
Editors: Frassica, Frank J.; Sponseller, Paul D.; Wilckens, John H.
Title: 5-Minute Orthopaedic Consult, 2nd Edition
Copyright ©2007 Lippincott Williams & Wilkins
> Table of Contents > Macrodactyly
Macrodactyly
Paul D. Sponseller MD
Description
-
Macrodactyly is overgrowth of 1 or
several adjacent digits or rays of a hand or foot that produces the
appearance of localized gigantism (Fig. 1). -
Virtually all cases are present at birth, although some cases worsen disproportionately.
-
Growth of the enlarged digits ceases when the patient reaches skeletal maturity.
-
-
Classification (1):
-
Static: Enlargement remains proportionate to other digits
-
Dynamic: Enlargement increases with time, even by proportion
-
-
Synonym: Localized gigantism
Epidemiology
-
Upper extremity more commonly affected than lower extremity
-
No gender-specific predilection for increased frequency
Incidence
-
<1 per 10,000 (2,3)
-
Most cases (95%) are unilateral (3,4).
Risk Factors
-
Most cases are isolated (idiopathic).
-
Also may occur in:
-
NF
-
Proteus syndrome
-
Klippel-Trenaunay syndrome
-
Genetics
-
Isolated macrodactyly is not a heritable condition.
-
Only if it is associated with NF does a familial tendency exist.
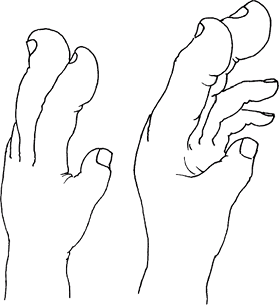 Fig. 1. Macrodactyly is generalized enlargement of 1 or 2 digits of the hand or foot.
Fig. 1. Macrodactyly is generalized enlargement of 1 or 2 digits of the hand or foot.
Etiology
-
In idiopathic macrodactyly, the cause is
unknown; it may be secondary to a localized disturbance of growth
factors in the ectodermal ridge. -
Other cases of macrodactyly occur in patients with NF, Proteus syndrome, lymphedema, and hemangiomas.
Associated Conditions
-
Proteus syndrome (multiple hamartomatous abnormalities)
-
NF
-
Klippel-Trenaunay syndrome
Signs and Symptoms
-
Generalized overgrowth of all tissues in the affected digits occurs.
-
Enlargement is greater distally than proximally.
-
The nail is especially enlarged.
-
Tissues on the plantar or palmar surface
of the digit are more greatly enlarged than those on the dorsal side,
thus causing the digit to become hyperextended (dorsiflexed). -
The 2nd ray is affected most commonly, followed by the 3rd, 1st, and 4th.
-
Syndactyly may coexist (Fig. 2).
 Fig.
Fig.
2. Macrodactyly of the foot in a 2-year-old. Note the central
involvement, syndactyly, involvement is greatest plantarly and
distally, and contralateral normal foot. A: Dorsal view. -
If 2 digits are involved, they grow away from each other.
-
In some cases, the enlargement becomes proportionately greater with time (dynamic type).
-
Main clinical symptoms are related to overgrowth, such as clumsiness in the hand or difficulty with shoe wear.
-
Pain may occasionally develop in adulthood because degeneration of the involved joints is premature.
Physical Exam
-
Diagnosis is made purely by physical examination.
-
Inspect the patient’s hands and feet for hemangiomas and other signs of Proteus syndrome and NF.
-
Compare limb lengths; they are rarely uneven in idiopathic macrodactyly.
-
Check the motion of the affected digits.
-
Compare the widths and lengths of the 2 hands or feet.
-
Progression of growth of the hand or foot
may be tracked clinically by making tracings or prints of both hands or
feet over time, so length and width may be measured and compared.
Tests
Lab
Genetic testing is available for Proteus syndrome and NF, if they are suspected.
Imaging
-
Plain films should be obtained to help assess and document the extent of overgrowth and the segments involved.
-
Soft-tissue enlargement also may be quantified from these films.
-
The extent of skeletal maturity also may be judged; it often is advanced in the enlarged rays.
-
-
MRI is rarely necessary.
Pathological Findings
-
All tissue types are overgrown in the affected digit.
-
Fibrofatty proliferation accounts for the greatest bulk.
-
Vessel, bone, subcutaneous tissue, and dermis are enlarged, and the changes are greatest distally.
-
Pathologic changes are greatest in the digital nerves.
Differential Diagnosis
-
Hemihypertrophy, in which all digits in a hand or foot are uniformly overgrown
-
Acrodactyly, in which overgrowth of all digits is greatest distally
-
Growth hormone overabundance (hypersecretion), acromegaly
P.241
General Measures
-
Serial follow-up:
-
The pattern of growth may be determined by serial follow-up.
-
In this way, the static and the
progressive types may be distinguished, and the appropriate treatment
may be chosen: observation, shoe modification, or surgery.
-
-
Measurements of length and width
-
Surgery
Medication
No drugs are known to help this condition.
Surgery
-
Surgery may involve resection of the most enlarged ray, if the width of the hand or foot is greatly increased.
-
Surgery is the fastest way to make an important difference.
-
-
Phalangectomy may make the length more even if the width is not a problem.
-
It also may be performed in addition to ray resection to address excessive length of adjacent digits.
-
-
Epiphysiodesis (closure of the growth plates) is another way of evening length.
-
The correction occurs more gradually with time, and it may not completely correct the length inequality.
-
-
Debulking of fat may improve the appearance, especially of the plantar fat hypertrophy.
-
To avoid tissue ischemia, surgeon discretion on staging these multiple procedures is advised.
Prognosis
-
Most patients are made substantially better by judicious surgery.
-
At the same time, it is important to realize that the parts will not be completely normal.
Complications
-
Stiffness and aching in the joints of the enlarged digits often develop in adulthood.
-
Persistent enlargement, especially in the width of the involved digits, is the norm.
-
Circulatory disturbance may occur if both sides of an involved digit undergo surgery concurrently.
Patient Monitoring
-
Serial follow-up appointments every 6–12 months are needed to develop and monitor a treatment plan.
-
To keep records, tracings or radiographs should be made at each visit.
-
Follow-up should be continued up to, and past, maturity.
References
1. Dennyson WG, Bear JN, Bhoola KD. Macrodactyly in the foot. J Bone Joint Surg 1977;59B:355–359.
2. Akinci M, Ay S, Ercetin O. Surgical treatment of macrodactyly in older children and adults. J Hand Surg 2004;29A:1010–1019.
3. Barsky AJ. Macrodactyly. J Bone Joint Surg 1967; 49A:1255–1266.
4. Chang CH, Kumar SJ, Riddle EC, et al. Macrodactyly of the foot. J Bone Joint Surg 2002; 84A:1189–1194.
Codes
ICD9-CM
-
755.57 Macrodactyly of fingers or thumb
-
755.65 Macrodactyly of toes
Patient Teaching
-
Show radiographs to help explain the nature of the condition.
-
Advise that macrodactyly often requires several surgical procedures to achieve an optimal result.
-
Emphasize the benefits of ray resection, if appropriate.
FAQ
Q: When will the affected digits stop their overgrowth?
A: Only with maturity will the affected digits stop their overgrowth.
Q: What is the cause of macrodactyly?
A: Currently, it is unknown.