
VII – NEOPLASTIC, INFECTIOUS, NEUROLOGIC AND OTHER SKELETAL DISORDERS
> Amputations > CHAPTER 122 – PRINCIPLES OF AMPUTEE PROSTHETICS
Orthopaedic Surgery, Weill Medical College of Cornell University;
Metabolic Bone Disease Service, Hospital for Special Surgery, New York,
New York 10021.
limb from either a functional or a cosmetic viewpoint. In the last
decade, however, modern technology and improved materials have closed
the gap considerably (1,3,4,11).
The result is that motivated individuals with no additional health
problems can now expect to regain a degree of function that will allow
them to pursue an active life style of their choice. Limitation of the
maximum performance possible should not be a consequence of either an
inadequate prosthesis or negative expectations of the health care
providers. Patients’ cooperation and positive attitude are critical.
educated about the operative procedure, receive psychosocial support,
be fitted with a comfortable prosthesis, and engage in aggressive
rehabilitation. Good communication between members of the health care
team and patients cannot be emphasized strongly enough. Encouragement
and positive reinforcement go a long way toward helping patients
achieve their goals (see Chapter 120 and Chapter 121 for discussion of the principles of lower- and upper-extremity amputations, respectively).
components can often result in significantly better function than an
amputation that results in a longer lever arm with the use of more
basic and primitive components (16,18).
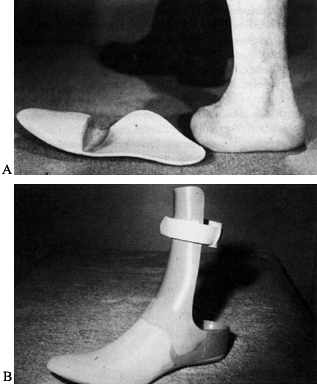
ability to walk without a prosthesis. The disadvantages at this site
include the difficulty in making a cosmetic prosthesis with “toe off”
function, the uneven gait that results without toe-off function, the
tendency to develop an equinovarus deformity in the residual foot
stump, and the limited foot components available (Fig. 122.1).
 |
|
Figure 122.1. A: Midfoot amputation with a shoe insert prosthesis. B: An ankle–foot prosthesis for amputations through the hindfoot other than a Syme’s amputation. (From Dee R, Mango E, Hurst LC. Principles of Orthopaedic Practice. New York: McGraw-Hill, 1989:365, with permission.)
|
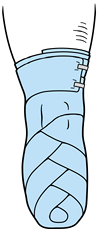
this technique is that limited ambulation is possible without a
prosthesis. Its disadvantages include a less cosmetic prosthesis due to
the thick ankle required to accommodate the stump, the limited foot
components available, and the limited amount of energy storage within
these components (Fig. 122.2).
 |
|
Figure 122.2. Syme’s prosthesis with posterior cutout for donning the prosthesis. (Courtesy of the Joyce Center, Manhasset, NY.)
|
selected, it is preferable to have enough space distally to incorporate
appropriate prosthetic components for best function and cosmesis, while
maintaining adequate length of the residual limb. Ideally, the length
of tibia from the mid-knee joint to the distal end should be no less
than 4 in. (10 cm) and no more than 7 in. (17.75 cm). If the tibia is
too long, the choice of components is limited and cosmesis may be
compromised. The space from the floor to the end of the residual limb
(after the incision is closed) should be at least 12 in. (30.5 cm), but
not if it will leave the length of the tibia less than 4 in. (10 cm).
end bearing in the prosthesis, a long lever arm, and condylar
suspension. A knee disarticulation is particularly good for patients
with poor gait and neuromuscular control. It is important in children
with growth potential who need their distal femoral epiphysis to retain
stump length. The disadvantages of this technique include the limited
knee components available (including a button rotator), the differences
in the center of rotation of the two knees, poor cosmesis due to the
large femoral condyles, and atrophy of the thigh that occurs with
condylar suspension. High-performance function is better achieved with
a long transfemoral
amputation and a prosthesis with modern knee components.
in. (10 cm) from the knee center to the distal end of the residual limb
is optimum, as long as this is not greater than one-third the length of
the femur. This space permits a greater choice of knee and other
components, and function and cosmesis are improved (Fig. 122.3).
 |
|
Figure 122.3.
A transfemoral socket shows a valve hole and one-way valve for suction application. This is a transfemoral prosthesis with a button rotator, hydraulic swing-stance knee, and carbon-composite ankle–foot system with shock-absorbing pylon. (Courtesy of the Joyce Center, Manhasset, NY.) |
improved comfort and reduced the workload of patients wearing these
types of prostheses (Fig. 122.4).
 |
|
Figure 122.4. Endoskeletal prosthesis with foam cover for a hip disarticulation. (Courtesy of the Joyce Center, Manhasset, NY.)
|
These can be achieved through one of several methods: an immediate
postoperative prosthesis or serial wrapping of the residual limb with
an elastic bandage or an elastic shrinker. The overall aim is to reduce
postsurgical edema. This in turn reduces postsurgical pain, minimizes
later phantom pain, increases circulation (therefore hastening
healing), and prepares the operative site and residual limb for a
preparatory prosthesis. Where possible, elevation of the affected limb
can also help reduce edema, although this must be accompanied by
immediate aggressive physical therapy to prevent contractures of the
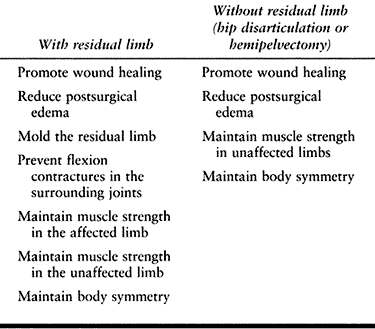
surrounding joints. When there is no residual limb, the postsurgical
goals are fewer (Table 122.1). Methods to
reduce postoperative edema and prevent breakdown of the incision in
patients include turning the patient onto the sound side and early
mobilization.
