
Editors: Swiontkowski, Marc F.; Stovitz, Steven D.
Title: Manual of Orthopaedics, 6th Edition
Copyright ©2001 Lippincott Williams & Wilkins
> Table of Contents > 6 – Common Types of Emergency Splints
6
Common Types of Emergency Splints
I. Emergency Splinting of The Spine
-
Patients with spinal injuries should be splinted with a backboard before they are moved, as shown in Fig. 6-1.
Immobilize patients with suspected cervical spine injuries by placing
sandbags, rolled towels, or rolled blankets on each side of the head.
Then put a cravat through or around the backboard and over the
forehead. In this way, the patient’s head, neck, and backboard can be moved as one unit.
Commercial foam as well as plastic neck collars are available in
different sizes and are carried by emergency medical technician (EMT)
units. One can also make an adequate neck collar by placing foam or
felt of the appropriate width, thickness, and length inside a tubular
stockinet and then fastening the stockinet about the patient’s neck.
This method is particularly useful for immobilizing the neck of injured
children where correct sizing is critical so as to immobilize the neck
without extension or flexion. The only emergency indication for moving
the neck of an individual with a suspected injured cervical spine is to
improve an inadequate airway by aligning the neck with the torso and
opening the airway with a jaw thrust. -
Be aware of possible neurogenic shock, which is treated by elevating the lower end of the backboard to improve venous return in the reverse Trendelenburg position.
-
If complete evaluation identifies a cervical spine fracture, then the patient is usually placed in traction
or hard collar immobilization. The direction of traction depends on the
injury. If there is no dislocation, then a neutral or slightly extended
position is preferred (see Chap. 9).
II. Upper Extremity Splinting
-
Remember to remove rings from an involved hand!
Swelling can make them impossible to remove without cutting them off
and they obscure x-rays. Petroleum jelly can be useful for ring removal. -
Figure-of-8 splint
-
The principal use is for clavicular fractures (see Chap. 13).
-
Application.
The factory-made figure-of-8 clavicular strap is recommended because it
is a webbed fabric and does not stretch. If a properly fitting
factory-made strap is not available for children younger than 10 years
old, make a figure-of-8 strap with a tubular stockinet filled with felt
or cotton padding, as shown in Fig. 6-2.
These should be used only if they make the patient more comfortable. A
sling is generally more effective in this regard. Generally, the
figure-of-8 splint does not improve fracture reduction. -
Precautions
-
Prevent skin maceration with a powdered pad in the axilla.
-
In the adult, restrict the use of the sling and encourage glenohumeral motion after 2 weeks to prevent shoulder stiffness.
-
Do not tighten the figure-of-8 strap to the point that the axillary artery or brachial plexus is compressed.
-
-
-
Velpeau and sling-and-swathe bandages
-
These bandages are used for shoulder dislocations, proximal humerus fractures, and humeral fractures.
-
One application of Velpeau bandage using bias-cut stockinet is seen in Fig. 6-3. The common application of the typical sling-and-swathe bandage is shown in Fig. 6-4.
P.94
Either type of bandage can be covered with a light layer of fiberglass or plaster to prevent unraveling of the material. Figure 6-1. A backboard may be used in an emergency to transport a patient with a spinal injury.
Figure 6-1. A backboard may be used in an emergency to transport a patient with a spinal injury. -
Precautions
-
Prevent skin maceration with a powdered pad in the axilla and between the arm and chest.
-
Prevent wrist and finger stiffness with active exercise.
![]() Figure 6-2.
Figure 6-2.
