
-
Inferior division of lumbar L4, L5 and sacral S1, S2, S3 nerves.
-
Emerges from the greater sciatic foramen.
-
Lies below the piriformis muscle (m.), deep to gluteus maximus m. on the posterior wall of the pelvis.
-
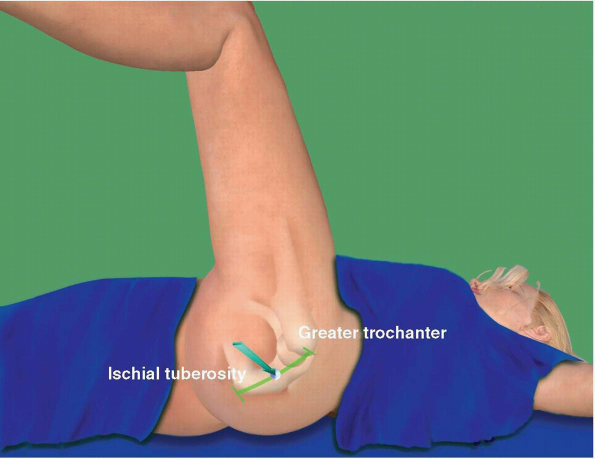
Descends between the greater trochanter of the femur and the ischial tuberosity.
-
Splits into the common peroneal and
tibial nerves. This division may take place at any point between the
sacral plexus and the lower third of the thigh. -
Articular branches arise from the upper part of the nerve and supply the hip joint.
|
|
|
|
|
|


|
|
|
|
|
|
|
|
|

|
|
|
|
|
|
|
|
|
|
|
|

 |
|
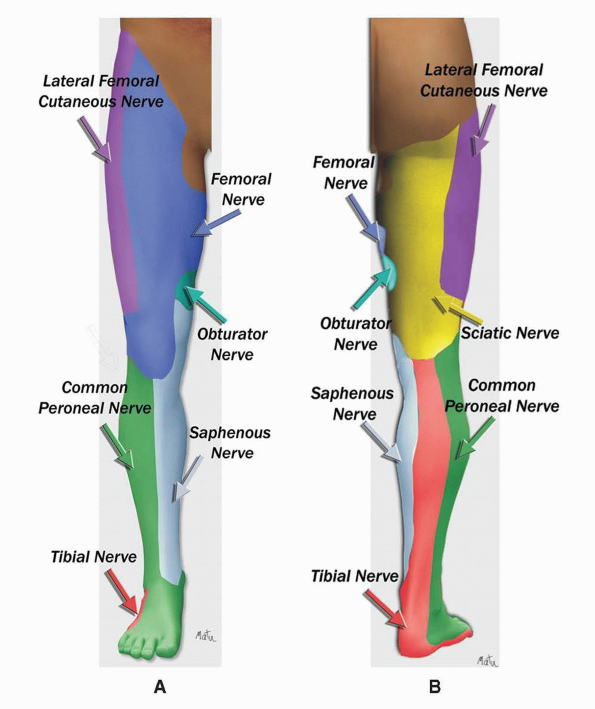
SCIATIC NERVE: DERMATOMES
|
-
Parasacral
-
Classic
-
Lithotomy (Raj’ approach)
-
Subgluteal
-
Lateral popliteal
-
High posterior popliteal
-
Classic posterior popliteal
-
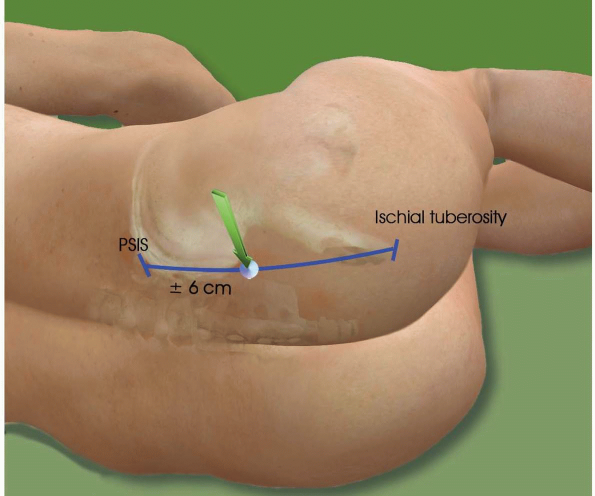
Line between the posterior superior iliac spine and the ischial tuberosity.
