the humeral shaft. The
radial nerve pierces the intermuscular septum 10 cm proximal to the
lateral epicondyle of the humerus.
rotator cuff tear and can also be used for shoulder arthroplasty in the
setting of a massive rotator cuff tear. The skin incision is made
extending from the anterior lip of the acromion 8 cm distally in line
with the deltoid fibers. Dissection is carried through subcutaneous
tissue with cautery, and full-thickness flaps are raised anteriorly and
posteriorly at the level of the superficial deltoid fascia. There is an
avascular raphe separating the anterior and middle thirds of the
deltoid, which is identified and incised from its acromial attachment
distally to a point approximately 4 cm from the acromion. A stay suture
is placed at the distal edge of the deltoid split to prevent
propagation of the split beyond 5 cm, where the axillary nerve is known
to lie. Richardson retractors are placed to retract the anterior
deltoid anteriorly and the middle deltoid posteriorly. A complete
bursectomy is then performed, allowing excellent exposure of the
rotator cuff tear anatomy or, if the cuff is absent, the glenohumeral
joint. Detachment of the deltoid origin from the lateral acromion is
considered a last resort for increased exposure because of the
postoperative complication of deltoid rupture, which is often not
salvageable. If some fibers of deltoid origin are detached, it should
be done strictly subperiosteally so that a cuff of stout tissue remains
for repair.
studied and is considered an improvement over larger incisions that
detach some of the deltoid origin. The approach consists of a 3- to
4-cm incision, which is often an extension of a previously placed
midlateral arthroscopy portal. It is carried to the superficial deltoid
fascia, above which full thickness flaps are elevated. The superficial
deltoid fascia is then split in line with its fibers, again taking care
to avoid propagating the split beyond 5 cm distal to the lateral edge
of the acromion. The deltoid is then divided, exposing the
subdeltoid/subacromial bursa. A bursectomy is performed, which allows
excellent direct visualization of the rotator cuff, the anatomy of the
cuff tear, and the cuff footprint on the greater tuberosity.
deltopectoral and anterosuperior approaches can be exploited. This
allows, in addition to the excellent deltopectoral exposure,
visualization of the posterior glenohumeral joint and posterior cuff,
especially the infraspinatus. If this approach is planned
preoperatively, the standard deltopectoral skin incision is made
slightly more laterally; otherwise, the combined
approach
can be done through the standard deltopectoral incision. Again, large
full thickness flaps of skin are created and mobilized extensively. The
deltopectoral approach is performed as described previously and then a
second approach is made between the anterior and middle deltoid as
described in the anterosuperior approach, but both approaches are made
through the same deltopectoral incision.
 |
|
Figure 30-2 The concealed axillary approach. A: The concealed axillary incision. B: With the arm adducted, the incision is hidden in the axillary fold. C: Identification of the cephalic vein by mobilizing full-thickness skin flaps. D: Identification of the conjoint tendon. E: Incision of the subscapularis tendon. F: Repair of the subscapularis tendon.
|
 |
|
Figure 30-3 The posterior approach. A: The skin incision. B: Retraction of the deltoid and identification of the interval between infraspinatus and teres minor. C: Incision of the infraspinatus and dissection off the posterior capsule. D: Capsulotomy exposing the glenohumeral joint.
|
prone. An incision is made vertically following the Langer lines along
a line drawn from the posterolateral lip of the acromion to the
posterior axillary fold, centered 2 cm beneath the acromion.
Full-thickness flaps are raised at the level of the deep fascia. The
deltoid as well as its superficial and deep fascia is split in line
with its fibers. This deltoid split must not propagate beyond the teres
major to avoid injury to the axillary nerve. The internervous plane
between infraspinatus (suprascapular nerve) and teres minor (axillary
nerve) is used for this approach. It is most easily identified at the
medial aspect of the wound proximal to the musculotendinous junction
and is often marked by a stripe of fat. It is important, however, that
the dissection stays lateral to the glenoid neck to avoid injury to the
suprascapular nerve. On entering the interval between infraspinatus and
teres minor, the posterior joint capsule is apparent.
 |
|
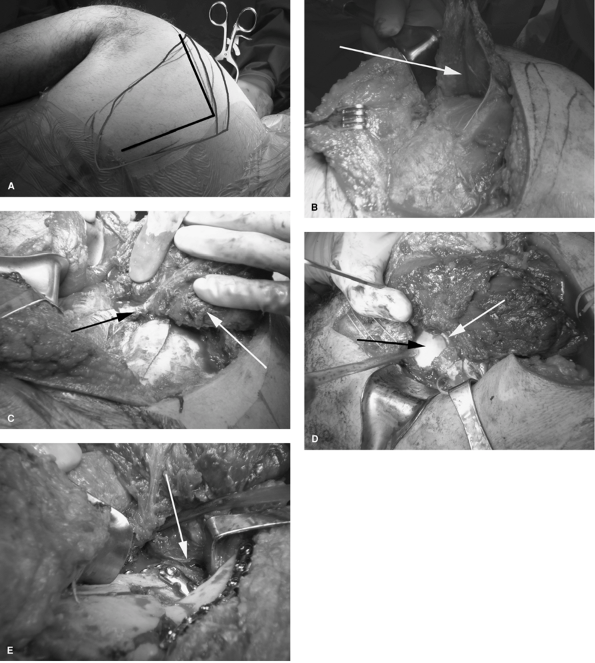
Figure 30-4 Judet Approach. A: Skin incision. B: Detachment of the deltoid from the scapular spine. C: Reflection of the infraspinatus muscle (white arrow) on the suprascapular neurovascular pedicle (black arrow). D: Exposure of the posterior glenohumeral joint (white arrow indicates glenoid, black arrow indicates humera head). E: Final placement of hardware on glenoid neck, posterior glenoid, and scapular spine (arrow indicates reduced glenoid fragment).
|
The patient is positioned prone, and the skin incision begins at the
posterolateral lip of the acromion, extends along the spine of the
scapula, and turns at a right angle inferiorly along the medial border
of the scapula. The posterior deltoid is elevated off the spine of the
scapula. The underlying infraspinatus is elevated off the medial border
of the scapula and retracted laterally on its suprascapular
neurovascular pedicle, while care is taken to protect the pedicle.