
III – Emergency Department > 11 – Carpal Injuries > 11.2 – Carpal
Instabilities and Fracture-Dislocations of the Carpus
integrity due to acute traumatic dislocations or ligamentous laxity. It
implies the loss of the ability to maintain normal kinematic and
kinetic functions and relationships under static conditions and or
functional loads between the radius, carpal bones and metacarpals. In
the broader definition of carpal instabilities used in this chapter,
they may be associated with certain fracture dislocations of the
carpus, and include isolated carpal dislocations and adaptive
instabilities secondary to malunions of distal radius fractures.
refers to carpal instability that is reproduced or demonstrated on
physical examination maneuvers, and may often be demonstrated on stress
radiographs. Static instabilities are usually associated with complete
ligamentous disruption, whereas dynamic instabilities are usually
associated with a partial or incomplete ligamentous disruption. Dynamic
carpal instability is said to be the most common cause of wrist pain
and carpal instability in adolescents and young adults. It is most
likely due to attenuation of the palmar radioscaphoid and scapholunate
interosseous ligaments.
region of the SL ligament have been shown to be associated with
symptoms and signs of dynamic scapholunate instability.
carpus as a ring that allows reciprocal motion between the proximal and
distal rows during radial and ulnar deviation, and during flexion and
extension. The scaphoid is considered to be the stabilizing link
between these two rows, and the triquetrum is said to be the pivot
point for carpal rotation. Any interruption of the ring in the proximal carpal row results in carpal instability.
or suspended between the radius/ulna and the distal carpal row/hand.
Some have called the proximal carpal row a “free body in space.” This
oversimplification is amplified by noting that the radius
of
curvature of the proximal pole of the scaphoid and the lunate are
different (the lunate has a greater radius). This finding fits with the
interosseous scapholunate ligament anatomy that demonstrates thick and
unyielding fibers dorsally compared to the palmar portions of the
ligament that are less dense and more elastic. These two facts (among
others) account for the different rates or ratios of movement that
demonstrate equal rotation of these two bones in wrist extension, but
show greater rotation of the scaphoid in wrist flexion. This
observation is but a small example of the complexity of the kinematics
of the wrist, and the reader is referred to the Suggested Reading list
for additional study.
 |
|
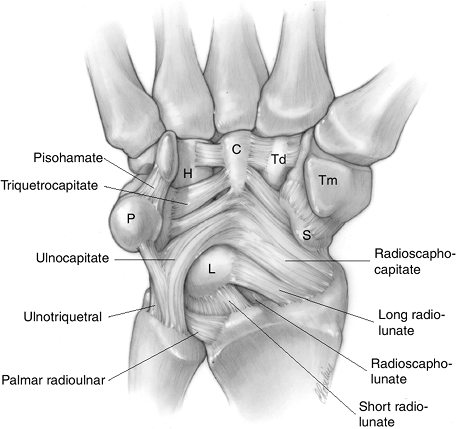
Figure 11.2-1 The palmar radiocarpal ligaments (see text for details).
|
concepts of carpal kinematics will be enhanced by a review of the
current description and terminology of the carpal ligaments.
ligaments, including the radioscaphocapitate, long radiolunate
(previously named the radiotriquetral and also the radiolunotriquetral)
and short radiolunate, radioscapholunate, pisohamate,
triquetrocapitate, ulnocapitate, ulnotriquetral and palmar radioulnar
ligaments.
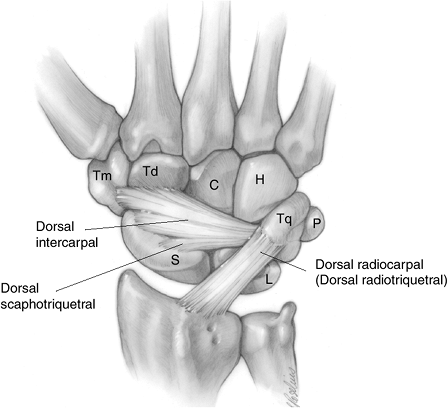
ligaments, including the dorsal intercarpal, dorsal scaphotriquetral,
and dorsoradiocarpal (sometimes called the dorsal radiotriquetral)
ligaments.
