
Anesthesia and postoperative analgesia for foot, ankle, and knee. In
combination with femoral nerve block for surgery on the whole leg.
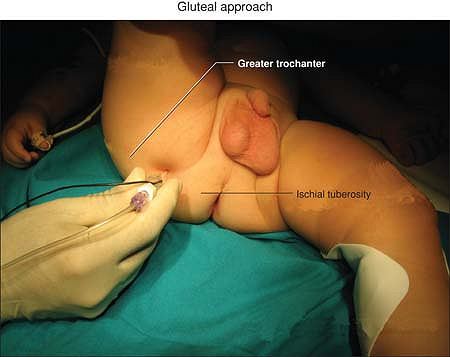
Many approaches have been described but the easiest way, by Dalens, is
to mark a line from the skin projection of the great trochanter to the
coccyx; the point of insertion of the needle is the midpoint of this
line, perpendicular to the skin, pointing to the ischial tuberosity.
Since the sciatic nerve is too deep it is impossible to detect it via
transcutaneous stimulation. Therefore, insert the needle connected to
the nerve stimulator set at 1 mA and 2 Hz, and advance it until the
motor response of the foot and toes is elicited (dorsiflexion of the
toes and foot or eversion following stimulation of the common peroneal
nerve, or plantar flexion of the toes and foot or inversion following
stimulation of the tibial nerve). Adjust the position of the needle to
maintain the appropriate muscle response with a current of 0.4 to 0.5
mA. Then, after negative aspiration, slowly inject the local anesthetic
solution.
-
There are no particular contraindications or side effects except the vessel puncture of the inferior gluteal artery.
-
A potential error could be the local anesthetic injection upon stimulatory response from the gluteal muscles.
-
A combined sciatic and femoral or
saphenous nerve block can be used for most lower extremity surgeries.
In this case the total dose of local anesthetic must be reduced for
each block.
B, Tanguy A, Vanneuvile G. Sciatic nerve block in children: a
comparison of the posterior, anterior and lateral approaches in 180
paediatric patients. Anaesth Analg 1990;70:131.
Very easy to perform in small children, supine with both the leg
maintained flexed on the abdomen at 90° and the knee flexed at 90°
helped by a nurse.
Anesthesia and immediate postoperative analgesia for foot, ankle, and
knee. In combination with femoral nerve block for surgery on the whole
leg.
The shorter distance from skin to nerve compared with the posterior
approach allows the use of nerve mapping, then insert the needle
perpendicular to the skin in the midpoint of the line joining the
greater trochanter with the ischial tuberosity. Connect to the nerve
stimulator set at 1.5 mA and 2 Hz, and advance it until the motor
response of the foot and toes is elicited (dorsiflexion of the toes and
foot or eversion
following
stimulation of the common peroneal nerve, or plantar flexion of the
toes and foot or inversion following the stimulation of the tibial
nerve). Adjust the position of the needle to maintain the appropriate
muscle response with a current of 0.4 to 0.5 mA. Then, after negative
aspiration, slowly inject the local anesthetic solution.
 |
|
Figure 48-1. Gluteal approach anatomic landmarks.
|
-
There are no particular contraindications or side effects except the vessel puncture of the inferior gluteal artery.
-
A potential error could be the local anesthetic injection upon stimulatory response from the gluteal muscles.
-
A combined sciatic and femoral or
saphenous nerve block can be used for most lower extremity surgeries.
In this case the total dose of local anesthetic must be reduced for
each block. -
In older children this block can be performed placing the patient in lateral position with the same landmarks.
B, Tanguy A, Vanneuvile G. Sciatic nerve block in children: a
comparison of the posterior, anterior and lateral approaches in 180
paediatric patients. Anaesth Analg 1990;70:131.
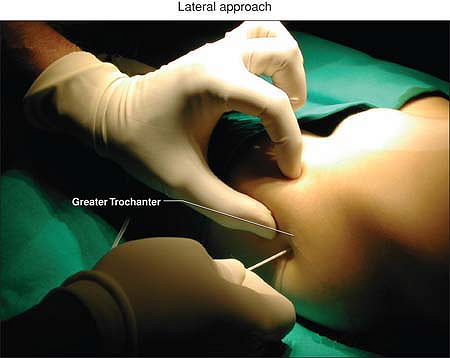
Find and mark the lateral skin projection of the greater trochanter of
the femur. The site of introduction of the needle is 1 to 3 cm below
the greater trochanter. Since the sciatic nerve is too deep it is
impossible to detect it via transcutaneous stimulation. Therefore
insert the needle connected to the nerve stimulator set at 1 mA and 2
Hz, just below the trochanter perpendicular to the skin and advance it,
passing below the femur, until the motor response of the foot and toes
is elicited (dorsiflexion of the toes and foot or eversion following
stimulation of the common peroneal nerve, or plantar flexion of
the
toes and foot or inversion following the stimulation of the tibial
nerve). Adjust the position of the needle to maintain the appropriate
muscle response with a current of 0.4 mA. Then, after negative
aspiration, slowly inject the local anesthetic solution.
 |
|
Figure 48-2. Lateral approach anatomic landmarks.
|
-
Lateral sciatic nerve block is effective,
safe, and simple and there is no need to mobilize the child. Since
children are often sedated during the performance of the block, with
this approach the child is in spontaneous ventilation and can breathe
properly. -
There are no particular contraindications or side effects.
