
Editors: Frassica, Frank J.; Sponseller, Paul D.; Wilckens, John H.
Title: 5-Minute Orthopaedic Consult, 2nd Edition
Copyright ©2007 Lippincott Williams & Wilkins
> Table of Contents > Shoulder Anatomy and Examination
Shoulder Anatomy and Examination
Constantine A. Demetracopoulos BS
Timothy S. Johnson MD
Description
-
Bones:
-
Glenohumeral joint:
-
The humeral head articulates with the glenoid fossa of the scapula.
-
Stabilized by the glenohumeral ligaments (1) capsule and rotator cuff muscles
-
The labrum of the glenoid deepens the joint and enhances stability.
-
-
AC joint:
-
The acromion process of the scapula articulates with the distal clavicle.
-
Suspends the arm and scapula
-
-
Sternoclavicular joint:
-
The sternum articulates with the proximal end of clavicle.
-
Suspends the arm and scapula
-
-
Scapulothoracic joint:
-
Consists of the body of the scapula and the muscles covering the posterior chest wall
-
Contributes to shoulder flexion and rotation
-
-
-
Muscles:
-
The trapezius, levator, rhomboids, and serratus anterior stabilize the scapula to aid motion at the glenohumeral joint.
-
Deltoid: Flexor, abductor, and extensor
-
Rotator cuff:
-
Supraspinatus: Abductor and external rotator
-
Infraspinatus: External rotator
-
Teres minor: External rotator
-
Subscapularis: Internal rotator and adductor
-
-
Pectoralis major: Adductor
-
Coracobrachialis and biceps: Flexors
-
-
Nerves:
-
Brachial plexus:
-
Passes through the axilla
-
Branches originate in the neck from C5–T1.
-
-
Axillary nerve:
-
Innervates the deltoid
-
May be injured in anterior shoulder dislocations
-
-
Musculocutaneous nerve: Innervates the biceps and coracobrachialis
-
Signs and Symptoms
History
Thorough history of the mechanism of injury and the nature of pain
Physical Exam
-
Initial assessment:
-
Assess the cervical spine and elbow.
-
Perform a complete neurovascular examination of the extremities.
-
Assess the contralateral shoulder for comparison.
-
-
Inspection:
-
Expose both upper extremities from the shoulder girdle to the hand, inspecting for asymmetry, atrophy, and scapular winging.
-
-
Palpation:
-
Palpate the sternoclavicular joint,
clavicle, AC joint, coracoid, acromion, glenohumeral joint, bicipital
groove, and the greater and lesser tuberosities of the humerus. -
Localize the pain.
-
-
ROM:
-
Compare active and passive ROM.
-
Forward flexion: 180°
-
Extension: 50–60°
-
-
Motion:
-
Assess in adduction and abduction.
-
Distinguish glenohumeral motion from combined glenohumeral and scapulothoracic motion (combined values).
-
External rotation: 80–90°
-
Internal rotation: 60–80°
-
Abduction: 160–180°
-
-
Tests
-
Biceps tendinitis:
-
Pain to palpation in the bicipital groove, found anteriorly on the shoulder with the arm at 10° of internal rotation
-
Yergason test:
-
Test resisted forearm supination with the elbow flexed at 90°.
-
Test is positive when pain is reproduced in the bicipital groove.
-
-
Speed test:
-
With the elbow extended, the forearm
supinated, and the shoulder flexed at 60°, ask the patient to resist
additional forward flexion of shoulder. -
The test is positive when pain is reproduced in the bicipital groove.
-
-
-
Subacromial bursitis:
-
Presentation is very similar to that of rotator cuff tendinitis.
-
Patient may present with subacromial crepitus.
-
-
Rotator cuff tear (2) (Fig. 1):
-
Diffuse, dull, aching pain localized over the deltoid and upper arm
-
Pain with overhead activities
-
Tenderness to palpation over the greater tuberosity of the humerus
-
Test individual rotator cuff muscles for weakness and or pain.
-
Supraspinatus: Test the patient’s
strength in active arm elevation in the plane of the scapula with the
patient’s thumb pointing down. -
Infraspinatus and teres minor: Test the
patient’s strength in active external rotation with the patient’s arm
at the side and the elbow flexed at 90°. -
Subscapularis (“belly press” test): Place
both of the patient’s hands on his/her belly; have the patient press
the belly inward while thrusting elbows forward; the test is positive
if the elbow cannot be actively moved forward.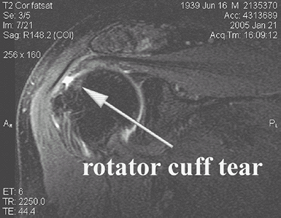 Fig. 1. MRI image of a supraspinatus tendon tear.
Fig. 1. MRI image of a supraspinatus tendon tear.
-
-
Neer sign:
-
Elevate the arm while stabilizing the scapula.
-
Positive sign: Pain at maximal elevation
-
-
Hawkins test:
-
With the patient’s elbow flexed at 90°, forward flex the shoulder to 90° and internally rotate the humerus.
-
The test is positive if pain is reproduced on contact of the greater tuberosity with the acromion.
-
-
Painful arc:
-
Active abduction in the coronal plane
-
The test is positive with pain at 60–100° of abduction.