Typical figure-of-8 splint made for a child younger than 10 years old
with a fractured clavicle. In adults, use a factory-made splint when
possible.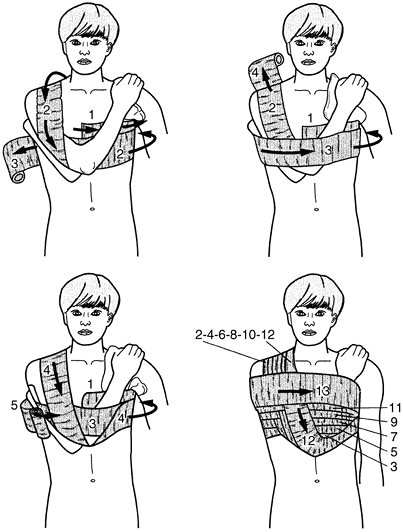 Figure 6-3. Method for applying Velpeau bandage.
Figure 6-3. Method for applying Velpeau bandage.
-
-
A number of commercial shoulder immobilizers
are available. Although they provide less secure immobilization than
the Velpeau and sling-and-swathe bandages, these ready-made items have
proved satisfactory. Commercial straps for acromioclavicular (AC)
separations are also available; they have straps which go over the
distal one third of the clavicle and lift up on the elbow in order to
reduce the AC separation.
P.95 -
-
Use air splints
in emergency situations for the distal extremity. The air splint is
closed over the extremity by its zipper and inflated by flowing air
into the mouth tube. High pressure from mechanical pumps can produce
circulatory embarrassment and should not be used. Skin maceration
occurs if air splints are used for any extended period. Cardboard or
magazines can be used with tape of any sort to achieve temporary
immobilization.

III. Lower Extremity Splinting
-
Thomas splint
-
Use for femoral shaft fractures and, occasionally, knee injuries.
The following description is for the emergency situation. The Thomas
splint may also be used as fixed skeletal traction, as described in Chap. 9, VII.F.3.![]() Figure 6-4. Slng-and-swathe bandage, covered by a single layer of plaster to help prevent unraveling of the material.
Figure 6-4. Slng-and-swathe bandage, covered by a single layer of plaster to help prevent unraveling of the material. -
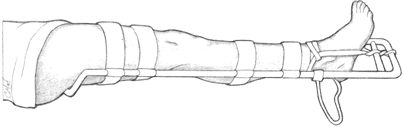
The ideal Thomas splint application
uses a full ring splint that measures 2 in. greater than the
circumference of the proximal thigh. If a full ring splint is not
available, use a half ring splint with a strap placed anteriorly. The
ring engages the ischial tuberosity for countertraction, and traction
is applied to the end of the splint with an ankle hitch, as shown in Fig. 6-5.
A Spanish windlass is made by taping several tongue blades together.
These twist the material used to secure the ankle hitch to the end of
the splint, producing a traction force. The half ring splint still
engages the ischial tuberosity, and the strap buckles down across the
anterior thigh. Towels or a tubular stockinet placed on the Thomas
splint with safety pins support the leg, as shown in Fig. 6-6. -
Hare splints and Roller splints
are also commercially available. They differ from the Thomas splint
only by the foot attachments and leg supports. They are in widespread
use by emergency medical technicians. -
Most precautions relate to complications of fixed skeletal traction and are discussed in Chap. 9, VII.
Do not leave the temporary splint on for more than 2 hours, whenever
possible, because the ankle hitch places significant pressure on the
skin and may produce necrosis.
P.96 -
-
Jones compression splint
-
Use in acute knee trauma (patellar, knee, and some tibial fractures) and acute ankle injuries.
-
Apply by wrapping the injured leg from
the toes to the groin in rolled cotton. Next, add a single layer of
elastic bandage. Apply 5- × 30-inch plaster splints posteriorly,
medially, and laterally to keep the ankle in a neutral position. Medial
and lateral splints support the knee in the desired degree of flexion.
Do not overlap the splints, or a circumferential plaster will be
created about the extremity. The splints are then overwrapped with
bias-cut stockinet in a herringbone fashion. -
Precautions
-
Do not apply wraps too tightly.
-
Do not make upper wraps tighter than lower wraps or venous return will be impeded, causing swelling and circulatory problems.
-
-
Although they provide less satisfactory compression, commercial knee immobilizers are acceptable in most cases.