-
If a femur contraction occurs, the insertion of the needle is too ventral; remove the needle and insert it slightly below.
-
A combined sciatic and femoral or
saphenous nerve block can be used for most lower extremity surgeries.
In this case the total dose of local anesthetic must be reduced for
each block.
B, Tanguy A, Vanneuvile G. Sciatic nerve block in children: a
comparison of the posterior, anterior and lateral approaches in 180
paediatric patients. Anaesth Analg 1990;70:131.
Anesthesia and postoperative analgesia for lower extremity surgery,
especially for ankle and foot, except for the medial aspect of the
thigh, supplied by the saphenous nerve.
The popliteal fossa, the tendons of the biceps femoris and
semitendinosus muscle, the medial and lateral epicondyle of the femur.
Find and mark the bisector of the angle created by the summit of the
popliteal fossa, formed by the tendons of the biceps femoris and the
semitendinosus. The point of puncture is located 1 cm lateral to this
bisector at the junction of the upper one-third with the lower
two-thirds of the line extending from the apex of the popliteal fossa
to the intercondylar line. Set the nerve stimulator at a frequency of 2
Hz and a current of 2.5 mA. Connect this to the pen dedicated for the
transcutaneous technique (instead of the pen it is possible to use the
negative electrode of the ENS) and point it to the skin cranially with
a 30° angle direction until a motor response of the foot and toes is
elicited (dorsiflexion of the toes and foot or eversion following
stimulation of the common peroneal nerve, or plantar flexion of the
toes and foot or inversion following stimulation of the tibial nerve).
Then insert the needle connected to the nerve stimulator set at 1 mA
and 2 Hz, exactly at the point evidenced via transcutaneous in a
cranial direction until the motor response is again elicited. Adjust
the position of the needle to maintain the appropriate muscle response
with a current of 0.4 to 0.5 mA. Then, after negative aspiration,
slowly inject the local anesthetic solution.
-
A combined sciatic and femoral or
saphenous nerve block can be used for most lower extremity surgeries.
In this case the total dose of local anesthetic must be reduced for
each block. -
One complication could be vessel puncture (popliteal artery and vein).
FJ, Gouverneur JM, Gribomont BF. Popliteal sciatic nerve block aided by
a nerve stimulator: a reliable technique for foot and ankle surgery. Reg Anesth 1991;16(5):278–281.
The patient is supine, with the leg in a neutral position or slightly
rotated inward, the leg to be blocked elevated on a pillow at the knee
level.
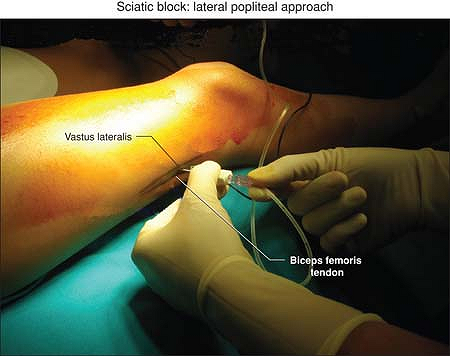
Find and mark the lateral skin projection of the patellar crest, then
palpate the biceps femoris tendon. Palpate the inferior border of the
vastus lateralis muscle and identify the groove between the tendon and
the muscle. Since the sciatic nerve is too deep it is impossible to
detect it via transcutaneous stimulation. Therefore insert the needle
connected to the nerve stimulator set at 1 mA and 2 Hz, in a horizontal
plane with
a
cephalad angulation and advance it until the motor response of the foot
and toes is elicited (dorsiflexion of the toes and foot or eversion
following stimulation of the common peroneal nerve, or plantar flexion
of the toes and foot or inversion following stimulation of the tibial
nerve). At this level both the tibial branch and the peroneal branch
are still together because the division of the sciatic nerve into the
two branches occurs at about 5 to 8 cm above the crease at the knee so
that the insertion of the needle at 7 cm can easily find both twitches.
Adjust the position of the needle to maintain the appropriate muscle
response with a current of 0.4 to 0.5 mA. Then, after negative
aspiration, slowly inject the local anesthetic solution.
 |
|
Figure 48-3. Lateral popliteal approach anatomic landmarks.
|
-
Lateral sciatic nerve block is effective,
safe, and simple and there is no need to mobilize the child. Since
children are sedated during the performance of the block it is better
to use the lateral approach both at the trochanter level and at the
popliteal level, since in this way the child is in the supine position
and can breathe properly. -
A combined sciatic and femoral or
saphenous nerve block can be used for most lower extremity surgeries.
In this case the total dose of local anesthetic must be reduced for
each block. -
A complication could be the vessel puncture (popliteal artery and vein).
DH, Wong DV, et al. Lateral popliteal sciatic nerve block compared with
ankle block for analgesia following foot surgery. Can J Anaesth 1995;42:765–769.
JD, Hadzic A, Kitain E. Anatomic considerations for sciatic nerve block
in the popliteal fossa through the lateral approach. Reg Anesth 1997;84:387–390.