
Editors: Chelly, Jacques E.
Title: Peripheral Nerve Blocks: A Color Atlas, 3rd Edition
Copyright ©2009 Lippincott Williams & Wilkins
> Table of Contents > Section VII – Pain Blocks > 69 – Myoneural Injections
69
Myoneural Injections
Nashaat N. Rizk
Albert J. Carvelli
Myofascial pain in muscle groups secondary to areas of ischemia in
those muscles as a result of reflex muscle and vascular spasm. This is
often secondary to prolonged imbalance in posture from chronic low back
pain.
The muscle attached proximally to the anterior border of the sacrum and
distally to the superior border of the greater trochanter of the femur.
Under fluoroscopy in the anteroposterior view, identify the greater
trochanter, the head of the femur, and the neck of the femur.
Quadratus lumborum injection:
The muscle is attached superiorly to the inferior border of the 12th
rib and inferiorly to the internal lip of the iliac crest. Under
fluoroscopy in the anteroposterior view, identify the iliac crest in
the lumbar back.
The muscle is attached superiorly to the inferior border of the 12th
rib and inferiorly to the internal lip of the iliac crest. Under
fluoroscopy in the anteroposterior view, identify the iliac crest in
the lumbar back.
Psoas muscle injection: The
proximal attachment is the sides of T12-L5 vertebrae, and the distal
attachment is the lesser trochanter of the femur. Under fluoroscopy in
the anteroposterior view, identify the L3 vertebral body and transverse
process.
proximal attachment is the sides of T12-L5 vertebrae, and the distal
attachment is the lesser trochanter of the femur. Under fluoroscopy in
the anteroposterior view, identify the L3 vertebral body and transverse
process.
Identify the landmarks as listed previously. Direct a 22-gauge spinal
needle just superior to the neck of the femur, medial to the greater
trochanter, and lateral to the head of the femur. The injection of 2 mL
Isovue-200 (Bracco Diagnostics, Princeton, NJ) dye shows the piriformis
muscle as a distinct band running in the direction of the sacrum to the
greater trochanter (Fig. 69-1). After negative aspiration for blood, the local anesthetic mixture is injected.
Quadratus lumborum injection:
After identification of the iliac crest in the lumbar back region,
insert a 22-gauge needle until it comes into contact with the superior
edge of the iliac crest. Walk the needle off the iliac crest until it
lies just superior and 1 cm deep to the
After identification of the iliac crest in the lumbar back region,
insert a 22-gauge needle until it comes into contact with the superior
edge of the iliac crest. Walk the needle off the iliac crest until it
lies just superior and 1 cm deep to the
P.448
bone (Fig. 69-2A).
Inject 1 to 2 mL Isovue-200 to rule out intravascular placement of the
needle. After negative aspiration for blood, the local anesthetic
mixture is injected.
 |
|
Figure 69-1. Piriformis injection.
|
Psoas muscle injection:
After identification of the L3 vertebral body and transverse process,
insert a 22-gauge needle so that the tip is just inferior and deep to
the transverse process at this level. Inject 2 mL of Isovue-200 to
reveal the muscle as it fans out from the vertebral body inferiorly and
laterally (Fig. 69-2B). After negative aspiration for blood, the local anesthetic mixture is injected.
After identification of the L3 vertebral body and transverse process,
insert a 22-gauge needle so that the tip is just inferior and deep to
the transverse process at this level. Inject 2 mL of Isovue-200 to
reveal the muscle as it fans out from the vertebral body inferiorly and
laterally (Fig. 69-2B). After negative aspiration for blood, the local anesthetic mixture is injected.
-
If the course of the muscle is not
delineated after injection of the dye, but rather appears blotchy, the
needle will need to be repositioned.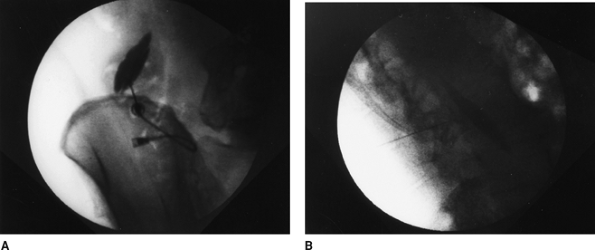 Figure 69-2. A: Quadratus lumborum injection. B: Psoas muscle injection.
Figure 69-2. A: Quadratus lumborum injection. B: Psoas muscle injection. -
Botox (Allergen, Irvine, CA) 25 to 100 U
can be injected after a successful diagnostic block is performed. The
dose depends on the intensity of the patient’s pain.
P.449
Suggested Reading
Sola AE, Bonica JJ. Myofascial pain syndromes. In: Loeser JD, ed. Bonica’s management of pain, 3rd ed. Philadelphia: Lippincott Williams & Wilkins, 2001.