 |
|
Table 122.1. Goals of Preprosthetic Care
|
weight-bearing areas to enable patients to ambulate as soon as it is
practical. The IPOP incorporates an adapter into its distal end that
has a removable pylon with a prosthetic foot attached.
ambulation, and prevent flexion contractures, as well as to keep
patients from “waking up without a leg.” The prosthetist applies a
specially padded and molded cast in the operating room after the
surgical dressings have been applied. The advantage of this technique
is that the cast initially prevents postsurgical edema, promoting wound
healing and reducing pain. The cast also protects the residual limb,
prevents flexion contractures in the surrounding joints, and molds the
residual limb while compression is maintained. The difficulties with
this technique are that the cast loosens as soon as the edema subsides
and the subsequent pistoning action can cause tissue breakdown. The
cast must either be continually replaced or be removable so that
additional socks or fillers can be used to maintain compression. Other
difficulties involve the heaviness of the cast, which prevents movement
of the contained joints, impedes walking, and leads to muscle atrophy.
The cast must be removed to monitor wound healing, frequently needs to
be reapplied to contain compression, and is not cosmetic. Auxiliary
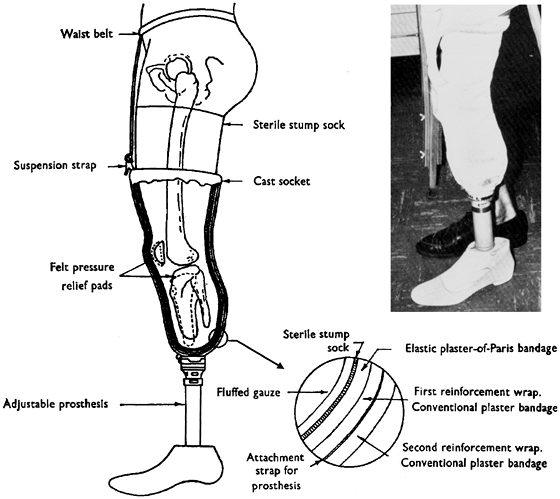
suspension may be required (Fig. 122.5).
 |
|
Figure 122.5.
IPOP after a below-knee amputation. Surgical dressings are applied first. The prosthetist then rolls a stump sock into place, pads the end of the stump and bony prominences with specially designed cushioning materials, and applies a well molded plaster cast that incorporates the knee, with a hole left for the patella, and extends up to the mid thigh. This is held in place by a suspension strap hooked to the stump sock and tied to a band around the waist. A connection for a pylon is incorporated into the end of the cast. The pylon is applied postoperatively when the patient is ready to be mobilized. (From Fulford GE, Hall MJ. Amputation and Prostheses. Philadelphia: Williams & Wilkins Co.: 14, with permission.) |
it can be reapplied whenever it becomes loose and therefore compression
can be kept constant. Patients can be taught to wrap the limb, and
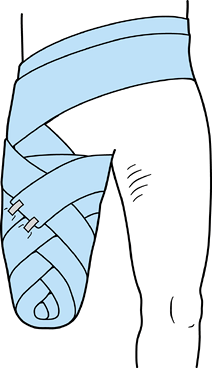
compression can be applied only in areas where it is needed (Fig. 122.6 and Fig. 122.7).
The problem with a compression dressing is that it may be wrapped too
tightly, causing pain or tissue breakdown, or too loosely to be
effective. Patients may have difficulty wrapping it themselves, and it
may cause window edema when applied incorrectly or unevenly.
 |
|
Figure 122.6.
Figure-eight wrap for a transfemoral amputation. The wrap is applied around the stump and subsequently around the waist, progressing from distal to proximal. The dressing is gently wrapped to avoid overconstriction, and more compression is applied distally than proximally. |
 |
|
Figure 122.7.
Figure-eight elastic wrap for a below-knee amputation. The wrap is applied, progressing from distal to proximal, with the pressure graduated so that more compression is provided distally. The bandage should not be applied too tightly. |
overall compression and allow wound monitoring. They may be difficult
to apply correctly in some individuals, however, and may not put direct
pressure over areas where it is needed (Fig. 122.8).
 |
|
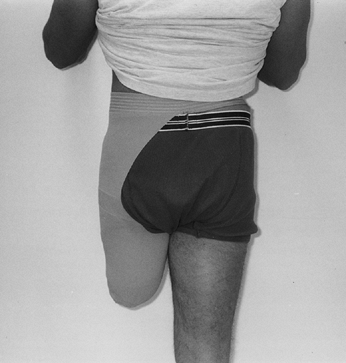
Figure 122.8. Elastic shrinker for a transfemoral residual limb. (Courtesy of the Joyce Center, Manhasset, NY.)
|
ability and cooperation of a patient, the length of the limb, and
careful evaluation of the goals for the individual.
motion in the surrounding joints (hip and knee), prevention of muscle
atrophy, and elimination of pain. To achieve these, physical and
occupational therapy consisting of range-of-motion, stretching, and
strengthening exercises should be initiated as soon as possible. An
early fit of the prosthesis will be beneficial.
the amputated limb undergoes normal maturational shape changes after
surgery. Fitting should be started after the sutures or staples have
been removed and the incision has healed.
lower-extremity prosthesis include controlling postsurgical edema,
minimizing the loss of muscle mass and strength, preventing joint
contractures, and allowing patients to ambulate. Historically,
preparatory prostheses were made with the simplest components, worn
with prosthetic socks, and suspended with straps and belts. To
accommodate postsurgical shrinkage and muscle atrophy of the residual
limb, the ply of the socks was increased until the size of the limb
stabilized, at which time the definitive prosthesis would be
fabricated. However, new socket materials and designs, along with
modern components and more aggressive training, promote the use of
remaining muscle so that after postsurgical edema has subsided, there
is often little or no muscle atrophy. If appropriate for an individual,
one of several types of suction suspension can often be used as soon as
the incision is completely healed, replacing the socks and belts. With
the use of more sophisticated components, correct gait can be taught
immediately to avoid retraining once the definitive prosthesis has been
fit.