-
Insertion point is 6 to 7 cm caudal to the posterior superior iliac spine on this line.
-
Needle is introduced perpendicular to the skin or at a 30-degree angle in the cranial direction. Upon bone contact (deep landmark), the sciatic nerve is located 2 to 3 cm deeper. This bone contact corresponds to the medial part of the
P.57greater sciatic notch of the hip bone. The needle needs to be redirected either caudally or laterally or both.
-
A first muscle twitch occurs when the
needle is passing through the gluteus muscle. A second, deeper muscle
twitch occurs when passing through the piriformis muscle. The nerve is
located beneath the piriformis muscle at a depth of 6 to 9 cm. -
If the first distal twitch is a hamstring
contraction, deeper advancement of the needle will result in a tibial
nerve stimulation (60%) or a combined tibial and common peroneal
stimulation (18%). -
At this level, the sciatic nerve is close to internal iliac vessels (sciatic vascular trunk).
 |
|
PARASACRAL APPROACH
|
-
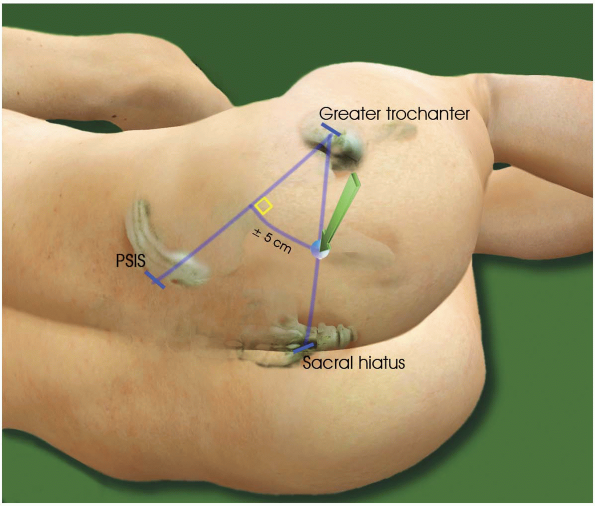
Line between the posterior superior iliac spine and the greater trochanter.
-
Perpendicular line is drawn at its midpoint.
-
Intersection with a line between the greater trochanter and the sacral hiatus. Or
-
5 cm on a perpendicular line drawn at the
midpoint of the line between the posterior superior iliac spine and the
greater trochanter.
-
4-inch needle.
-
Perpendicular to the skin.
-
The first contraction is elicited when
the needle passes through the gluteus maximus muscle; then a deeper
muscular contraction occurs when the needle passes through the
piriformis muscle. -
A tibial or peroneal neurostimulation is elicited 1 cm deeper.
-
Multistimulation: a dorsiflexion and
eversion of the foot (peroneal nerve) means that the needle is
stimulating the lateral part of the sciatic nerve.P.60A tibial n. stimulation will be elicited by moving the needle medially. -
Bone contact = lateral part of the
greater sciatic notch of the hip bone. The needle must be redirected
medially, caudally, or both.
 |
|
CLASSIC POSTERIOR APPROACH
|
-
Needle is introduced perpendicular to the skin.
-
Nerve is located at a depth of 5 to 7 cm.
-
Stimulation of the tibial or common peroneal nerve (hamstrings may be direct muscle stimulation).
 |
|
LITHOTOMY (RAJ’ APPROACH)
|
-
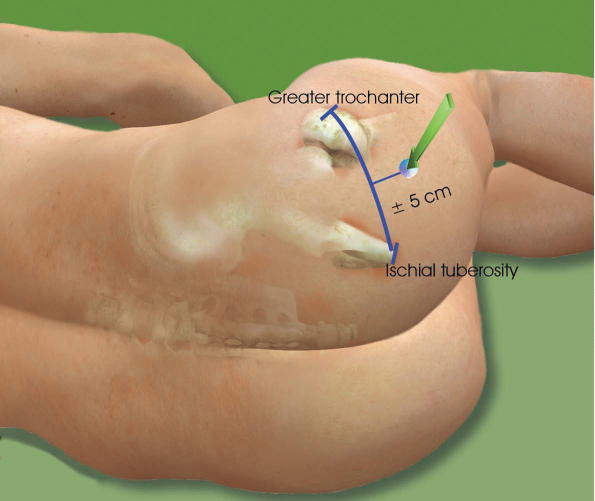
Line between the greater trochanter and ischial tuberosity.
