
Editors: Frassica, Frank J.; Sponseller, Paul D.; Wilckens, John H.
Title: 5-Minute Orthopaedic Consult, 2nd Edition
Copyright ©2007 Lippincott Williams & Wilkins
> Table of Contents > Posteromedial Bow of the Tibia
Posteromedial Bow of the Tibia
Paul D. Sponseller MD
Description
-
Posteromedial bowing of the tibia is an angulation of the lower leg noticed at birth (Fig. 1).
-
The foot typically is in a calcaneovalgus position.
-
The angulation of leg is secondary to a deformity in the tibia.
-
In most children, the angle gradually corrects itself during growth.
-
The limb-length discrepancy persists and increases proportionately during growth.
Epidemiology
-
This condition is rare.
-
Noticed at birth
-
Occurs equally in males and females (1,2)
Risk Factors
No risk factors are known.
Genetics
No Mendelian pattern is known.
Etiology
-
Unknown, but thought to be secondary to intrauterine positioning
-
May also represent an inborn error in physeal growth
-
Unlikely to be the result of fracture because of the proportionate shortening that follows
Associated Conditions
No known associated conditions
 |
|
Fig. 1. Posteromedial bow of the tibia occurs just above the ankle of infants.
|
Signs and Symptoms
-
At birth, the ankle is dorsiflexed, and the foot is in the calcaneovalgus position.
-
An obvious bow is present in the distal part of the tibia posteromedially.
-
-
The condition is painless.
-
The condition is almost always unilateral.
History
No history of gestational abnormality or birth trauma
Physical Exam
-
Perform a complete examination of the lower extremity.
-
The leg appears shortened below the knee.
-
-
Measure the leg length bilaterally.
-
Measure the range of foot dorsiflexion, plantarflexion, inversion, and eversion.
-
The foot is calcaneovalgus.
-
Check for active function of all ankle muscles.
Tests
Lab
None is needed.
Imaging
-
Plain radiographs reveal the deformity.
-
Angulation of the tibia may be up to 60°.
-
Tibial bone may be normal or thickened.
-
No internal cystic change is seen.
Pathological Findings
-
All muscles, tendons, and tissues are within normal limits, although the anterolateral muscles are underdeveloped.
-
Only the bone is abnormal, with thickening and bowing.
Differential Diagnosis
-
Tibial fracture (3)
-
Fibular hemimelia
-
Calcaneovalgus foot (similar foot position)
-
Congenital pseudarthrosis and NF, which are associated with anterolateral bow
General Measures
-
This condition often resolves spontaneously with growth (Fig. 2), so initial treatment is watchful waiting.
-
Residual deformity may be up to 6–8° of angulation and limb length inequality of up to 5 cm at maturity.
-
Usually, it is much less.
-
-
Patients with a projected limb-length
inequality of >2 cm at skeletal maturity should be candidates for
epiphysiodesis or limb lengthening, depending on the degree of
discrepancy and their preference for a major versus minor procedure. -
Casting, bracing, and stretching provide no benefit in most cases (2).
-
In some extreme cases, a splint may be helpful in placing the foot flat to allow walking.
-
No activity restrictions are necessary.
-
A heel lift may benefit some patients with large limb-length inequalities.
Special Therapy
Physical Therapy
Physical therapy is not indicated.
Surgery
-
Epiphysiodesis of the contralateral tibial epiphysis is the most common procedure.
-
Performed near adolescence, long after the bow has straightened
-
-
Residual angulation of the tibia is sometimes problematic (5–10% of patients) (2).
-
Osteotomy of the tibia is used to correct the angulation.
-
Tibial lengthening procedures are used rarely.
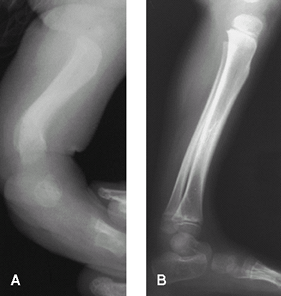 Fig. 2. Spontaneous resolution in a child. A: Lateral radiograph of 1-year-old patient. B: Lateral radiograph of same patient at 6 years of age.
Fig. 2. Spontaneous resolution in a child. A: Lateral radiograph of 1-year-old patient. B: Lateral radiograph of same patient at 6 years of age.
P.345
Prognosis
-
Prognosis is generally good.
-
No long-term sequelae occur as long as lengths are corrected.
Complications
-
Limb-length inequality:
-
The main complication
-
Thought to be secondary to damage to physis by asymmetric forces as a result of bowing
-
Is correctable by surgery
-
Patient Monitoring
-
Obtain radiographic measurements of limb lengths (scanogram) by age 5 years, so they can be plotted onto a growth curve.
-
Usually, growth inhibition remains proportionate.
-
Radiographic measurement allows for prediction of final discrepancy and determination of the need for future surgery.
References
1. Pappas AM. Congenital posteromedial bowing of the tibia and fibula. J Pediatr Orthop 1984;4: 525–531.
2. Schoenecker
PL, Rich MM. The lower extremity. Bowing of the tibia. In: Morrissy RT,
Weinstein SL, eds. Lovell and Winter’s Pediatric Orthopaedics, 6th ed
Philadelphia: Lippincott Williams & Wilkins, 2006:1189–1200.
PL, Rich MM. The lower extremity. Bowing of the tibia. In: Morrissy RT,
Weinstein SL, eds. Lovell and Winter’s Pediatric Orthopaedics, 6th ed
Philadelphia: Lippincott Williams & Wilkins, 2006:1189–1200.
3. Hofmann A, Wenger DR. Posteromedial bowing of the tibia. Progression of discrepancy in leg lengths. J Bone Joint Surg 1981;63A:384–388.
Codes
ICD9-CM
736.89 Posteromedial bowing of the tibia
Patient Teaching
-
Educate the family about the benign course of the disease.
-
Bowing should correct itself over the 1st few years.
-
Impress on the family that the patient
must be followed throughout growth to assess limb lengths, angulation,
and the need for surgery.
FAQ
Q: Could posteromedial bow be the result of a fracture in utero?
A:
No, because the discrepancy in length increases proportionately in
patients with posteromedial bow, whereas in patients with fracture, the
discrepancy decreases slightly because of the overgrowth phenomenon.
No, because the discrepancy in length increases proportionately in
patients with posteromedial bow, whereas in patients with fracture, the
discrepancy decreases slightly because of the overgrowth phenomenon.
Q: Is casting or bracing helpful in speeding resolution?
A:
No evidence suggests that it does. The only role for bracing is in
children who have such malposition of the foot that a brace improves
function.
No evidence suggests that it does. The only role for bracing is in
children who have such malposition of the foot that a brace improves
function.
Q: What percentage of children with posteromedial bow require surgery?
A:
More than 1/2 of children require epiphysiodesis near maturity for
leg-length equalization. Fewer than 1/4 require treatment of the
angulation.
More than 1/2 of children require epiphysiodesis near maturity for
leg-length equalization. Fewer than 1/4 require treatment of the
angulation.