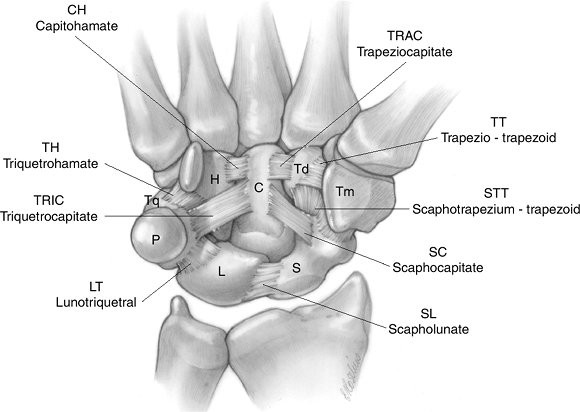
capitohamate, triquetrohamate, triquetrocapitate, lunotriquetral,
scapholunate, scaphocapitate, scaphotrapezium-trapezoid,
trapeziotrapezoid, and trapeziocapitate ligaments. The scapholunate
(SL) ligament is divided into three parts: dorsal (the most substantial
part), proximal, and palmar. It is the main stabilizer of the scaphoid
that prevents it from flexing under load. In contrast to the SL
ligament, the lunotriquetral (LT) ligament is more substantial in its
palmar aspect
as an aid to understanding some of the more common patterns of carpal
instability.
of the major interosseous ligaments involving the same carpal row. It
is termed dissociative because there is
separation or dissociation between at least two carpal bones. Common
examples of CID are scapholunate dissociation, lunotriquetral
dissociation, unstable scaphoid fracture, and perilunate dislocation.
Examples of scapholunate dissociation and lunotriquetral dissociation
are given in Figures 11.2-4 and 11.2-5.
dissociation allows us to add two other compound terms that the reader
will encounter in descriptions of these injuries.
 |
|
Figure 11.2-2 The dorsal radiocarpal ligaments (see text for details).
|
 |
|
Figure 11.2-3 Palmar midcarpal and proximal- and distal-row interosseous ligaments (see text for details).
|
deformity. If scapholunate dissociation is present for a prolonged
period of time, it will result in a scapholunate advanced collapse
deformity, with severe arthritis in the radioscaphoid and midcarpal
region.
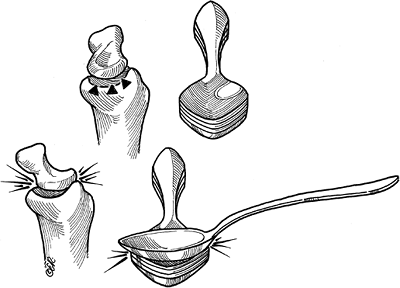
articulates with the scaphoid is elliptical, and dorsal scaphoid
dissociation or subluxation results in incongruity between the scaphoid and the scaphoid fossa in the radius. This is
analogous to two superimposed and co-linear tea spoons that normally
are co-linear but then one spoon (scaphoid) rotates into noncolinear
alignment. The result of this incongruous alignment is arthritis. Figure 11.2-7 demonstrates the mechanism for development of a SLAC arthrosis.
 |
|
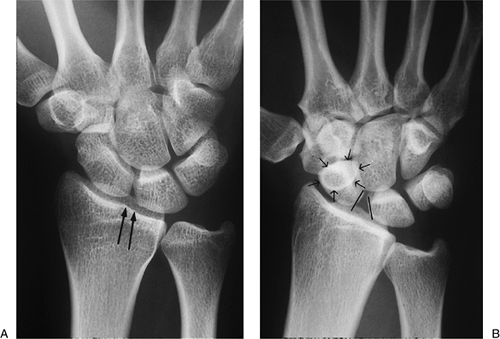
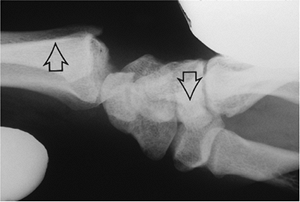
Figure 11.2-4 Comparison of x-ray findings in a normal wrist and in one with a scapholunate dissociation. A.
