
Editors: Frassica, Frank J.; Sponseller, Paul D.; Wilckens, John H.
Title: 5-Minute Orthopaedic Consult, 2nd Edition
Copyright ©2007 Lippincott Williams & Wilkins
> Table of Contents > Knee Injection
Knee Injection
Timothy S. Johnson MD
Description
-
Knee aspiration commonly is used for diagnostic purposes for effusions of unclear cause.
-
Injections are used most commonly to treat arthritis.
-
Indications
-
Effusion
-
Hemarthrosis
-
Infection/septic joint
-
Synovitis/arthritis
-
-
Equipment
-
18-gauge needle
-
20–60-mL syringes
-
Sterile gloves
-
Sterile antiseptic solution
-
-
Aspiration technique (Fig. 1):
-
The superolateral approach is the most reliable for aspiration (1).
-
Position the patient supine on the examination table with the knee fully extended or with a pillow under the knee.
-
Perform a wide sterile preparation of the knee.
-
Identify the aspiration site ~1 finger
breadth proximal to the superior pole of the patella and 1 finger
breadth lateral to the lateral border of the patella. -
Advance a needle through the skin,
subcutaneous tissue, and lateral retinaculum into the suprapatellar
pouch between the anterior femur and the quadriceps tendon from lateral
to medial.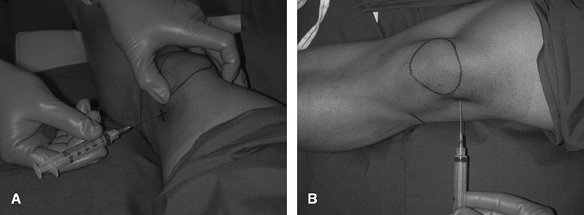 Fig. 1. Knee injection. A: Lateral view. B: Superior view.
Fig. 1. Knee injection. A: Lateral view. B: Superior view. -
Aspirate the entire fluid collection.
-
When the syringe is full, clamp the hub of the needle with a sterile clamp.
-
Hold the hub and unscrew the syringe from the needle without removing the needle from the joint.
-
Apply a new syringe to the needle hub and continue aspirating.
-
Repeat these steps as many times as necessary to aspirate the effusion completely.
-
-
Remove the needle and apply a bandage.
-
Store the fluid for laboratory analysis (see “Arthrocentesis” chapter)
-
-
Pearls
-
A wide sterile skin preparation allows for manipulation of the knee and patella during aspiration.
-
Milking the effusion up into the suprapatellar pouch allows for a more complete aspiration of fluid.
-
Synovium can easily clog the needle tip
during aspiration; use a large-bore needle (18-gauge or higher) to
minimize this problem. -
Injecting the skin with lidocaine at the injection/aspiration site is an option for patients concerned about pain.
-
It may allow the patient to tolerate the procedure better.
-
However, it does require an additional needle stick.
-
Alternatively, ethyl chloride sprayed on the skin immediately before the aspiration has a similar effect.
-
-
Never aspirate or inject through cellulitic skin.
-
-
Therapeutic injection:
-
Injection of corticosteroid:
-
Commonly performed after aspiration of synovial fluid that is not infected
-
The superolateral approach is the most reliable (1).
-
-
If an aspiration was performed:
-
Do not remove the needle from the joint.
-
Simply exchange the aspiration syringe
with the syringe filled with the injectable and inject the medication
without changing the needle’s location within the joint.
-
-
If an aspiration was not performed:
-
Identify the landmarks and insertion location as described for the superolateral approach into the suprapatellar pouch.
-
Advance the needle into the pouch.
-
Aspirate a small amount of synovial fluid to confirm intra-articular placement.
-
Once confirmed, inject the medication into the joint.
-
-
Remove the needle and apply a bandage.
-
P.217
Medication
-
Lidocaine:
-
Can be helpful in controlling pain caused by the injection.
-
Also can facilitate diagnostic procedures.
-
Painful knees are examined more easily after injection because of lidocaine’s numbing effect.
-
This effect is particularly helpful in determining the cause of a traumatic knee effusion.
-
Bupivicaine also may be used for a longer numbing effect.
-
On the day of injection, limit activity on the affected knee to activities of daily living.
-
-
-
Corticosteroid:
-
Can be useful for controlling pain and inflammation from noninfectious arthritis
-
Contraindicated if a septic knee has not been ruled out
-
A typical dose for the knee is 1 mL of kenalog (40 mg/mL), usually injected with 4 mL of 1% lidocaine.
-
Steroid medication usually takes 2–3 days to have an effect.
-
Manage the patient’s expectations by discussing this delayed pain relief at the time of the injection.
-
-
-
Hyaluronates (2) are indicated for treatment of mild osteoarthritis.
References
1. Wind WM, Jr, Smolinski RJ. Reliability of common knee injection sites with low-volume injections. J Arthroplasty 2004;19:858–861.
2. Miller EH. Viscosupplementation: therapeutic mechanisms and clinical potential in osteoarthritis of the knee. J Am Acad Orthop Surg 2001;9: 146–147.
Additional Reading
Cole BJ, Schumacher HR, Jr. Injectable corticosteroids in modern practice. J Am Acad Orthop Surg 2005; 13:37–46.
FAQ
Q: Which approach is least reliable in successfully injecting therapeutic agents into the knee joint?
A: The lateral joint line approach.
Q: Viscosupplementation therapy of the knee is indicated for which type of arthritis?
A: Osteoarthritis.