-
5 to 6 cm caudate on a perpendicular line drawn from its midpoint.
-
Needle is introduced perpendicular to the skin.
-
Nerve is located at a depth of 4 to 6 cm.
-
Tibial nerve or common peroneal nerve is stimulated.
-
A catheter can be inserted for a continuous sciatic block.
 |
|
SUBGLUTEAL APPROACH
|
-
Great trochanter.
-
2 cm posterior and 2 cm caudal.
-
4-inch needle.
-
Needle contact with the lateral part of bone.
-
1 to 2 cm deeper.
-
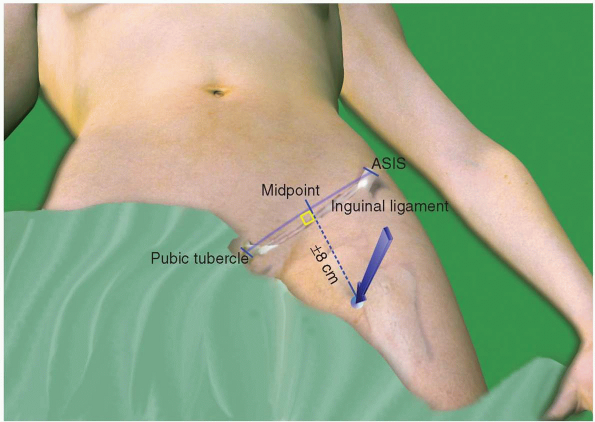
Line between anterior superior iliac spine (ASIS) and superior border of pubic tubercle.
-
8 cm caudate on a perpendicular line drawn from its midpoint.
-
4- to 6-inch needle.
-
Lateral to the femoral artery (has to be located).
-
Femoral nerve can be in the way.
-
Needle will contact the lesser trochanter
if approach is too proximal. The sciatic nerve runs lateral to the
lesser trochanter. To increase the probability of reaching the nerve,
internal rotation of the leg is necessary. -
4 cm below the lesser trochanter, the sciatic nerve runs more medial to the femur.
 |
|
PROXIMAL ANTERIOR APPROACH
|
-
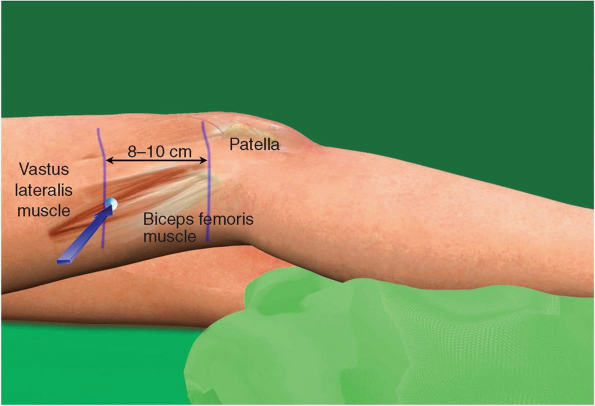
Groove between biceps femoris and vastus lateralis muscles (accentuated by asking patient to lift leg).
-
8 to 10 cm above the patella.
-
Sciatic division in tibial nerve and common peroneal nerve ranges from 4 to 13 cm above popliteal crease.
-
2- or 4-inch needle.
-
Needle insertion is perpendicular to the skin, then redirected at a 30-degree angle relative to the horizontal plan.
-
The sciatic nerve is deep to the biceps femoris muscle. The first twitch will be a contraction of this muscle.
-
A peroneal stimulation is elicited 2 to 3
cm deeper. Internal rotation of the leg may be needed to elicit tibial
nerve stimulation. -
When the groove cannot be located, look
for contact with the posterior part of the femur. The sciatic nerve is
located posteriorly and 1 to 2 cm deeper. -
A catheter can be inserted for a continuous sciatic block.
 |
|
LATERAL POPLITEAL APPROACH
|
-
Popliteal fossa crease.
-
Tendon of the biceps femoris muscle.
-
Tendon of the semitendinosus muscle.
-
Line along each of the two tendons.
-
Lateral border of the intersection of these two lines.
-
4-inch needle.
-
30- to 45-degree cranial direction.
-
Stimulation of tibial or common peroneal nerve at a depth of 6 to 8 cm.
-
A catheter can be inserted for a continuous sciatic block.
-
Tendon of the biceps femoris muscle.
-
Tendon of the semitendinosus muscle.
-
Perpendicular line to the midpopliteal fossa crease.
-
2-inch needle.
