
Authors: Koval, Kenneth J.; Zuckerman, Joseph D.
Title: Handbook of Fractures, 3rd Edition
Copyright ©2006 Lippincott Williams & Wilkins
> Table of Contents > III – Upper Extremity Fractures and Dislocations > 11 – Clavicle Fractures
11
Clavicle Fractures
EPIDEMIOLOGY
-
Clavicle fractures account for 2.6% to 12% of all fractures and for 44% to 66% of fractures about the shoulder.
-
Middle third fractures account for 80% of
all clavicle fractures, whereas fractures of the lateral and medial
third of the clavicle account for 15% and 5%, respectively.
ANATOMY
-
The clavicle is the first bone to ossify
(fifth week of gestation) and the last ossification center (sternal
end) to fuse, at 22 to 25 years of age. -
The clavicle is S-shaped, with the medial end convex forward and the lateral end concave forward.
-
It is widest at its medial end and thins laterally.
-
The medial and lateral ends have flat expanses that are linked by a tubular middle, which has sparse medullary bone.
-
The clavicle functions as a strut,
bracing the shoulder from the trunk and allowing the shoulder to
function at optimal strength. -
The medial one-third protects the
brachial plexus, the subclavian and axillary vessels, and the superior
lung. It is strongest in axial load. -
The junction between the two
cross-sectional configurations occurs in the middle third and
constitutes a vulnerable area to fracture, especially with axial
loading. Moreover, the middle third lacks reinforcement by muscles or
ligaments distal to the subclavius insertion, resulting in additional
vulnerability. -
The distal clavicle contains the coracoclavicular ligaments.
-
The two components are the trapezoid and conoid ligaments.
-
They provide vertical stability to the acromioclavicular (AC) joint.
-
They are stronger than the AC ligaments.
-
MECHANISM OF INJURY
-
Falls onto the affected shoulder account
for most (87%) of clavicular fractures, with direct impact accounting
for only 7% and falls onto an outstretched hand accounting for 6%. -
Although rare, clavicle fractures can
occur secondary to muscle contractions during seizures or
atraumatically from pathologic mechanisms or as stress fractures.
CLINICAL EVALUATION
-
Patients usually present with splinting
of the affected extremity, with the arm adducted across the chest and
supported by the contralateral hand to unload the injured shoulder. -
A careful neurovascular examination is
necessary to assess the integrity of neural and vascular elements lying
posterior to the clavicle. -
The proximal fracture end is usually
prominent and may tent the skin. Assessment of skin integrity is
essential to rule out open fracture. -
The chest should be auscultated for
symmetric breath sounds. Tachypnea may be present as a result of pain
with inspiratory effort; this should not be confused with diminished
breath sounds, which may be present from an ipsilateral pneumothorax
caused by an apical lung injury.
P.122
ASSOCIATED INJURIES
-
Up to 9% of patients with clavicle fractures have additional fractures, most commonly rib fractures.
-
Most brachial plexus injuries are associated with proximal third clavicle fractures.
RADIOGRAPHIC EVALUATION
-
Standard anteroposterior radiographs are
generally sufficient to confirm the presence of a clavicle fracture and
the degree of fracture displacement. -
A 30-degree cephalad tilt view provides an image without the overlap of the thoracic anatomy.
-
An apical oblique view can be helpful in
diagnosing minimally displaced fractures, especially in children. This
view is taken with the involved shoulder angled 45 degrees toward the
x-ray source, which is angled 20 degrees cephalad. -
Computed tomography may be useful,
especially in proximal third fractures, to differentiate
sternoclavicular dislocation from epiphyseal injury, or distal third
fractures, to identify articular involvement.
CLASSIFICATION
Descriptive
Clavicle fractures may be classified according to
anatomic description, including location, displacement, angulation,
pattern (e.g., greenstick, oblique, transverse), and comminution.
anatomic description, including location, displacement, angulation,
pattern (e.g., greenstick, oblique, transverse), and comminution.
Allman
-
Group I: fracture of the middle third
(80%). This is the most common fracture in both children and adults;
proximal and distal segments are secured by ligamentous and muscular
attachments. -
Group II: fracture of the distal third
(15%). This is subclassified according to the location of the
coracoclavicular ligaments relative to the fracture:
| Type I: | Minimal displacement: interligamentous fracture between the conoid and trapezoid or between the coracoclavicular and AC ligaments; ligaments still intact (Fig. 11.1) |
| Type II: | Displaced secondary to a fracture medial to the coracoclavicular ligaments: higher incidence of nonunion |
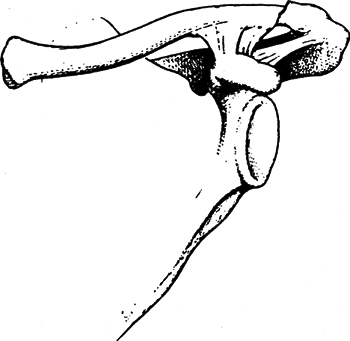
| IIA: | Conoid and trapezoid attached to the distal segment (Fig. 11.2) |
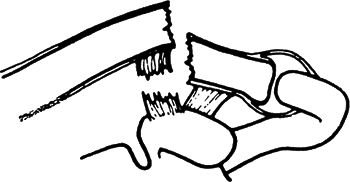
| IIB: | Conoid torn, trapezoid attached to the distal segment (Fig. 11.3) |
| Type III: | Fracture of the articular surface of the AC joint with no ligamentous injury: may be confused with first-degree AC joint separation (Fig. 11.4) |
 |
|
Figure 11.1. A type I fracture of the distal clavicle (group II). The intact ligaments hold the fragments in place.
