
Editors: Frassica, Frank J.; Sponseller, Paul D.; Wilckens, John H.
Title: 5-Minute Orthopaedic Consult, 2nd Edition
Copyright ©2007 Lippincott Williams & Wilkins
> Table of Contents > Hip Dislocation, Traumatic
Hip Dislocation, Traumatic
Gregory Gebauer MD, MS
Description
-
Dislocations and fracture-dislocations of the hip are orthopaedic emergencies.
-
Serious, high-energy injuries in which the femoral head becomes completely dislodged from the acetabulum
-
-
A thorough examination must be performed to assess for other possible injuries.
-
Up to 50% of patients suffer other fractures at the time of injury (1).
-
Associated acetabular or femoral head or neck fractures are common.
-
-
Classification is based on the direction
of dislocation (anterior versus posterior) and associated fractures in
the femoral head or femoral neck (Fig. 1-1).
General Prevention
Seat belts should be used in conjunction with air bags.
Epidemiology
-
Most common in young adults (1)
-
More males than females are affected (1).
Incidence
-
Anterior dislocation: 10–15% (1)
-
Posterior dislocation: 85–90% (1)
Risk Factors
-
Motor vehicle accidents
-
Falls from substantial heights
Etiology
-
70–90% of traumatic hip dislocations are caused by motor vehicle accidents (2).
-
As the car decelerates, the flexed knee strikes the dashboard, forcing the femoral head out posteriorly (2).
-
-
Other mechanisms include automobile
versus pedestrian accidents, falls from heights, industrial injuries,
and sporting accidents.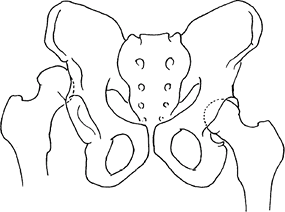 Fig.
Fig.
1. In an acute hip dislocation, the femoral head usually is displaced
posteriorly and superiorly. The acetabulum should be inspected for
fractures.
Associated Conditions
-
Because hip dislocations usually are secondary to high-energy trauma, other severe injuries are common, including:
-
Neurologic injuries: Sciatic nerve palsy and herniated discs
-
Sciatic nerve injury occurs in 10–20% of posterior dislocations (3).
-
Sciatic nerve injury appears to be related to the length of time that the hip is dislocated (3).
-
-
Musculoskeletal injuries:
-
Femoral head, neck, and acetabular fractures
-
Common: Ipsilateral knee and foot injuries
-
-
Intra-abdominal or chest injuries
-
Signs and Symptoms
-
Severe pain over the hip or numbness along the posterior thigh
-
Altered resting lower extremity position:
-
In posterior dislocation, the hip is fixed in a position of flexion, internal rotation, and adduction.
-
In anterior dislocation, the hip is in marked external rotation with mild flexion and abduction.
-
-
Shortening of the extremity
-
Many patients suffering traumatic hip
dislocations are obtunded or unconscious on arrival at the emergency
department and, therefore, cannot assist the physician in the initial
evaluation.
Physical Exam
-
Examination must include a full trauma survey, because concomitant injuries are common.
-
Motor and sensory nerve function as well
as the presence or absence of pulses should be documented before and
after reduction of the dislocation. -
In particular, sciatic nerve function should be assessed.
Tests
Lab
A standard series of lab tests for a trauma workup should be obtained.
Imaging
-
All patients with traumatic hip
dislocations should have routine trauma radiographs, including cervical
spine, chest, and AP pelvic films.-
Plain films of painful extremities or
other pelvic views (internal or external oblique-Judet views) should be
obtained if associated fractures are suspected. -
A cross-table lateral view of the hip will determine if the dislocation is anterior or posterior.
-
Judet views may help identify any acetabular fracture.
-
In a posterior dislocation, the femoral head appears smaller radiographically than on the contralateral, uninjured side.
-
In an anterior dislocation, the femoral head appears slightly larger than in the uninjured hip.
-
Careful evaluation of the femoral neck
must rule out the presence of a femoral neck fracture before any
manipulative reduction is undertaken.-
The acetabulum should be inspected
carefully to ascertain the presence or absence of intra-articular
osteochondral fragments and asymmetry of the joint space.
-
-
-
CT scans:
-
Should be obtained routinely after successful closed reductions or before surgery, if open reduction is planned.
-
Valuable in showing the presence of small
intra-articular fragments and in assessing the congruence of the
femoral head and acetabulum (4)
-
-
The role of MRI in posttraumatic evaluation of the hip has not yet been established, and this technique is not currently used.
Differential Diagnosis
-
Femoral neck and head fracture
-
Acetabular and pelvic fractures
Initial Stabilization
-
Assess the patient for concomitant injuries, which are common.
-
Determine whether closed reduction can be done.
-
Sedation is required for reduction.
-
Document the affected limb’s neurovascular status before and after reduction.
General Measures
-
Emergent orthopaedic consultation should
be obtained because urgent reduction of the dislocated hip is necessary
to prevent long-term complications. -
It is important to assess patients fully for concomitant injuries secondary to high-energy trauma.
-
The management of a patient with a hip dislocation is divided into 2 phases:
-
Initial phase: Identify and reduce the dislocation:
-
Perform reduction quickly to reduce the risk of femoral head osteonecrosis.
-
If possible, closed reduction in the
emergency department or operating room with the patient under general
anesthesia and with complete muscle paralysis -
If general anesthesia is not immediately feasible, attempt reduction with the patient under intravenous sedation.
-
Regardless of the direction of the dislocation, attempt reduction with inline traction with the patient lying supine (5).
-
During the reduction, assess stability.