The normal appearance of the wrist in the AP view. Note the uniform spacing of the carpal bones, and more specifically, the parallel alignment of the articular interface between the proximal pole of the scaphoid and the lunate (parallel vertical arrows). B. A scapholunate dissociation showing a widened and nonparallel space between the scaphoid and lunate, a foreshortened scaphoid, and a positive “ring sign” (arrows in a circle). |
 |
|
Figure 11.2-5
A lunotriquetral dissociation as shown by an arthrogram. Note the presence of radio-opaque dye in the space between the lunate and triquetrum (opposing arrows), indicating disruption of the lunotriquetral ligament. |
between the proximal pole of the scaphoid and the adjacent lunate or
between the lunate and the triquetrum. CIND is often referred to as
midcarpal instability. This condition refers to carpal instability that
is characterized by a major noninterosseous ligament injury that could
be seen in dorsal or palmar carpal subluxation/dislocation and ulnar
translation. It is termed radiocarpal CIND. Figure 11.2-8 represents an example of CIND in a patient with palmar radiocarpal dislocation.
characterized by midcarpal instability, such as capitate lunate
instability (CLIP wrist), palmar or dorsal midcarpal instability, and
medial anteromedial instability (MAMI). Symptoms are often present as a
painful wrist clunk that is reproduced by pronation, axial compression,
and ulnar deviation. The sequence of events is as follows: with radial
deviation, the proximal row palmar flexes; during ulnar deviation,
there is loss of the normal synchronous (or smooth) movement of the
proximal row, and it “jumps” rather than glides into extension; this
precipitous catch-up movement or clunk reproduces the patient’s
symptoms.
instability involves or impairs the relationship of the bones in the
same row (CID type) and the relationship
between rows (CIND type). Dorsal perilunate dislocation, trans-scaphoid
perilunate fracture dislocation, trans-scaphoid trans-capitate
dislocation, and trans-triquetrum perilunate fracture dislocation are
all types of CIC injuries. The first two injuries are the most common.
 |
|
Figure 11.2-6 DISI deformity as seen in an established scapholunate dissociation. A. AP view of the wrist showing a widened scapholunate space (vertical arrows). B. Note the dorsally rotated lunate (arrows) on the lateral view.
|
Slower loading forces (injuries) are usually associated with carpal
fractures, in contrast to faster loading forces that usually produce a
purely ligamentous injury.
 |
|
Figure 11.2-7 Artist’s depiction of the pathomechanics of the SLAC arthrosis (see text for details).
|
carpal instability that results from dorsal angulation of the distal
radius in malunited fractures of the distal radius. This term is used
to differentiate or distinguish this instability from those midcarpal
instabilities that are intrinsic to the carpus. The deformity in the
radius leads to a secondary malalignment of the proximal carpal row,
loss of wrist flexion and radiocarpal or midcarpal instability.
 |
|
Figure 11.2-8 Lateral x-ray view, showing a radiocarpal palmar subluxation. This was a stress radiograph (arrows).
|
wrist, and there is tenderness over the radiocarpal and midcarpal
region, along with an obvious deformity of the wrist. Corrective
osteotomy of the radius may help in re-alignment of the carpus.
-
This maneuver is a physical examination
technique that aids in the diagnosis of scapholunate dissociation. It
is performed with the forearm in slight pronation. -
This maneuver is performed by applying
pressure over the palmar tubercle of the scaphoid by the examiner’s
thumb with the wrist in ulnar deviation and slight extension. -
Pressure is maintained on the distal pole
of the scaphoid and then the wrist is brought into radial deviation and
slight flexion.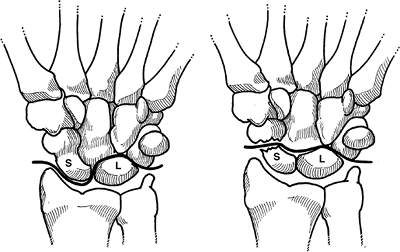 Figure 11.2-9 The lesser and greater carpal arcs (see text for details).
Figure 11.2-9 The lesser and greater carpal arcs (see text for details).-
In wrists with this
form of instability (SL), the proximal pole of the scaphoid is
displaced dorsally over the lip of the radius.
-
-
Release of the thumb pressure causes the scaphoid’s dorsally displaced proximal pole to return to its anatomic position in the scaphoid fossa of the radius, and a palpable (and usually painful) “clunk” or “pop” may be noted (Figure 11.2-11).