the components are aligned, patients should be taught how to use the
prosthesis. Limit ambulation to partial weight bearing, and check the
residual limb frequently; graduate to total weight bearing as
tolerated. How long this takes will depend on the fit of the
prosthesis, as well as the strength, coordination, ability, and
determination of the patient.
change shape for the lifetime of individuals, the most dramatic changes
occur during the first 3–6 months. Constantly monitor and modify the
socket, or change the sock ply to accommodate these changes to maintain
fit. Make patients aware that this is quite normal. The definitive
prosthesis is fabricated once these changes have stabilized.
thoroughly examines a patient and evaluates the medical history. A
detailed explanation of the process of prosthetic fitting, preferably
accompanied by written materials, is given to the patient. A
prescription recommendation is sent to the referring physician by the
prosthetist with a request for a letter of medical necessity. The
primary concerns are comfort, function, and cosmesis. The prescription
recommendations depend on the patient’s age, previous activity level,
hoped-for outcome, length of residual limb, medical history, and
reimbursement limitations. The prescription should include type of
prosthesis (endoskeletal versus exoskeletal), type of suspension,
socket design, materials, choice of components, and cosmetic finish.
and depends on the skill of the person taking the measurements or the
impression of the residual limb, as well as on the materials used.
Initially, measurements are taken, and a negative wrap of the residual
limb (or digitized equivalent; see below) is made. A positive model is
produced from the impression and modified, and a clear diagnostic
socket is formed over that mold. The diagnostic socket is fitted to the
residual limb, the fit is checked, and any indicated changes are made
to the positive model, with refitting of the socket if necessary. A
flexible, total-contact socket is formed within a rigid frame, and the
chosen components are aligned so that the foot, knee joint, and so on
are in a neutral alignment. The prosthesis is then fitted and
dynamically aligned, and initial gait training is performed while the
alignment is fine-tuned. After the prosthesis is delivered to the
patient for trial use, a protective cosmetic cover is fabricated, and
further alignment and fitting changes are made, as necessary, on the
basis of continued functional examination.
residual limb and manually modify the positive mold to fabricate a
socket, an alternative method is the computer-aided
design/computer-aided manufacturing (CAD/CAM) system. With this system,
information on the residual limb is converted into numerical data, read
into the computer by a digitizer (usually from a negative mold), and
converted into a three-dimensional image by commercially available
software. Modifications to this image are made by the prosthetist; the
information is then relayed to the attached carver, which produces the
positive model. Thereafter, the processes are similar regardless of
whether the manual or the CAD/CAM method is used: A hard, clear
diagnostic socket is formed over the model and then fitted on the
residual limb. Weight-bearing surfaces and bony or sensitive areas are
checked, and any necessary modifications are made to the diagnostic
socket before the definitive one is fabricated.
bench-aligned, a dynamic alignment must be done with the patient
wearing the prosthesis. There are two schools of thought concerning
alignment: According to one school, the prosthesis is aligned to
accommodate any abnormalities in posture, such as flexion contracture,
whereas with
the
second gradual corrections in alignment are made simultaneously with
aggressive rehabilitation of the patient, until a more correct
alignment can be obtained.
of the prosthesis to make the corrections and adjustments that will
inevitably be needed as a patient progresses. It is important that
patients understand that this is a normal process and that a plateau
will eventually be reached where it will only be necessary to have
routine check-ups, unless a new prosthesis needs to be fabricated. They
must be informed of the importance of maintaining a stable body weight
and a regular exercise program. Excessive gain or loss of weight
compromises fit and function of a prosthesis. Many of today’s
components are designed for a weight range or activity level.
It is modular in design, thus permitting greater interchangeability.
The advantages of the endoskeletal are that changes in alignment can be
made with ease at any time during the life of the prosthesis to
accommodate changes in posture, gait, or growth. In the modular design,
individual components can be changed without remaking the prosthesis.
The problems with this technique are that it is more expensive and may
require more maintenance.
 |
|
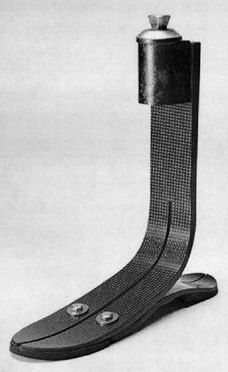
Figure 122.9.
Endoskeletal type of prosthesis, without socket. A Flex-Foot, Inc. prosthetic foot has a shank component composed of carbon fiber epoxy. This prosthesis stores energy during the stance phase and returns it to the amputee for push-off. A foam cover will be added for cosmesis. |
Once fabricated, it has limited adjustability without being
refabricated. It is less expensive and has a more durable cover than
the endoskeletal type. Its disadvantages include no postdelivery
accommodation–alignment changes, limited dynamic response capability,
and limited component choices. In addition, it is frequently heavier
than the endoskeletal prosthesis.
 |
|
Figure 122.10.
Exoskeletal type of below-knee prosthesis. This patellar tendon–bearing type of below-knee prosthesis has a Pelite liner and supracondylar suspension. (From D’Astous J, ed. Orthotics and Prosthetics Digest. Canada: Edahl Productions Ltd., 1981:113 with permission.) |
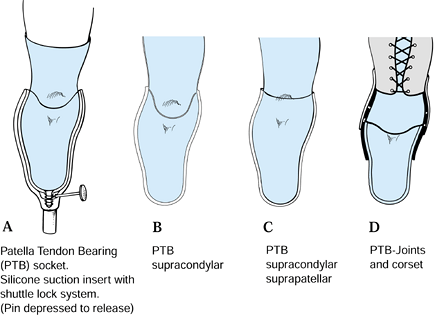
belt, or cuff strap. The suction technique aims to reduce pistoning in
the socket, thus requiring less energy expenditure during ambulation (Fig. 122.11).
