
surgeon must have sharp and functioning instruments. The care,
maintenance, and ownership of surgical instruments and implants is, for
the most part, the province of the hospital and its operating room
staff. A few surgeons, particularly in highly specialized fields such
as microvascular surgery or arthroplasty, own their own surgical tools.
Surgeons might want to consider purchasing, maintaining, and using
their own instruments in the case of particularly delicate instruments,
those that are ineffective if damaged, and those that as a rule are not
in good condition in the average, busy operating room.
instruments, to be familiar with the instruments and implants, and to
inform the operating room staff well in advance if specialized or
backup instrumentation or implants are required for a particular
procedure. After the instruments are open on the back table, review the
steps of the surgery with the scrub nurse to be certain that all
instruments are present, in good shape, and functioning. Do this review
before the skin incision is made; do not delegate this responsibility.
first time, it is wise to go over the instrumentation at a time
separate from the first surgery. In hospitals that have motor skills
workshops, it may be worthwhile to go through a motor skills exercise
using the equipment.
grasp and manipulate large, tough structures such as tendons,
ligaments, and bone. Most forceps and clamps used in general surgery
are not designed to handle these structures and can be damaged if used
inappropriately.
regard to corrosion resistance and are designed more to meet functional
needs, such as cutting, wear resistance, and weight. After each use,
clean instruments thoroughly, usually with an ultrasonic cleaner. Some
must be disassembled for proper cleaning. After cleaning, dry them
thoroughly and store them properly to avoid corrosion.
surgical instruments that will spare problems for the surgeon, patient,
and instruments.
-
Never use microsurgical instruments for routine hand surgery.
-
Handle tendon, ligaments, periosteum, and
other soft tissues with toothed forceps, which provide a better grip,
crush less, and have a smaller surface area of contact than do
nontoothed forceps. The teeth of a large Kocher clamp provide such
advantages if you must firmly grip or pull a tendon or ligament. -
Do not use Kelly clamps, hemostats,
mosquitoes, or other similar instruments to grasp musculoskeletal
tissues. Using them in such a way springs the tines and makes them
useless for routine soft-tissue use. -
To suture tendons and ligaments, use a
heavy-duty needle holder with diamond-patterned jaws to grip the needle
firmly. Round needles are very difficult to pass through ligaments.
Instead, use a cutting needle unless you think the suture may cut out
of the tissue. -
The only instrument that should be used
for hammering is a mallet. In particular, do not use the handles of
power instruments, whose delicate machinery may be broken by any type
of pounding. -
Do not use dull or chipped osteotomes,
chisels, gouges, or periosteal elevators. It is particularly damaging
to sharp instruments to use them to remove hardware. Metal-to-metal
contact chips and dulls blades. Ask the operating room staff to set
aside a special set of older sharp instruments to be reserved for
hardware removal. -
Sharp, straight drill points are
essential to avoid bone necrosis and to obtain secure fixation. Because
drill points are difficult to resharpen correctly, replace them
frequently.
instruments belongs to the operating room staff. The surgeon can help
by being certain that the power tool is properly assembled and that it
is not used for anything other than its intended purpose.
assembly may damage power transfer interfaces. Know your power
instruments and make sure that the scrub nurse assembles them properly.
Excessive noise or overheating could be an indication of mechanical
problems or inadequate lubrication. Stop using the instrument
immediately; continued use may result in freezing of the components.
operation—lubricating the instrument—may result in its destruction,
requiring replacement or major overhaul. Care of these expensive,
sophisticated instruments cannot be casual. The operating room staff
must set up a mandatory maintenance program.
acetabulum to fine powered instruments for arthroscopy, are delicate
instruments. Most are gas powered; treat the hose carefully to avoid
gas leakage and loss of power. Do not sharply angulate, crimp, or
penetrate the hose. Use compressed air or nitrogen. Never use oxygen
because of the danger of fire.
as designated by the manufacturer. For most instruments, proper
pressure is approximately 6 bar (90 psi). Nevertheless, a central air
system should have the capacity to provide 9.6 to 12 bar (145 to 180
psi). It is best if power systems evacuate their gases out of the
operative field. The gas must be sterile, and sterility is usually
accomplished by means of a filter. If instruments are run by compressed
air from a central system, use of a filter may be necessary to
eliminate condensed water, dirt, or rust, which may interfere with the
function of the power equipment.