-
-
Short-leg or modified Jones compression splint
-
Use in acute ankle and foot trauma such as ankle sprains, calcaneal fractures, and other foot injuries.
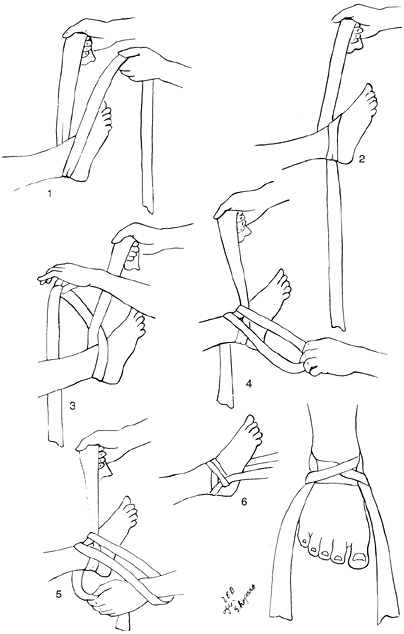 Figure 6-5.
Figure 6-5.
A Collins hitch is a means of applying traction from the ankle to the
end of the Thomas splint, but it is used only in emergency situations.![]() Figure 6-6. A Thomas splint may be used at the scene of the accident for a fracture of the femur.
Figure 6-6. A Thomas splint may be used at the scene of the accident for a fracture of the femur. -
The splint is applied in a fashion similar to that described for the Jones splint except that it does not extend above the tibial tubercle.
-
Precautions are the same as those for the Jones compression splint.
P.97P.98 -
-
Commercial leg and ankle braces
-
Short leg walkers
constructed of a rigid foot piece and double uprights and secured with
Velcro fasteners are available for conditions not requiring more rigid
cast immobilization. -
Lace-up canvas ankle supports with removable aluminum stays are also often convenient and useful for ankle sprains and instability.
-
Air splints
with inflatable medial and lateral supports have recently proven
extremely useful as supports for ankle sprains and stable fractures
that are well along in the healing process.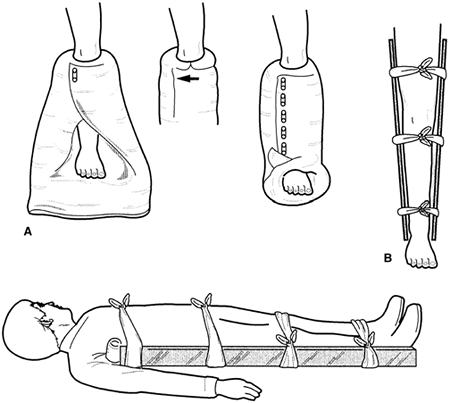 Figure 6-7. A: A pillow splint may be applied to a leg with a distal injury as a temporary measure. B: Board splints may be used for lower-extremity fractures in emergency situations.
Figure 6-7. A: A pillow splint may be applied to a leg with a distal injury as a temporary measure. B: Board splints may be used for lower-extremity fractures in emergency situations.
-
-
Other emergency splints
-
Make-do splints
may be used as a temporary measure. One may apply a pillow splint,
rigid cardboard, magazine, or a wooden splint to the upper or lower
extremity. A pillow splint for the ankle is shown in Fig. 6-7A. -
Precautions
-
Avoid circulatory embarrassment
by applying splint straps or wraps in such a way as to prevent pressure
on the skin over a bony prominence or a tourniquet effect to the
extremity. -
Splint
-
For closed fractures,
restore gross limb angulation into better alignment before the splint
is applied by using gentle traction first in the direction of the
angulation and then in the long axis of the limb. -
Restore alignment in the same manner if there is tenting of the skin over the injury.
-
For open fractures, gross limb alignment should be restored, the wound inspected and dressed with sterile technique, and a splint applied.
-
-
Cover exposed bone with a saline- or betadine-moistened sterile dressing as first aid treatment.
-
-

P.99