It promotes venous return and gives patients the feeling that the
prosthesis is lighter. In addition, it eliminates the need for
uncomfortable belts and straps.
 |
|
Figure 122.11. Types of suspension for transtibial amputees. A:
Traditional patellar tendon–bearing (PTB) total-contact socket with a silicone socket suspension system in which the suction unit attaches to the socket by a shuttle-lock system. If this is not used, a supracondylar suspension strap can be added. B: PTB supracondylar prosthesis. C: PTB supracondylar/suprapatellar socket. D: PTB prosthesis incorporating side hinges and joints with a thigh corset. |
residual limb is drawn into the socket with an elastic bandage or a
type of pull sock until the air is displaced through the distal valve
hole; a one-way valve is placed in the valve hole to prevent air from
reentering the socket (Fig. 122.3).
Although it seems easier to lubricate the residual limb and push it
into the socket, the result is hammocking (stretching) of tissues on
the distal end and failure to get all the proximal tissue into the
socket.
several silicone or gel liners with a distal locking mechanism can be
used. These are rolled up onto the residual limb, with the liner
holding onto it; and the distal locking mechanism attaches mechanically
to the prosthesis, creating an alternative suction fit.
application. The distal end of the sleeve fits over the proximal
portion of the prosthesis. The proximal end of the sleeve is then
pulled up over the knee onto the patient’s thigh. It can act as a
suction device if it is made of nonporous material.
transtibial applications when suction suspension is not an option. It
can be used in conjunction with a socket interface, socks, or silicone
gel liner that has no locking mechanism.
applications when suction is not an option. It is sometimes used in
conjunction with a waist belt.
important factor in a successful outcome. Today’s sockets are designed
to fit more anatomically and to provide total contact with the residual
limb. Increased suction on the distal end of the residual limb, due to
lack of contact, results in verrucous hyperplasia, if left uncorrected.
Under extreme circumstances, this can lead to localized infection or
cellulitis.
surrounded by a rigid frame to support the weight-bearing areas. The
quadrilateral socket for the transfemoral amputee is being replaced by
one of several versions of ischium-containing designs. Containment of
the ischium within this type of socket provides pelvic stability and
promotes more normal femoral alignment and better function of the
remaining intact musculature. Proprioception is also increased.
higher transfemoral, hip-disarticulation, or hemipelvectomy
amputations. The bucket socket is made of laminated silicone or
flexible plastic supported by a rigid frame (Fig. 122.4). The new families of silicone or gel socket liners have improved the comfort of sockets.
prosthesis should be used. It is our opinion that the more debilitated
a patient is, the greater is the need for help from the prosthesis. The
question posed should be, “What can we provide to make walking easier
and more efficient for a person?” rather than making the assumption
that this person is not “a candidate for ambulation.” The components
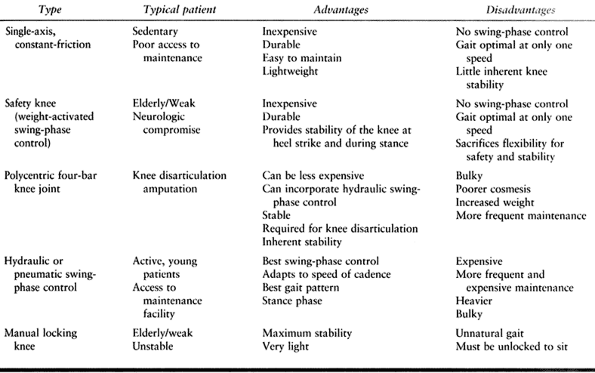
requiring consideration are the hips, the knees, and the feet.
constant-friction knee is the simplest design. The main drawback for
this component is that ambulation is normal only at one speed for a set
amount of friction. The safety knee with constant friction is designed
so that the patient’s weight locks the knee in the standing position.
The polycentric knee joint has hinges external to the prosthesis and
was originally designed for through-the-knee prostheses. It provides
better control during standing and the stance phase of gait. The swing
phase may be controlled mechanically or with a hydraulic cylinder.
Hydraulic knee joints, which are the most sophisticated on the market
to date, control both swing and stance phase and are
velocity-sensitive. Table 122.2 specifies the indications for use of the various types of prostheses, together with advantages and disadvantages.
 |
|
Table 122.2. Knee Joints for Above-Knee Prosthesis
|
groups: articulated ankle joints, dynamic-response and energy-storing
foot, and nondynamic-response and/or energy-storing feet. The simplest
and cheapest combination is the nonarticulated ankle and the
nondynamic-response foot, called the solid ankle-cushion heel (SACH)
foot; it is also the least efficient.
foot allows maximum loading of the toe section of the foot during
“rollover.” Similar to the action of a coiled spring, when the pressure
or loading is removed, the toe section springs back to provide
push-off. The most extreme version of this is found in a foot–ankle and
shank made of carbon fibers, in which the loading action or energy
storage is also carried out in the shank. The method of loading the toe
must be taught, or the benefits will not be experienced. In fact, users
may complain that the toe is too stiff, and reject the foot.
considerable time walking on uneven ground, is heavier than other
prosthetic feet and requires more maintenance. An added disadvantage is
that even if it is combined with a dynamic-response foot, the action of
the ankle precludes loading the toe to provide push-off. The various
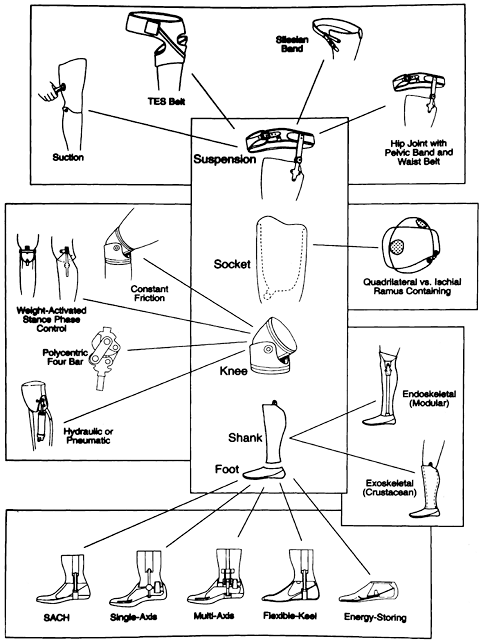
options for lower-extremity prosthetic components are shown in Figure 122.12.
 |
|
Figure 122.12. Choice of components for the transfemoral amputee. (From Braddon RL. Physical Medicine and Rehabilitation. Philadelphia: W.B. Saunders, 1996:307, with permission, University of Texas Health Science Center at San Antonio.)
|
and training as it does on the fabrication and fitting of a prosthesis.