-
Pain is common in tendinitis and small rotator cuff tears
-
-
Drop-arm test:
-
Inability to hold arm up when passively positioned into an elevated position
-
Suggests a large tear
-
-
Weakness, inability to elevate, and passive ROM that exceeds active ROM also suggest rotator cuff tear.
-
Popeye sign:
-
The biceps resembles a “Popeye” muscle when resisted elbow flexion is tested.
-
Indicates a proximal rupture of the biceps tendon
-
Note: Also occurs with distal biceps tendon rupture
-
P.391 -
-
Shoulder instability (3):
-
History of previous dislocations
-
Patient complains of instability with or without pain.
-
Anterior instability: Apprehension with 90/90 positioning (90° of abduction and 90° of external rotation)
-
Posterior instability: Apprehension with humeral forward flexion in internal rotation
-
Load and shift test:
-
With the humerus in a neutral position on the glenoid, axially load the humerus and shift the head anteriorly and posteriorly.
-
Excessive translation resulting in palpable subluxation and/or dislocation is a positive finding.
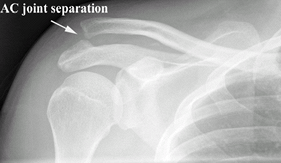
![]() Fig. 2. Radiograph of an AC joint separation.
Fig. 2. Radiograph of an AC joint separation.
-
-
Sulcus sign:
-
With the affected elbow flexed, apply inferior traction to the arm and look for skin dimpling near the lateral acromion.
-
Dimpling indicates inferior instability.
-
-
-
AC joint arthritis/AC separation (4):
-
Palpable point tenderness at the AC joint
-
Palpable step-off at the AC joint in the presence of a separation (Fig. 2)
-
Joint effusion may be present.
-
Cross-body adduction test:
-
With the shoulder at 90° of flexion, passively adduct the arm.
-
The test is positive when pain is reproduced at the AC joint.
-
-
-
Labrum abnormality (Fig. 3):
-
Patient describes pain as “deep” in the shoulder and occurring with overhead activities.
-
Patient may have anterior or posterior joint line tenderness.
-
Active compression test:
-
Position the affected arm as for the cross-body adduction test.
-
With the elbow extended, and the humerus internally rotated (thumb down), test resisted humeral elevation.
-
Positive test: Pain is elicited when in
internal rotation but relieved when the test is repeated in external
rotation (thumb up). -
Pain localized deep in the shoulder is indicative of biceps or labral abnormality.
-
Pain at the top of the shoulder indicates AC abnormality.
-
Pain elsewhere is equivocal.
-
-
-
Glenohumeral joint arthritis:
-
Start-up pain on initiation of activity
-
Palpable joint-line tenderness
-
Decreased active and passive ROM
-
Active and passive ROM are equal.
-
Pain at the extremes of motion in all planes
-
Glenohumeral crepitus with motion
-
-
Adhesive capsulitis:
-
Palpable joint line tenderness
-
Severely decreased ROM
-
Active and passive ROM are equal.
-
Pain with motion in all planes
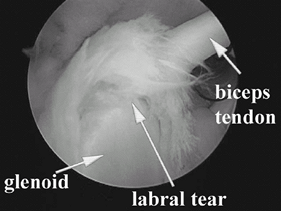 Fig. 3. Arthroscopic image of a SLAP tear.
Fig. 3. Arthroscopic image of a SLAP tear.
-
References
1. Curl LA, Warren RF. Glenohumeral joint stability. Selective cutting studies on the static capsular restraints. Clin Orthop Relat Res 1996;330:54–65.
2. Tennent
TD, Beach WR, Meyers JF. A review of the special tests associated with
shoulder examination. Part I: the rotator cuff tests. Am J Sports Med 2003;31:154–160.
TD, Beach WR, Meyers JF. A review of the special tests associated with
shoulder examination. Part I: the rotator cuff tests. Am J Sports Med 2003;31:154–160.
3. Tennent
TD, Beach WR, Meyers JF. A review of the special tests associated with
shoulder examination. Part II: laxity, instability, and superior labral
anterior and posterior (SLAP) lesions. Am J Sports Med 2003;31:301–307.
TD, Beach WR, Meyers JF. A review of the special tests associated with
shoulder examination. Part II: laxity, instability, and superior labral
anterior and posterior (SLAP) lesions. Am J Sports Med 2003;31:301–307.
4. Chronopoulos E, Kim TK, Park HB, et al. Diagnostic value of physical tests for isolated chronic AC lesions. Am J Sports Med 2004;32:655–661.
Additional Reading
Hoppenfeld S. Physical examination of the shoulder. In: Physical Examination of the Spine & Extremities. Norwalk, CT: Appleton & Lange, 1976:1–34.
Hoppenfeld S, deBoer P. The shoulder. In: Surgical Exposures in Orthopaedics: The Anatomical Approach, 3rd ed. Philadelphia: Lippincott, Williams & Wilkins, 2003:1–66.
FAQ
Q: What are the most common causes of atraumatic shoulder pain?
A: Rotator cuff disease, AC joint arthritis, cervical radiculopathy.
Q: What is the difference between a shoulder separation and a shoulder dislocation?
A: A shoulder separation is a dislocation of the AC joint. A shoulder dislocation is a dislocation of the glenohumeral joint.