
Authors: Koval, Kenneth J.; Zuckerman, Joseph D.
Title: Handbook of Fractures, 3rd Edition
Copyright ©2006 Lippincott Williams & Wilkins
> Table of Contents > I – General Considerations > 4 – Gunshot Wounds
4
Gunshot Wounds
BALLISTICS
-
Low-velocity (<2,000 ft/sec): This includes all handguns.
-
High-velocity (>2,000 ft/sec): This includes all military rifles and most hunting rifles.
-
Shotgun wounding potential is dependent on:
-
Chote (shot pattern)
-
Load (size of the individual pellet)
-
Distance from the target
-
ENERGY
-
The kinetic energy (KE) of any moving object is directly proportional to its mass (m) and the square of its velocity (v2), and is defined by the equation: KE = 1/2 (mv2).
-
The energy delivered by a missile to a target is dependent on:
-
The energy of the missile on impact (striking energy).
-
The energy of the missile on exiting the tissue (exit energy).
-
The behavior of the missile while traversing the target: tumbling, deformation, fragmentation.
-
TISSUE PARAMETERS
-
The wounding potential of a bullet
depends on the missile parameters, including caliber, mass, velocity,
range, composition, and design, as well as those of the target tissue. -
The degree of injury created by the
missile is generally dependent on the specific gravity of the traversed
tissue: higher specific gravity = greater tissue damage. -
A missile projectile achieves a high
kinetic energy because of its relatively high velocity. The impact area
is relatively small, resulting in a small area of entry with a
momentary vacuum created by the soft tissue shock wave. This can draw
adjacent material, such as clothing and skin, into the wound. -
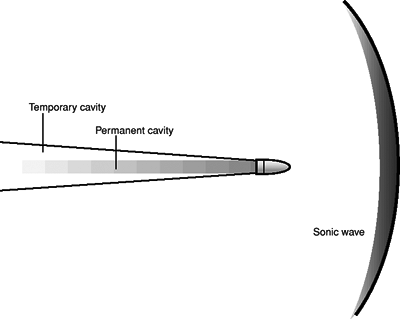
The direct passage of the missile through
the target tissue becomes the permanent cavity. The permanent cavity is
small, and its tissues are subjected to crush (Fig. 4.1). -
The temporary cavity (cone of cavitation)
is the result of a stretch-type injury from the dissipation of imparted
kinetic energy (i.e., shock wave). It is large, and its size
distinguishes high-energy from low-energy wounds. -
Gases are compressible, whereas liquids
are not; therefore, penetrating missile injuries to the chest may
produce destructive patterns only along the direct path of impact as a
result of air-filled structures, whereas similar injuries to
fluid-filled structures (e.g., liver, muscle) produce considerable
displacement of the incompressible liquid with shock-wave dissipation,
resulting in significant momentary cavities. This may lead to regions
of destruction apparently distant to the immediate path of the missile
with resultant soft tissue compromise.
P.31
CLINICAL EVALUATION
 |
|
Figure
4.1. The two areas of tissue injury: the permanent cavity and the temporary cavity. The permanent cavity is caused by localized areas of cell necrosis proportional to the size of the projectile as it travels through. Temporary cavitization causes a transient lateral displacement of tissue. The shock wave, although measurable, has not been found to cause injury in tissue. (From Bucholz RW, Heckman JD, Court-Brown C, et al., eds. Rockwood and Green’s Fractures in Adults, 6th ed. Philadelphia: Lippincott Williams & Wilkins, 2006.)
|
-
Following initial trauma survey and management (see Chapter 2),
specific evaluation of the gunshot injury will vary based on the
location of injury and patient presentation. Careful neurovascular
examination must be undertaken to rule out the possibility of
disruption to vascular or neural elements. -
Attention must also be paid to possible
injuries sustained after the missile impact, such as those that may
occur following a fall from a height.
RADIOGRAPHIC EVALUATION
-
Standard AP and lateral radiographs of the injured sites should be obtained.
-
Specific attention must be paid to
retained missile fragments, degree of fracture comminution, and the
presence of other foreign bodies (e.g., gravel). -
Missile fragments can often be found distant to the site of missile entry or exit.
P.32
TREATMENT OF ORTHOPAEDIC GUNSHOT INJURIES
Low-Velocity Wounds
-
Victims can usually be treated as outpatients.
-
Steps in treatment include:
-
Administration of antibiotics (first-generation cephalosporin), tetanus toxoid, and antitoxin.
-
Irrigation and debridement of the entrance and exit skin edges.
-
Indications for operative debridement:
-
Retention in the subarachnoid space
-
Articular involvement (intraarticular bone or missile fragments)
-
Vascular disruption
-
Gross contamination
-
Missile superficial on the palm or sole
-
Massive hematoma
-
Severe tissue damage
-
Compartment syndrome
-
Gastrointestinal contamination
-
-
Fracture treatment: Generally treat this injury as a closed fracture.
-
High-Velocity and Shotgun Wounds
-
These should be treated as high-energy injuries with significant soft tissue damage.
-
Steps in treatment include:
-
Administration of antibiotics (first-generation cephalosporin), tetanus toxoid, and antitoxin.
-
Extensive and often multiple operative debridements.
-
Fracture stabilization.
-
Delayed wound closure with possible skin grafts or flaps for extensive soft tissue loss.
-
Important: Gunshot wounds
that pass through the abdomen and exit through the soft tissues with
bowel contamination deserve special attention. These require
debridement of the intraabdominal and extraabdominal missile paths,
along with administration of broad spectrum antibiotics covering
gram-negative and anaerobic pathogens.
that pass through the abdomen and exit through the soft tissues with
bowel contamination deserve special attention. These require
debridement of the intraabdominal and extraabdominal missile paths,
along with administration of broad spectrum antibiotics covering
gram-negative and anaerobic pathogens.
COMPLICATIONS
-
Retained missile fragments: These are
generally tolerated well by the patient and do not warrant a specific
indication for surgery or a hunt for fragments at the time of surgery
unless they are causing symptoms (pain, loss of function), are
superficial in location especially on the palms or soles, are involved
in an infected wound, or are intraarticular in location. Occasionally,
the patient will develop a draining sinus through which fragments will
be expressed. -
Infection: Studies have demonstrated that
gunshot injuries are not necessarily “sterile injuries” as was once
thought. This is secondary to skin flora, clothing, and other foreign
bodies that are drawn into the wound at the time of injury. In
addition,
P.33
missiles
that pass through the mouth or abdomen are seeded with pathogens that
are then dispersed along the missile path. Meticulous debridement and
copious irrigation will minimize the possibility of wound infection,
abscess formation, and osteomyelitis. -
Neurovascular disruption: The incidence
of damage to neurovascular structures is much higher in high-velocity
injuries (military weapons, hunting rifles), owing to the energy
dissipation through tissues created by the shock wave. Temporary
cavitation may produce traction or avulsion injuries to structures
remote from the immediate path of the missile. These may result in
injuries ranging from neuropraxia and thrombosis to frank disruption of
neural and vascular structures. -
Lead poisoning: Synovial or cerebrospinal
fluid is caustic to lead components of bullet missiles, resulting in
lead breakdown products that may produce severe synovitis and low-grade
lead poisoning. Intraarticular or subarachnoid retention of missiles or
missile fragments is thus an indication for exploration and removal.