-
Obtain confirmatory radiographs after reduction.
-
After successful closed reduction and
completion of the stability examination, place the patient in traction
to await CT evaluation.-
If the hip has been shown to be stable, simple traction using a Buck traction boot or skin traction is sufficient.
-
If the hip is unstable, it is preferable to use skeletal traction with a tibial pin.
-
P.185 -
-
Secondary phase: Plan and perform definitive care:
-
Once the femoral head has been reduced,
urgency is diminished, and an appropriate diagnostic workup, including
CT analysis, can be completed. -
Surgical intervention, if indicated, can
be undertaken after the patient has become hemodynamically stable and
safe for operative management. -
Indications for surgical treatment
include inability to obtain adequate closed reduction, nonconcentric
reduction, ipsilateral femur fracture, or presence of an associated
acetabular fracture requiring surgical treatment (6).
-
-
Activity
-
Weightbearing status depends on the stability of the hip and the presence of any associated fractures.
-
Early active ROM is ideal.
-
Patients with postreduction stable hips should be mobilized and allowed to bear weight (7).
Special Therapy
Physical Therapy
Often required for gait training with protected weightbearing and ROM
Medication
First Line
Narcotic analgesics
Surgery
-
If closed reduction cannot be achieved, then open reduction is indicated.
-
The standard posterior approach, or a
lateral decubitus position, is used with or without a fracture
(traction) table, depending on the surgeon’s preference.
Prognosis
-
Posterior dislocations:
-
70–80% of simple posterior hip dislocations (without associated fractures) have good or excellent outcomes (1).
-
When posterior dislocations are associated with femoral head fractures or acetabular fractures, the outcome is not as favorable.
-
-
Anterior dislocations:
-
Patients with anterior dislocations have
been noted to have a high incidence of femoral head injuries, and
long-term outcome is not as good as with posterior dislocations.
-
-
Long-term prognosis worsens if the time to reduction is >12 hours.
Complications
-
Posttraumatic arthritis is the most frequent long-term complication.
-
The incidence of arthritis is higher in patients with associated acetabular or femoral head fractures.
-
Secondary arthritis may develop as a result of AVN.
-
-
Osteonecrosis (AVN) occurs in 1–17% of these patients (8).
-
A risk exists for osteonecrosis of the
hip, even with prompt hip reduction, secondary to injury to the femoral
head’s blood supply. -
The risk increases when the hip remains dislocated for a period of time.
-
Threshold time is reported to be ~6–24 hours (5).
-
-
Sciatic nerve injury occurs in 8–19% of
patients and is caused by stretching of the nerve from a posteriorly
dislocated femoral head or from a displaced fracture fragment.-
The peroneal component of the nerve is affected most commonly.
-
Electromyography and nerve conduction
studies are indicated at 3–4 weeks for baseline information,
documentation of precise level, and prognostic guidance. -
Prognosis is unpredictable, with 40–50% reporting full recovery (3).
-
-
Recurrent dislocation is rare (<2%) (1).
-
Heterotopic ossification is a rare complication of hip dislocation.
Patient Monitoring
-
In the 1st year, serial hip radiographs every 3–4 months
-
MRI will diagnose osteonecrosis.
References
1. Sahin V, Karakas ES, Aksu S, et al. Traumatic dislocation and fracture-dislocation of the hip: a long-term follow-up study. J Trauma 2003;54: 520–529.
2. Monma
H, Sugita T. Is the mechanism of traumatic posterior dislocation of the
hip a brake pedal injury rather than a dashboard injury? Injury 2001;32: 221–222.
H, Sugita T. Is the mechanism of traumatic posterior dislocation of the
hip a brake pedal injury rather than a dashboard injury? Injury 2001;32: 221–222.
3. Hillyard RF, Fox J. Sciatic nerve injuries associated with traumatic posterior hip dislocations. Am J Emerg Med 2003;21:545–548.
4. Brooks RA, Ribbans WJ. Diagnosis and imaging studies of traumatic hip dislocations in the adult. Clin Orthop Relat Res 2000;377:15–23.
5. Yang EC, Cornwall R. Initial treatment of traumatic hip dislocations in the adult. Clin Orthop Relat Res 2000;377:24–31.
6. Alonso JE, Volgas DA, Giordano V, et al. A review of the treatment of hip dislocations associated with acetabular fractures. Clin Orthop Relat Res 2000;377:32–43.
7. Schlickewei W, Elsasser B, Mullaji AB, et al. Hip dislocation without fracture: traction or mobilization after reduction? Injury 1993;24: 27–31.
8. Rodriguez-Merchan EC. Osteonecrosis of the femoral head after traumatic hip dislocation in the adult. Clin Orthop Relat Res 2000;377:68–77.
Codes
ICD9-CM
835.00 Hip dislocation
Patient Teaching
Activity
Patients should be counseled on safe driving practices, including the use of seat belts and airbags.
Prevention
The use of seat belts and airbags may help prevent hip dislocations.
FAQ
Q: Will I be at risk for dislocation in the future?
A: No. The risk of recurrent dislocation is low (<2%).
Q: What problems may I have in the future?
A:
The most common long-term problems after hip dislocation are
osteonecrosis and traumatic arthritis, both of which may lead to
chronic hip pain. These problems may ultimately lead to total hip
replacement.
The most common long-term problems after hip dislocation are
osteonecrosis and traumatic arthritis, both of which may lead to
chronic hip pain. These problems may ultimately lead to total hip
replacement.
Q: My sciatic nerve was injured during the dislocation; can I expect to get function back?
A: 40–50% of patients report full recovery, but recovery can take months to a year.