-
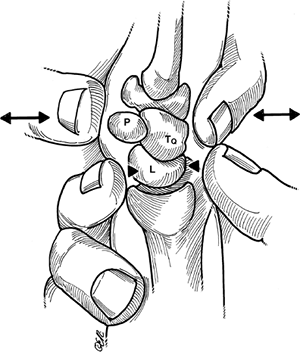
The ballottement test or maneuver is used to identify abnormal motion or tenderness at the lunotriquetral junction.
-
It is done by firmly fixing the lunate
with the examiner’s thumb and index finger of one hand while the
pisiform and triquetrum are displaced dorsally and volarly with the
other hand’s thumb and index finger (Figure 11.2-12). -
A positive test is revealed by pain, and indicates lunotriquetral instability.
-
Various forms of compression,
distraction, and translation may reveal abnormal mobility or pain
patterns with these motions, and can be indicative of various types of
instability about the wrist as previously described. -
Some patients may be able to reproduce
various clunks and abnormal movements about the wrist that may
sometimes aid the astute examiner in establishing a diagnosis.
-
Imaging techniques include standard x-ray
views such as the PA and lateral, PA in radial and ulnar deviation, and
lateral views in flexion and extension, as well as AP and lateral views
with a fist. -
The Moneim view is taken with the wrist elevated on the ulnar side by a sponge pad.
-
This view facilitates observation of the
space between the proximal pole of the scaphoid and the adjacent
lunate, and will often reveal a scapholunate separation that may not be
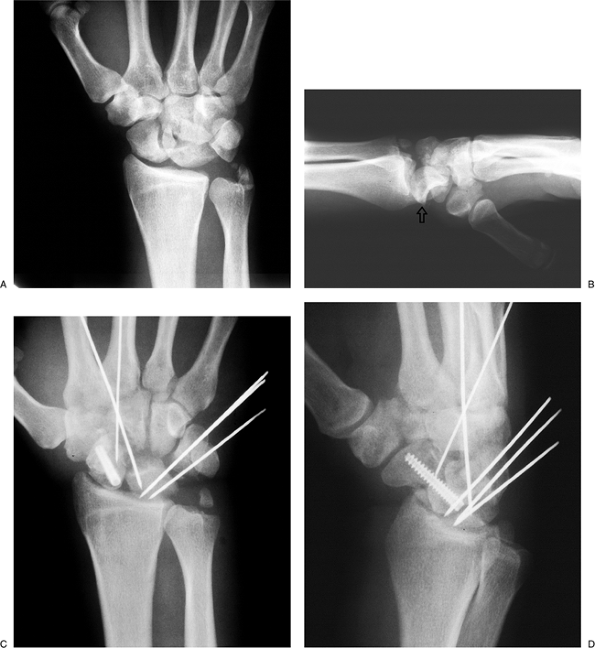
seen on the regular PA films.P.175![]() Figure 11.2-10 Trans-scaphoid-perilunate fracture dislocation. A. PA view showing the loss of continuity of the carpal arcs described by Gilula (see Figure 11.2-13). B. Lateral view of the palmar-flexed lunate (vertical open arrow) and dorsal displacement of the remaining carpus around the lunate. C, D.
Figure 11.2-10 Trans-scaphoid-perilunate fracture dislocation. A. PA view showing the loss of continuity of the carpal arcs described by Gilula (see Figure 11.2-13). B. Lateral view of the palmar-flexed lunate (vertical open arrow) and dorsal displacement of the remaining carpus around the lunate. C, D.
Internal fixation techniques used to restore the architectural
integrity of the carpus. (Courtesy of H. Relton McCarroll, Jr., MD, San
Francisco)P.176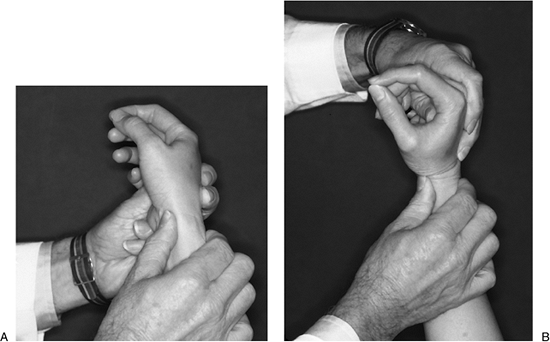 Figure 11.2-11 The scaphoid shift maneuver for a SL dissociation (see text for details).