-
Perpendicular to the skin.
-
5 to 7 cm in the cephalad direction of the perpendicular line. Needle is inserted lateral to this point.
-
Tibial nerve stimulation.
-
Common peroneal nerve is 1 cm lateral to the tibial nerve.
 |
|
POSTERIOR POPLITEAL APPROACH
|
-
Ventral roots of the first 4 lumbar nerves.
-
Lumbar plexus lies within the psoas muscle, anterior to the transverse processes of the L2-L5 vertebrae.
|
|
|
|
|
|
|
|
|
|
|
|
 |
|
LUMBAR NERVES: DERMATOMES
|
-
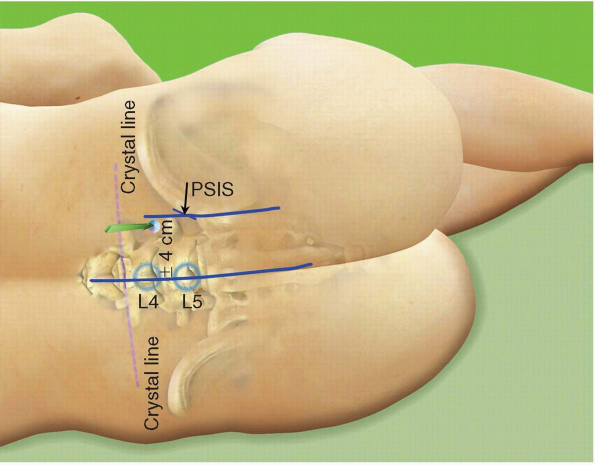
Highest point on iliac crest (HPIC).
-
Vertebral spine on the midline.
-
Posterior superior iliac spine (PSIS).
-
Line from the PSIS, parallel to the midline.
-
Line from the HPIC to the vertebral spine.
-
Puncture point can be at the intersection of these two lines or at 4 cm from the midline.
-
4-inch needle.
-
Perpendicular to the skin or slightly directed medially if puncture point at the intersection of the two lines.
-
After a contact with the transverse
process of L4 at 4 to 6 cm (deep landmark), walk the needle off the
transverse process cranially or caudally (angle between 30 and 45
degrees). -
The distance from the skin to the
transverse process depends on the patient’s size. The distance between
the transverse process and the plexus is never more than 2 cm. A stimulation of the femoral nerve inducing a contraction of the quadriceps should be elicited 1 or 2 cm deeper. -
Twitching of the hamstring muscles or
movement of the foot results from stimulation of a sciatic nerve root.
The needle is inserted too caudally and must be redirected to walk off
the transverse process cranially. -
A medial contraction of the thigh can be
related to an adductor muscle contraction by stimulation of the
obturator nerve. The needle must be redirected laterally in order to
induce a quadriceps contraction. -
A stimulation with a current intensity below 0.5 mA is not necessary (0.5 to 1 mA is adequate).
-
A catheter can be inserted for a continuous femoral block.
-
Blood pressure should be monitored closely because of a possible epidural or subarachnoid injection.
-
A test dose (3 to 5
mL) and a fragmented injection (10 mL/30 sec) of the mixture are
essential when a lumbar plexus block is being performed.
 |
|
POSTERIOR APPROACH (LUMBAR PLEXUS BLOCK)
|
-
Line between ASIS and pubic tubercle (PT).
-
Parallel line at the inguinal crease.
-
1 cm lateral to the femoral artery pulse.
-
If the femoral artery pulse cannot be felt, the puncture point will be approximately 1 cm lateral to a point located 5 cm caudally on a perpendicular line at the midpoint of the line ASIS-PT.
-
A contraction of the vastus medialis indicates a medial and anterior approach of the nerve.
-
To obtain a contraction of the vastus
intermedius (upward movement of the patella), the needle is directed
posterior and laterally. -
Single stimulation = the total dose of local anesthetic is injected when contraction of the vastus intermedius is elicited.
-
Multistimulation = injections of 5 to 7
mL local anesthetic, respectively, when a contraction of the vastus
medialis, vastus intermedius, and vastus lateralis is elicited. -
Distal pressure and large volume can procure a 3-in-1 block (the obturator nerve is missed most of the time).
-
For surgeries below the knee, a saphenous nerve block can be obtained when a vastus medialis contraction is elicited.