Studies show that energy expenditure during ambulation is higher for
amputees than for nonamputees (2,6,7,9,10,14,15,19).
Factors affecting energy expenditure include the length of the residual
limb, unilateral or bilateral amputation, the reason for amputation,
the choice of prosthetic components, the weight of the prosthesis and
whether the weight is concentrated distally or proximally, the
efficiency of the suspension aids for the prosthesis, the symmetry of
the gait, the state of the cardiovascular system, the patient’s age,
and the general state of physical fitness (5,11).
is higher than normal in most untrained amputees and increases as the
amputation level gets higher. In addition, the preferred speed of
walking becomes slower (8). The weight of the
prosthesis can contribute to this increased energy cost, particularly
if the extra weight is distal. Suction suspension can make a prosthesis
feel lighter, while pistoning between residual limb and socket creates
a pendulum effect. Careful choice of components is therefore very
important. A less symmetric gait also requires more energy. Elderly
individuals who have an amputation for vascular reasons are less
efficient partly because of the aging process but also as a result of
arteriosclerotic heart disease, peripheral vascular disease, or
diabetes, which all inhibit the efficient transfer of oxygen to the
muscles.
exercises as soon as possible after amputation to maintain flexibility,
prevent flexion contractures, and preserve muscle strength and mass. In
addition, make an aerobic conditioning program a part of the
rehabilitation process whenever possible. This combination will have
the dual effect
of
strengthening the cardiovascular system so that there is more efficient
transfer of oxygen and building up muscles to use that oxygen (8). Once a prosthesis has been fitted, patients should do all physical therapy and exercise programs with the prosthesis on.
in the prosthesis. Even if only partial weight bearing is allowed,
encourage amputees to stand up straight and take even strides. It is
easier to teach someone correctly from the beginning than to try to
correct a bad habit later, just as it is easier to prevent a flexion
contracture than to correct it. Although walking frames are frequently
used, particularly by the elderly, they have the disadvantage of
encouraging users to walk unevenly. Typically, a long step is taken
with the sound side to the front of the frame, and the prosthetic side
is then only brought even with the sound side. If a walker must be used
for stability, it should be moved forward before each footstep to allow
room for the feet to be placed sequentially one in front of the other.
of new amputees. Functional muscle-strengthening exercises—those that
are carried out standing on the prosthetic side while exercising the
sound side—are as important as exercises carried out on the affected
side.
amputees will stand and walk with their affected-side hip behind their
sound-side hip, even though the shoulders will remain straight. The
result is that the stride length is uneven, with the stride taken with
the prosthesis being longer than that with the sound side. Use of an
energy-storing/dynamic-response foot will in effect prevent loading of
the toe and the resulting toe push-off. It has therefore been our
practice to gait-train our clients in the following way:
-
At heel strike on the affected side,
contract the muscles on that side from the gluteals to the end of the
residual limb and push down and back. -
Move the affected hip forward until the
foot is flat on the floor while rolling forward (not up) onto the toe
of the sound side and starting the sound-side swing phase. -
Move the affected hip farther forward,
feeling the stretch in the hip flexors, compressing and loading the
prosthetic toe while completing the swing phase of the sound side. -
At heel strike on the sound side, relax
the muscles on the affected side. The prosthetic toe will push off,
initiating a knee bend and affected-side swing-through.
work of loading the prosthetic toe. It is also important to maintain
normal upper-body movement, that is, equal arm swing and torso
rotation. Although it seems to be very difficult work initially, the
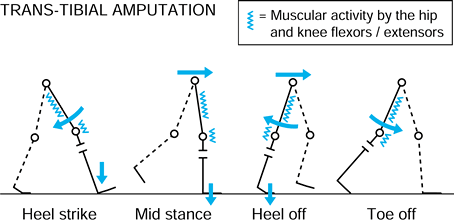
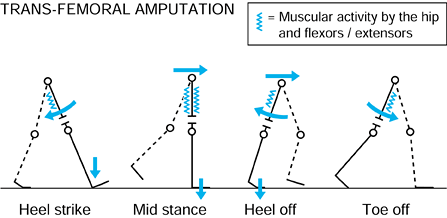
result is a more even gait pattern and less work. Figure 122.13 and Figure 122.14 depict the appropriate activity of the muscles during gait for transtibial or transfemoral amputation.
 |
|
Figure 122.13. Muscle activity in the flexors and extensors of the hip and knee during the gait cycle for a transtibial amputee.
|
 |
|
Figure 122.14. Muscle activity flexors and extensors of the hip in a transfemoral amputee during the full-gait cycle.
|
conditioning program will improve the endurance of all lower-extremity
amputees—it is not only for athletes. In our experience, as long as a
prosthesis fits well, a tailored exercise program can be undertaken by
individuals with diabetes and circulatory insufficiency, and they will
benefit. Stationary bicycles, rowing machines, or upper-body ergometers
can all be used, although the treadmill is the piece of equipment of
choice because it also improves walking. Ideally, in addition to
stretching and muscle-strengthening exercises, these individuals should
exercise for a minimum of 20 minutes at least three times per week at
an elevated heart rate determined by their physicians.