Most power instruments are damaged if immersed in water. After each
use, they must be wiped, thoroughly cleaned with an air jet, and
immediately oiled. See the manufacturer’s directions for maintenance.
 |
|
Figure 6.1.
Assorted power tools, including reciprocating and oscillating saws. The middle tool serves as a reamer or drill. A single power source is used. (Courtesy of Hall Surgical, Division of Zimmer, Santa Barbara, CA.) |
factory with high-quality surface finishes. Maintenance of the finish
is critical. Avoid scratching or nicking it to prevent the formation of
stress risers that can lead to premature implant failure. Store
implants in their original containers, and return them to their
containers if they are opened in the operating room. A second choice is
a properly designed storage rack that holds the implants securely, does
not scratch them, and prevents implants from rubbing against each
other. Never store implants loose and unprotected in a tray or drawer.
Significant scratches or nicks are justification for rejecting an
implant, particularly in the case of a prolonged implantation (e.g.,
total hip prostheses) or high-stress situations (e.g., plate fixation
of a nonunion). Never reuse implants that have been removed from
patients; they have been subjected to fatigue stress, and they may be
close to failure.
Discard screws used temporarily for external compression or other high-stress uses.
to minimize formation of stress risers. Avoid bending through screw
holes, and use templates so that bending of the plate is accomplished
with minimal manipulation. Excessive bending of a plate, particularly
reverse (back-and-forth) bending, increases its likelihood of failure.
The only implants that can be reused are unstressed ones—for example, a
screw that has been replaced because it is of incorrect length.
Although the designs appear identical, small differences often exist
that can cause mechanical or material incompatibility.
general instrument set is required for the incision and exposure of
soft tissues and for closure. Major orthopaedic operations usually
require a general surgery soft-tissue instrument set. A second set
contains orthopaedic instruments needed for most bone surgery, such as
periosteal elevators, chisels and osteotomes, gouges, mallets, drills
and drill points, rasps, forceps, rongeurs, and bone-holding
instruments. A third set contains some type of powered equipment for
drilling and cutting bone. A fourth set contains specialized
instruments for the procedure at hand. For fracture fixation, it
consists of internal fixation instruments and implants, and, in total
joint replacement, instruments for total joints. These specialized
instruments are discussed in separate chapters, with the surgical
procedures. General instruments are discussed in this chapter.
 |
|
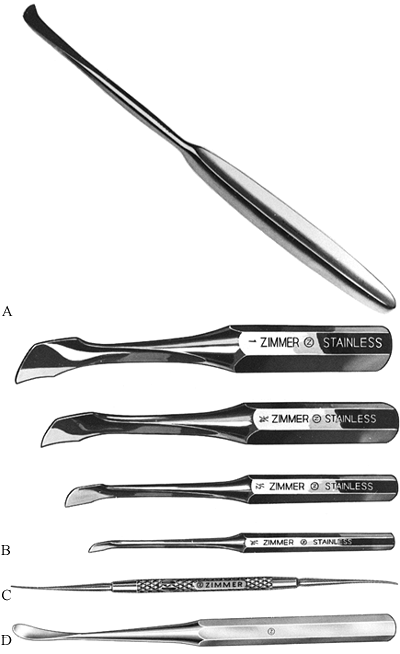
Figure 6.2. Periosteal elevators.
|
rounded tips that are designed to elevate periosteum and muscle fibers
from bone. Unless they are kept very sharp, they are ineffective in
cutting ligament and inserting tendon, for which a scalpel is more
useful. Use a periosteal elevator against the acute angle of muscle
fiber insertions. When used on the obtuse angle, it skids off into the
soft tissues. Examples include (A) the Langenbeck periosteal elevator, 8 in. (20 cm) long, and (B)
the Key periosteal elevator, which is available with blades from ¼ in.