-
A catheter can be inserted for a continuous femoral block.
 |
|
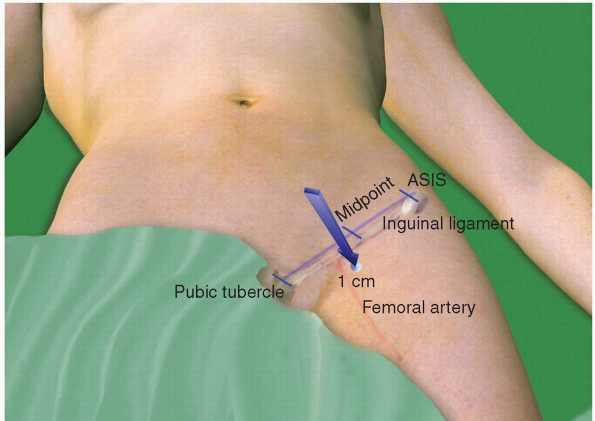
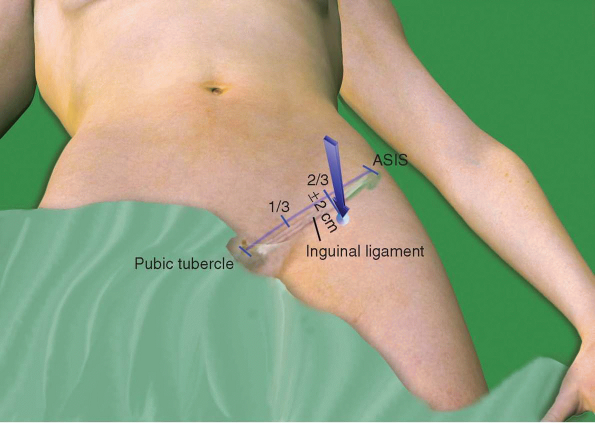
ANTERIOR APPROACH (FEMORAL BLOCK)
|
-
Line between ASIS and pubic tubercle.
-
Divide the line into three parts.
-
Insert needle 2 cm below this line at its lateral third.
-
Tuohy or B-bevel needle.
-
Perpendicular to the skin.
-
First “pop” and second pop occur when the
needle passes through the fascia lata and the fascia iliaca,
respectively (occasionally only one pop is obtained). -
A catheter can be inserted for a continuous femoral block.
 |
|
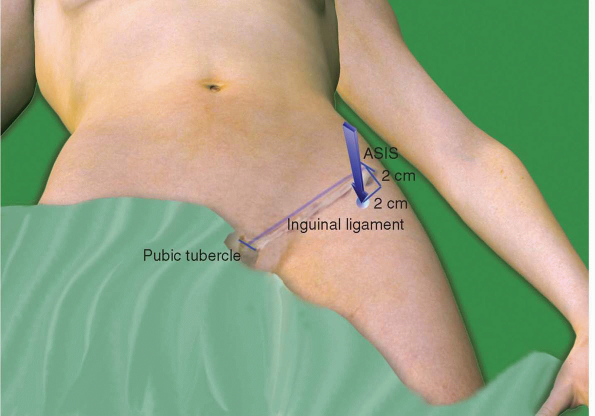
ANTERIOR APPROACH (FASCIA ILIACA APPROACH)
|
-
Pubic tubercle.
-
2 cm lateral and 2 cm caudal.
-
2-inch needle.
-
Insert perpendicular to the skin, then at a 30- to 40-degree angle in the cranial direction.
-
3- to 4-cm depth (obturator canal).
-
5 mL of local anesthetic.
-
Obturator nerve block is assessed by seeking for adductor muscle weakness.
-
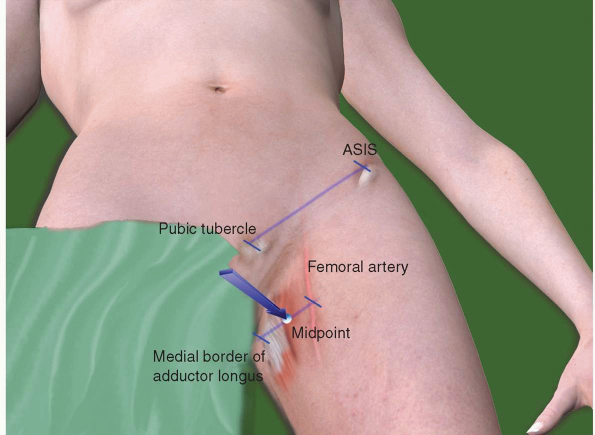
Line between ASIS and pubic tubercle.