(From Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD, eds. Rockwood and Green’s Fractures in Adults, 4th ed, vol. 1. Philadelphia: Lippincott-Raven, 1996:1117.)
|
P.123
-
Group III: fracture of the proximal third
(5%). Minimal displacement results if the costoclavicular ligaments
remain intact. It may represent epiphyseal injury in children and
teenagers. Subgroups include:Type I: Minimal displacement Type II: Displaced Type III: Intraarticular Type IV: Epiphyseal separation Type V: Comminuted ![]() Figure
Figure
11.2. A type IIA distal clavicle fracture. In type IIA, both conoid and
trapezoid ligaments are on the distal segment, whereas the proximal
segment without ligamentous attachments is displaced.(From Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD, eds. Rockwood and Green’s Fractures in Adults, 4th ed, vol. 1. Philadelphia: Lippincott-Raven, 1996:1118.)

 |
|
Figure
11.3. A type IIB fracture of the distal clavicle. The conoid ligament is ruptured, whereas the trapezoid ligament remains attached to the distal segment. The proximal fragment is displaced. (From Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD, eds. Rockwood and Green’s Fractures in Adults, 4th ed, vol. 1. Philadelphia: Lippincott-Raven, 1996:1118.)
|
P.124
OTA Classification of Clavicle Fractures
See Fracture and Dislocation Compendium at http://www.ota.org/compendium/index.htm.
TREATMENT
Nonoperative
-
Most clavicle fractures can be successfully treated nonoperatively with some form of immobilization.
-
Comfort and pain relief are the main
goals. A sling has been shown to give the same results as a
figure-of-eight bandage, providing more comfort and fewer skin problems.![]() Figure
Figure
11.4. A type III distal clavicle fracture, involving only the articular
surface of the acromioclavicular joint. No ligamentous disruption or
displacement occurs. These fractures present as late degenerative
changes of the joint.(From Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD, eds. Rockwood and Green’s Fractures in Adults, 4th ed, vol. 1. Philadelphia: Lippincott-Raven, 1996:1119.) -
The goals of the various methods of immobilization are as follows:
-
Support the shoulder girdle, raising the lateral fragment in an upward, outward, and backward direction.
-
Depress the medial fragment.
-
Maintain some degree of fracture reduction.
-
Allow for the patient to use the ipsilateral hand and elbow.
-
-
Regardless of the method of immobilization utilized, some degree of shortening and deformity usually result.
-
In general, immobilization is used for 4 to 6 weeks.
-
During the period of immobilization, active range of motion of the elbow, wrist, and hand should be performed.

P.125
Operative
-
The surgical indications for midshaft clavicle fractures are controversial.
-
The accepted indications for operative
treatment of acute clavicle fractures are open fracture, associated
neurovascular compromise, and skin tenting with the potential for
progression to open fracture. -
Controversy exists over management of midshaft clavicle fractures with substantial displacement and shortening (>1 to 2 cm).
-
Although most displaced midshaft
fractures will unite, studies have reported shoulder dysfunction and
patient dissatisfaction with the resulting cosmetic deformity.
-
-
Controversy also exists over management of type II distal clavicle fractures.
-
Some authors have indicated that all type II fractures require operative management.
-
Others report that if the bone ends are
in contact, healing can be expected even if there is some degree of
displacement. In this situation, nonoperative management consists of
sling immobilization and progressive range of shoulder motion.
-
-
Operative fixation may be accomplished via the use of:
-
Plate fixation: This is placed either on the superior or the anteroinferior aspect of the clavicle.
-
Plate and screw fixation requires a more
extensive exposure than intramedullary devices but has the advantage of
more secure fixation. -
Plate and screw fixation is more likely to be prominent, particularly if placed on the superior aspect of the clavicle.
-
-
Intramedullary pin (Hagie pin, Rockwood
pin): This is placed in antegrade fashion through the lateral fragment
and then in retrograde fashion into the medial fragment.-
Use of intramedullary fixation requires
frequent radiographic follow-up to monitor the possibility of hardware
migration and a second procedure for hardware removal. -
Intramedullary pins are prone to skin erosion at the hardware insertion site laterally.
-
-
Operative treatment of type II distal
clavicle fractures consists of reducing the medial fragment to the
lateral fragment. This is accomplished by using either coracoclavicular
fixation (Mersilene tape, sutures, wires, or screws) or fixation across
P.126
the AC joint, through the lateral fragment and into the medial fragment.
-
COMPLICATIONS
-
Neurovascular compromise: This is
uncommon and can result from either the initial injury or secondary to
compression of adjacent structures by callus and/or residual deformity. -
Malunion: This may cause an unsightly prominence, but operative management may result in an unacceptable scar.
-
The effect of malunion on functional outcomes remains controversial.
-
-
Nonunion: The incidence of nonunion
following clavicle fractures ranges from 0.1% to 13.0%, with 85% of all
nonunions occurring in the middle third.-
Factors implicated in the development of
nonunions of the clavicle include (1) severity of initial trauma, (2)
extent of displacement of fracture fragments, (3) soft tissue
interposition, (4) refracture, (5) inadequate period of immobilization,
and (6) primary open reduction and internal fixation.
-
-
Posttraumatic arthritis: This may occur after intraarticular injuries to the sternoclavicular or AC joint.