Figure 11.2-11 The scaphoid shift maneuver for a SL dissociation (see text for details).
-
-
Similarly, PA views with radial and ulnar deviation may show a separation that may not be seen on regular films.
-
Axial loading or compression of the
carpus by making a fist often demonstrates a scapholunate separation
that might not be present on routine radiographs.![]() Figure 11.2-12 Ballottement maneuver for LTD (see text for details).
Figure 11.2-12 Ballottement maneuver for LTD (see text for details).
-
-
Additional imaging techniques include arthrography with or without videofluoroscopy, bone scans, tomograms, and a CT or MRI.
-
A tomogram or CT is a useful aid in evaluating associated fractures. At this point in time, an MRI is less helpful.
-
-
An arthrogram is cost effective and, when
done as a triple phase injection, may provide useful information about
the midcarpal, radiocarpal, and distal radioulnar articulation.-
Contrast material injected into the
midcarpal joint should not extend into the radiocarpal joint unless
there is a ligament disruption in the proximal row (see Figure 11.2-5).
-
-
An arthrogram is easy to obtain, and has been most helpful in terms of revealing disruption of the interosseous ligaments.
-
Arthroscopy of the wrist is preferred
over an arthrogram by some surgeons, and may be more accurate in
determining the extent of ligament injury and the status of the
cartilage surface.
-
-
A bone scan is nonspecific, although it may reveal inflammatory changes about the joint.
-
Gilula identified three unbroken arcs
that mark the articular margins of the proximal and distal carpal row
in the PA x-ray view of the wrist. A set-off in any of these arcs or
lines indicates an intercarpal derangement at the site where the line
is offset (Figure 11.2-13). -
Most articulating bones have a space
between them that is usually 2 mm or less, and any overlap greater than
4 mm is suggestive of a carpal joint abnormality.P.177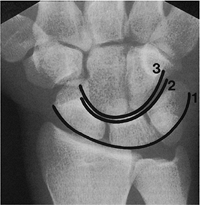 Figure 11.2-13 Gilula lines demarcating the proximal and distal carpal rows.
Figure 11.2-13 Gilula lines demarcating the proximal and distal carpal rows. -
In PA-neutral x-ray views of the wrist, the lunate normally has a trapezoidal shape. If the lunate is triangular in shape, it suggests a malrotated lunate (either flexed or extended).
 |
|
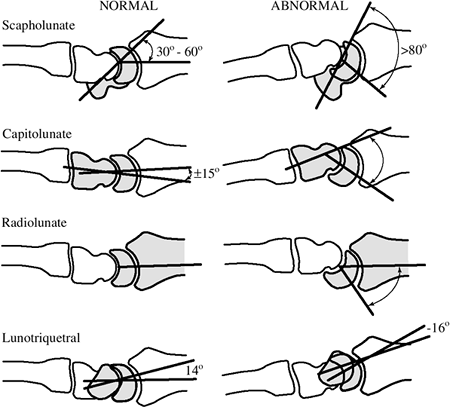
Figure 11.002-14 Useful carpal angles (see text for details).
|
-
Commonly used measurements made from
lateral wrist radiographs are the scapholunate angle, the capitolunate
angle, the radiolunate angle, and the lunotriquetral angle. -
These angles are depicted in Figure 11.2-14.
-
The SL angle is measured by a line drawn
through the longitudinal axis of the scaphoid from the distal to
proximal pole, and by a line drawn through the horizontal axis of the
lunate. -
Normal values range from 30 to 60 degrees, with an average of 47 degrees.
-
Angles greater than 70 to 80 degrees are a definite indication of SL dissociation.
-
Although the longitudinal axes of the
radius, lunate, capitate, and third metacarpal are not usually
colinear, the CL angle is useful when studying midcarpal (CIND)
instabilities. -
A line is drawn that is perpendicular to a line that connects the palmar and dorsal tips of the lunate.
-
The capitate axis is represented by a
line drawn from a point in the center of the convexity of the capitate
head to a point at the center of its distal articular surface. -
Theoretically, the normal CL axis should
be 0 degrees with the wrist in neutral, but what is considered normal
ranges to 15 degrees.
-
A line is drawn that is perpendicular to a line that connects the palmar and dorsal tips of the lunate.