-
Midpoint of a parallel line between femoral artery and medial border of adductor longus at inguinal crease.
-
Obturator n. is medial to the femoral
vein, below the pectineus m. and divides into anterior and posterior
branches, which straddle the adductor brevis muscle. -
2-inch needle.
-
30-degree angle in cranial direction.
-
5 mL of local anesthetic when a
contraction of the adductor brevis occurs and an additional 5 mL when a
contraction of the adductor longus (deeper) is elicited.
 |
|
OBTURATOR NERVE BLOCK (DISTAL APPROACH)
|
-
ASIS.
-
2 cm caudal and 2 cm medial.
-
Sensory nerve.
-
Paresthesia can be elicited using a 1-msec impulse.
 |
|
LATERAL FEMORAL CUTANEOUS NERVE BLOCK
|
-
Head of the tibia.
-
Femoral artery.
-
Sartorius muscle.
-
Sensory nerve.
-
Medial subcutaneous infiltration advancing deeper as the needle approaches the gastrocnemius muscle between the tibial tuberosity and the internal gastrocnemius muscle (3 cm deep).Or
-
Femoral neck block (stimulation of the vastus medialis m.).Or
-
Transsartorial approach: sartorius muscle above the medial side of the patella. The needle is inserted at a 45-degree angle posterior to the sartorius muscle.
-
Paresthesia can be elicited using a 1-msec impulse.
-
10 mL of local anesthetic.
-
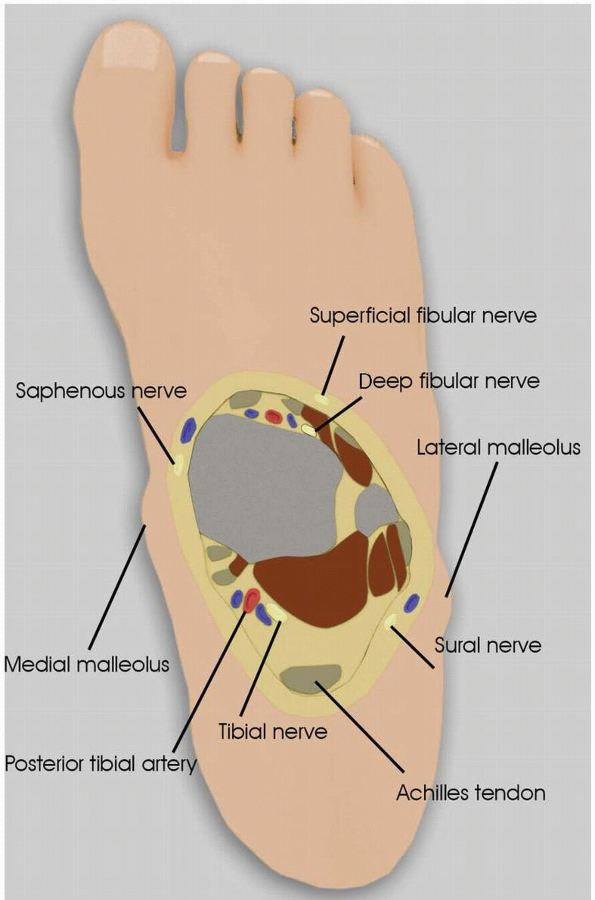
Posterior tibial artery.
-
Medial malleolus.
-
25-gauge or 1-inch needle for possible neurostimulation.
-
Injection of 5 mL of local anesthetic
posterior to the artery and anterior to the Achilles tendon at the
level of the medial malleolus. -
Neurostimulation = flexion of the toes.
-
No epinephrine.
-
Ankle joint.
-
Extensor hallucinis longus tendon.
-
Anterior tibial artery.
-
25-gauge needle.
-
Injection of 5 mL of local anesthetic
medial to the artery and lateral to the extensor hallucinis longus
tendon at the level of the ankle flexion crease. -
No epinephrine.
-
Achilles tendon.
-
Lateral malleolus.
-
Medial malleolus.
-
25-gauge needle.
-
Subcutaneous ring injection of 10 mL of
local anesthetic. One injection from the superior border of the lateral
malleolus to the lateral aspect of the Achilles tendon (sural nerve)
and one injection from the superior border of the lateral malleolus to
the posterosuperior aspect of the medial malleolus (superficial
peroneal nerve and saphenous nerve). -
No epinephrine.
 |
|
ANKLE BLOCK
|