prosthesis, members of the prosthetic team must observe the patient’s
gait on a straight-level walkway to be certain that gait abnormalities
are not due to inadequate rehabilitation or improper fitting or
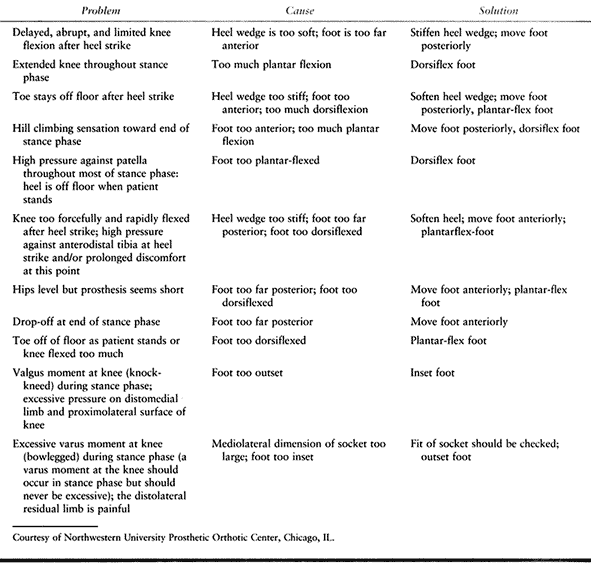
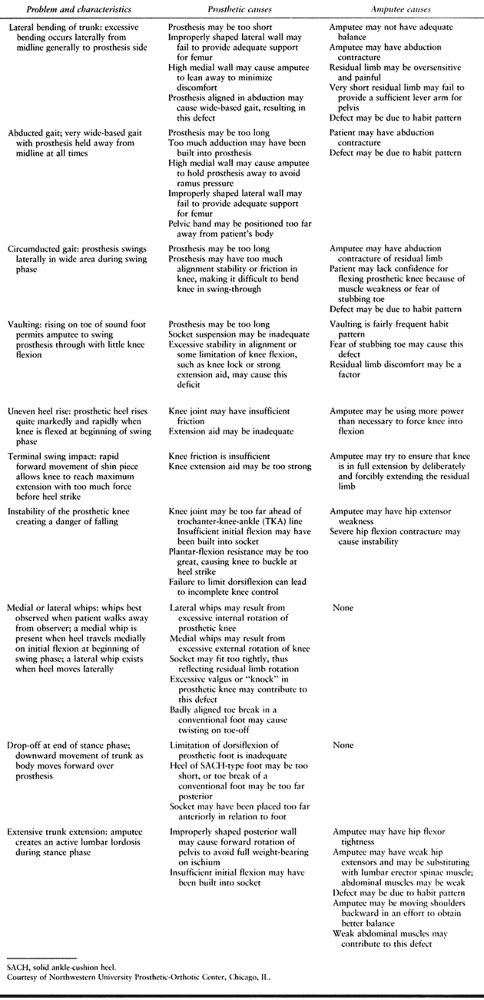
alignment of the prosthesis. Table 122.3 and Table 122.4
provide an outline of commonly observed gait abnormalities, a
description of their characteristics, and common causes that require
correction.
 |
|
Table 122.3. Gait Analysis of the Transtibial Amputee
|
 |
|
Table 122.4. Gait Analysis of the Transfemoral Amputee
|
disarticulation, below-elbow amputation, elbow disarticulation,
above-elbow amputation, shoulder disarticulation, and forequarter
amputation. Wrist disarticulation has the greatest range of extremity
motion: flexion, extension, pronation, and supination. It also has a
long lever arm for strength and support of distal components, and
increased proprioception and function. However, it is more difficult to
fit with a myoelectric hand and wrist, and the resulting fit is often
longer than the sound side. The choice of components is limited.
pronate and supinate, has a wider range of components available, and
can achieve equal length with the sound side. The choice of a
myoelectric or body-powered prosthesis is available. This amputation
has less range of motion, a shorter lever arm, and less proprioception
and function than the wrist disarticulation. Anatomic pronation and
supination decrease as the length of the residual limb decreases.
potential increased prosthetic range of motion, for the
shoulder-to-elbow portion, when fitted with a prosthesis, will
be
longer than the opposite extremity than with the above-elbow
amputation. The increased length at the elbow is due to the components,
but casual observers do not detect the discrepancy. Choice of elbow
components is limited to body-powered devices.
components, either myoelectric or body-powered. It has a short lever
arm to support distal components and a limited potential range of
motion.
leave patients with significant disability. The shoulder
disarticulation has a very limited range of motion, and the prosthesis
is cumbersome and heavy. It is frequently used primarily for cosmesis.
The forequarter amputation also has a limited range of motion. The
prosthesis is even more cumbersome and heavy, and suspension is
particularly difficult. The more distal the amputation in the upper
extremity is, the more functional the outcome and the better the
cosmesis will be.
postsurgical pain and edema, improving circulation through reduced
edema. Patients benefit psychologically by “waking up with a hand and
arm.”
upper-extremity prosthesis can protect the residual limb from injury,
prevent and treat contractures in the contained joints, and initially
mold the residual limb. Patients maintain some two-handed function and
receive training in the use of a prosthesis. It also allows assessment
of a patient’s motivation. It can be removed for wound care and helps
maintain body symmetry. The IPOP is usually worn only for 2–6 weeks
after surgery. It is body-powered rather than myoelectric, and because
of its weight, it uses a terminal hook device rather than a hand.
prevents movements of contained joints, resulting in muscle atrophy. If
the cast becomes loose, it can cause tissue breakdown, particularly if
it is resting on the transradial area or other proximal joint. The cast
is also prone to fall off, particularly with transhumeral amputations,
unless auxiliary suspension is used. Use of a cast also prevents
monitoring of the incision. Another problem with this technique is that
the terminal hook device is not cosmetic. An IPOP cannot be applied
over extensive skin grafting and is not useful on very short residual
limbs.
than for lower-extremity prostheses, with rejection rates increasing
the more proximal the amputation site is. If prosthetic fitting is not
done early, the client can become so adept at doing tasks with one hand
that a prosthesis may seem cumbersome and heavy.
residual limb are the determining factors in the choice of a prosthetic
system. Personal preference and motivation also play a role.
upper-extremity amputations is critical for maximum function. This
differs from the principles for the lower-extremity, where components
can be more functional and a long residual limb length is not always
beneficial.