-
The angle formed by this line and the longitudinal axis of the radius is the RL angle.
-
An RL angle greater than 15 degrees is abnormal, and such a finding is associated with DISI and VISI deformities.
-
The lunotriquetral angle represents that
angle formed by a line drawn through the horizontal (longitudinal axis)
axis of the lunate and a line drawn through the longitudinal axis of
the triquetrum. -
The accurate assessment of these axes is difficult to determine.
-
The average normal angle is 14 degrees.
-
In lunotriquetral dissociation, the angle averages -16 degrees.
-
Scapholunate dissociation is one of the most common forms of carpal instability.
-
Common findings that may be noted on
plain radiographs are foreshortening of the scaphoid, the appearance of
a ring in the distal pole of the scaphoid, lack of parallel apposition
of the adjacent articular surfaces of the scaphoid and lunate, widening
of the space between the proximal pole of the scaphoid and the lunate,
and an increased scapholunate angle (Figure 11.2-4).
-
Treatment options may vary according to
many factors, which include the location of the instability, the
underlying cause, the length of time from injury to treatment, the
presence or absence of secondary deformities and arthrosis, and whether
the instability is static or dynamic. -
In general, surgical treatment is based on the principles of carpal realignment and restoration of normal carpal kinematics.
-
Attempts to achieve these two principles have included ligamentous reconstruction and capsulodesis of various forms, arthrodesis of various types, carpectomy and realignment osteotomy of the radius in CIA types of instability.
-
A detailed discussion of these techniques
is beyond the scope of this text. New techniques and methods will no
doubt evolve as the understanding of this complex joint grows.
PC, Taleisnik J. Fractures of the carpal bones. In: Green DP, Hotchkiss
RN, Pederson WC, eds. Green’s operative hand surgery. 4th Ed. New York:
Churchill Livingstone, 1999:809–864.
G. Capsulodesis in reconstructive hand surgery. Dorsal capsulodesis for
the unstable scaphoid and volar capsulodesis following excision of the
distal ulna. Hand Clin 1987;3:81–102.
TT, Gelberman RH, Cooney WP. Carpal Instability. In Trumble TE, ed.
Hand surgery update 3, hand, elbow and shoulder. Rosemont, IL: Amer.
Soc Surg Hand, 2003:205–216.
JR, Botte MJ. Surgical anatomy of the hand and upper extremity. Chapter
1, Skeletal anatomy, pp. 1–91; Chapter 4, Vascular anatomy, pp.
237–293; Chapter 9, The wrist, pp. 486–531, Philadelphia: Lippincott
Williams & Wilkins, 2002.
M. Carpal instabilities and dislocations. In: Green DP, Hotchkiss RN,
Pederson WC, eds. Green’s operative hand surgery. 4th Ed. New York:
Churchill Livingstone, 1999:865–928.
WB. Dynamics of carpal instability. In: Watson HK, Weinzweig J, eds.
The wrist. Philadelphia: Lippincott, Williams and Wilkins, 2001:456–481.
WB, Carroll CT. Scapho-trapeziotrapezoid arthrodesis for treatment of
chronic static and dynamic scapho-lunate instability: a 10-year
perspective on pitfalls and complications. J Hand Surg 1990;15:408–414.
VD, Trumble TE: Scaphoid fractures and nonunions. In Trumble TE, ed.
Hand surgery update 3, hand, elbow and shoulder. Rosemont, IL: Amer.
Soc Surg Hand, 2003:161–173.
MJ, Cooney WP III, Hahn ME, et al. The effects of dorsally angulated
distal radius fractures on carpal kinematics. J Hand Surg
1990;15:721–727.
MD, Meyer NJ. Carpal fractures excluding the scaphoid. In Trumble T,
ed. Hand surgery update 3, hand, elbow and shoulder. Rosemont, IL:
Amer. Soc Surg Hand, 2003:175–187.
ET, Shin AY. Fracture dislocations of the carpus. In Trumble T, ed.
Hand surgery update 3, hand, elbow and shoulder. Rosemont, IL: Amer.
Soc Surg Hand, 2003:189–204.
HK, Ballet FL. The SLAC wrist: scapholunate advanced collapse pattern
of degenerative arthritis. J Hand Surg 1984;9:358–365.