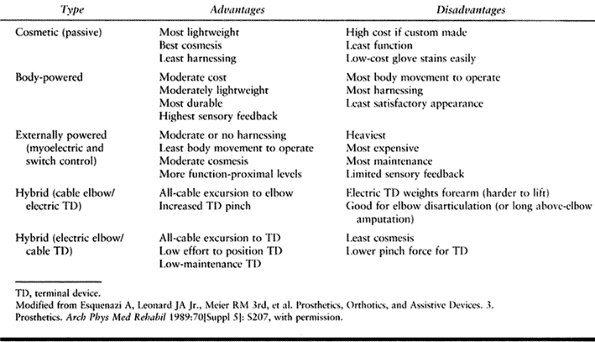
-
Passive, in which the position of the terminal device or more proximal components is changed with a contralateral hand
-
Body-powered, in which gross body movements activate cables for function
-
Myoelectric, which is battery-powered and computer-driven
-
Hybrid system, which is a combination of body-powered and myoelectric
 |
|
Table 122.5. Advantages and Disadvantages of Various Upper-limb Prostheses
|
want nearly life-like cosmesis or who have a high-level amputation and
want a lightweight arm for cosmetic reasons. Passive prostheses are
lightweight and nonfunctional. Cost depends largely on cosmetic finish.
Off-the-shelf cosmetic covers are relatively inexpensive, while nearly
life-like silicone covers are expensive.
controlled by gross body movements through a system of straps and a
harness that also doubles as a suspension aid. Stainless steel cables
are attached to the straps proximally and to parts of the terminal
device distally. If the amputation is proximal to the elbow joint, the
cable will go through an elbow flexion attachment first. Body
movements, such as a shoulder shrug or scapular abduction, put tension
on a cable, causing a response. A series of movements initiates
flexion, extension, and locking of the elbow, after which the terminal
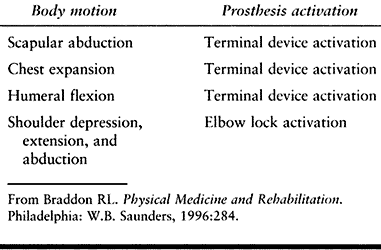
device can be activated (Table 122.6). If distal, the cables merely control the terminal
device. The body-powered prosthesis does not depend on a battery for
power, has a quicker component reaction time, and is less expensive
than the myoelectric. There is feedback from the cable, and it is more
durable and easier to maintain. Conversely, a body-powered prosthesis
is at risk for repetitive injury of the activating muscles and joints,
has limited pinch-force control for an involuntary terminal device, and
can cause irritation to the skin of the contralateral side from the
harness.
 |
|
Table 122.6. Body Control Motions Typically Used for Prosthesis Activation
|
voluntary muscle action via an electronic signal. The signal is picked
up and amplified by electrodes placed over the muscle fibers and then
downloaded to a computer to provide a specific function.
type of prosthesis, myoelectric testing is done, before the components
are chosen, to determine the maximum threshold available from the
muscles. A myoelectric prosthesis provides good cosmesis and does not
require a harness to be activated. It has increased range of motion and
avoids repetitive-movement injury; it also has increased anatomic
function and voluntary wrist rotation. To its disadvantage, a
myoelectric device has a slower response time and increased weight
distally, as well as higher maintenance. It is battery-dependent and
less durable and has a longer down time for repairs. In addition,
myoelectric devices are expensive, require longer training, and are
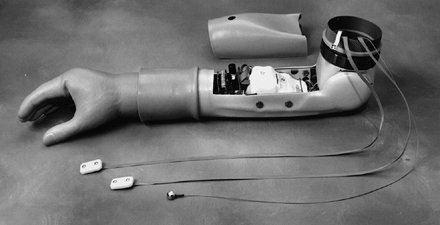
less adaptive and not waterproof (Fig. 122.15).
 |
|
Figure 122.15.
Myoelectric prosthesis with a hand attachment shows a battery and electrodes (no socket). (Courtesy of Liberty Technology, Hopkinton, MA.) |
myoelectric components, such as a body-powered elbow and a myoelectric
hand. This combination reduces the weight of the prosthesis and the
expense.
disarticulation and above- or below-elbow amputations. It is more
secure, provides greater proprioception, reduces harnessing, and
enables pronation and supination where anatomically possible. With
full-suction suspension, the prosthesis feels lighter. However, it is
more difficult to put on, especially for bilateral amputees, and
difficult to fit for short above- or below-elbow limbs. In addition, it
may be more expensive than other choices. A suction liner can be used
for above- and below-elbow prostheses. It is easier to put on than full
suction but may cause skin irritation. However, it is not as secure as
full suction and is more expensive.
for wrist disarticulation and below-elbow prostheses. It is easy to put
on and remove. Its disadvantages are that it can cause muscle atrophy
and prevents pronation and supination in below-elbow amputees (8).
prostheses. It is less expensive and more reliable than other
suspensions, and the only choice for a shoulder disarticulation or
forequarter amputation. The problem is that it is irritating to wear
and is less cosmetic.
considered in the choice of a terminal device. Hooks are lighter, have
less of a pendulum effect, and are less tiring to use. One option is to
use a hook for daily activities and to attach a hand whenever cosmesis
is more important. The passive device is nonfunctional and for cosmesis
only. Both the body-powered hook and body-powered hand are voluntary-
or involuntary-closing devices. The myoelectric hand is battery-powered
and computer-driven. It has specific adaptive equipment, such as for
sports, tools, and so forth.
myoelectric. Myoelectric devices can pronate and supinate and are
motor-driven. In elbow units, the main groups include passive,
body-powered, and myoelectric devices. In shoulder units, there is only
a manual unit.
 |
|
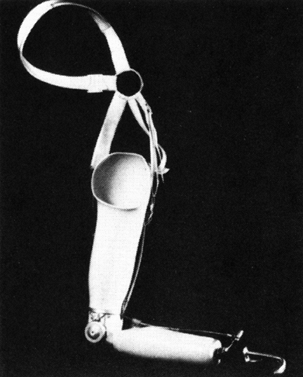
Figure 122.16. Typical body-powered prosthesis for a transhumeral amputee (harness not shown). (From D’Astous J, ed. Orthotics and Prosthetics Digest, Canada: Edahl Productions Ltd, 1981:153, with permission.)
|
 |
|
Figure 122.17. Typical body-powered prosthesis for a transradial level amputee.
|
maintain body symmetry, prevent flexion contractures, reduce surgical
edema, and prepare the residual limb for the prosthesis. Early fitting
of a prosthesis and promotion of two-handed function reduce the
rejection rate. Strengthening exercises help counteract the pendulum
effect of the terminal device. In addition, if myoelectric components
are used, patients may need exercises to improve their ability to
contract and cocontract the muscles chosen for the electrode site.
Computer programs are used to aid in training patients. Activities of
daily living must be taught before a patient becomes adept at doing
these tasks single-handedly; otherwise the prosthesis may feel
cumbersome.
necessary for success are not always available. Reimbursement issues
continue to present considerable problems for both prosthesis and
rehabilitation costs. In addition, a patient old enough to receive
Medicare cannot learn to walk in the limited physical therapy sessions
allowed for gait training at either outpatient or private physical
therapy facilities. The reimbursement allowed by some insurance
companies for one prosthesis per lifetime is not sufficient when the
patient is a child born with a limb deficiency. Often, less functional
components are used, purely on the basis of cost. In addition,
prosthetists have different levels of skills.
gradually accommodate amputees to their prosthesis and teach them how
to care for it and their skin will avoid most skin problems. The
residual limb and socket must be washed daily. Areas of split-thickness
skin graft do not tolerate pressure, particularly if over bony
prominences. They may eventually require revision if modification of
the socket is not successful in preventing problems. Painful bursas can
usually be managed by modifications of the socket, but occasionally
problematic bony prominences will require removal.
keeping the socket and skin as dry as possible, and, when necessary,
application of typical fungicides. Folliculitis usually results from
sweating, poor hygiene, and pistoning in the socket caused by a poor
fit. These problems usually respond to good skin care. If folliculitis
progresses to abscess, it may require incision and drainage, with
limited prosthesis use until healing occurs.
contact can lead to edema in the stump, which can lead to hemosiderin
deposition and the eventual development of verrucous hyperplasia. This
problem is preventable through good prosthetic fitting that achieves
total contact in the socket.
neuromas should initially be addressed with socket modifications. If
modifications are unsuccessful, then surgical intervention may be
required (see Chapter 120 and Chapter 121).
Nearly all adult amputees have an image and sensation of the amputated
part known as “phantom sensation,” which usually declines with time. On
occasion, this will be accompanied by pain in the phantom. Rule out any
prosthetic or surgical causes of pain, as these may aggravate phantom
pain. Referral to a pain management center for medicinal therapy,
transcutaneous electrical stimulation, lumbar sympathic blocks, and
other such interventions may be useful. Strong psychosocial support for
patients is important.
role of early rehabilitation and exercises to build strength and
prevent flexion contractures. Minor contractures of up to 10° can
usually be accommodated in the prosthesis and require no special
treatment. Hip and knee flexion contractures greater than 25° interfere
with prosthesis fitting and will result in an unfavorable posture and
gait pattern. Surgical release is sometimes necessary if these do not
respond to nonoperative treatment.
helpful for patients sustaining amputations in accepting their new body
image and adjusting to their new situation. Open discussion of their
problems and concerns in a group or mentor setting is helpful.
Information Center (toll-free: 1-888-AMP-KNOW) is a national
organization that is helpful for new amputees. This center has an
information hotline and can help find a local support group and peer
visitor, as well as providing appropriate pamphlets, magazines, and
videos and a list of certified prosthetists in their area.
in Prosthetics and Orthotics, Inc., today’s prosthetists must meet
certain educational and professional standards. These include a
bachelor’s degree and supervised internship, as well as passing a
national certification examination followed by mandatory continuing
education. As a result of constantly changing technology, better
outcomes can be realized when prosthetists have input into the
prescription request based on the initial prosthetic evaluation.
scheme: *, classic article; #, review article; !, basic research
article; and +, clinical results/outcome study.
FP, Glasser DB, Otis JC, et al. The Van Nes Tibial Rotationplasty: A
Functionally Viable Reconstructive Procedure in Children Who Have a
Tumor of the Distal End of the Femur. J Bone Joint Surg Am 1990:72:541.
LM, Engsberg JR, Tedford KG, Grimston SK. A Comparison of Oxygen
Consumption during Walking between Children with and without Below-knee
Amputations. Phys Ther 1994;74:943.
JM, Kroll MA, Rossbach PG. New Advances and Concepts in Amputee
Management after Treatment for Bone and Soft Tissue Sarcomas. Clin Orthop 1990;256:22.
JC, Lane JM, Kroll MA. Energy Cost during Gain in Osteosarcoma Patients
after Resection and Knee Replacement and after Above-the-knee
Amputation. J Bone Joint Surg Am 1985;67:606.
L, Powers CM, Guiterrez R, Perry J. Energy Expenditure during
Ambulation in Dysvascular and Traumatic Below-knee Amputation: A
Comparison of Five Prosthetic Feet. J Rehabil Res Dev 1995;32:111.
der Windt DA, Pieterson I, van der Eijken JW, et al. Energy Expenditure
during Walking in Subjects with Tibial Rotationplasty, Above-knee
Amputation, or Hip Disarticulation. Arch Phys Med Rehabil 1992;73:1174.
LJ, Chambers RB, Wagner FW Jr. Amputation Levels of Bilateral
Lower-extremity Amputees: Analysis of One Hundred and Three Cases. J Bone Joint Surg Am 1983;65:599.