(6.4 mm) to 1 in. (25 mm) wide. Handles are from 6¾ in. (171 mm) to 8¼
in. (210 mm) long. These are the most useful elevators for general bone
work, excluding the spine. The Freer septum elevator (C)
has both sharp and blunt blades available with a 7½-in. (191 mm)
handle. The Freer and Joseph elevators are useful in foot, hand, and
spine injury and in pediatric cases. Many styles of Cobb periosteal
elevators (D) are available. They are most
useful in spinal surgery. They have 11-in. (279 mm) handles in most
cases and have blades from ½ in. (13 mm) to 1¼ in. (32 mm) wide.
(Courtesy of Zimmer, Warsaw, IN.)
 |
|
Figure 6.3. Retractors.
|
the procedures that require them. Several useful retractors are
designed to bear against bone while atraumatically retracting the soft
tissues. Hohmann, cobra, and Bennett
retractors,
used singly or in combinations, are essential in most major long-bone
surgery and particularly surgery of the hip and pelvis. Small-tipped
retractors such as the Hohmann retractor are preferable because they
cause less stripping of the periosteum than other types do. The Hohmann
retractor (A) is available with blades from 11/16 in. (17 mm) to 111/16 in. (43 mm) and handles from 9¼ in. (235 mm) to 10¾ in. (273 mm). Aufranc cobra retractors (B)
have pointed, blunt, and blunt serrated tips. Overall lengths are
approximately 10 to 11 in. (25 to 28 cm). These are used widely for hip
surgery. Bennett retractors (C) are
available in two blade widths—¾ in. (44 mm) and 2½ in. (64 mm). They
are the most useful retractors in hip fracture repair and in major
long-bone surgery. The Blount retractor (D)
is designed to be used as a pair on either side of the bone. Length is
10¾ in. (273 mm). These are available with a single tine. (Courtesy of
Zimmer, Warsaw, IN.)
 |
|
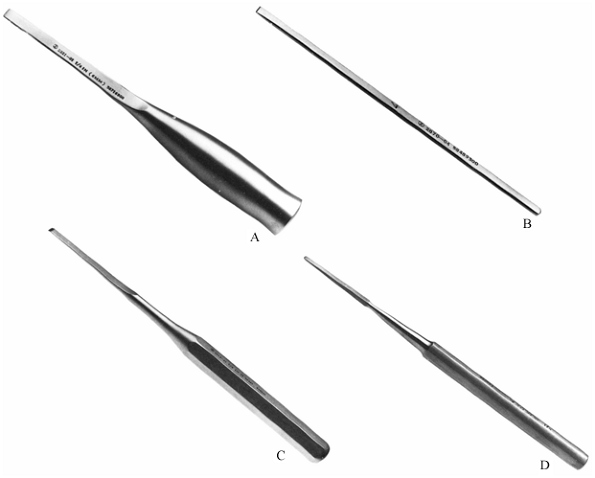
Figure 6.4. Chisels and osteotomes.
|
tools. Chisels have a cutting edge with a flat back parallel to the
long axis of the tool and a beveled edge; osteotomes are tapered on
both sides. These instruments are available in sets with widths varying
from 4.7 to 50 mm (3/16 to 2 in.). For general
orthopaedic use, these instruments should have large, knurled handles
that enable them to be grasped easily and that minimize fatigue of the
hand. They are designed to be used with mallets. Smaller varieties are
available for hand surgery, such as the Smith-Peterson osteotome (A).
Notice the double taper on the cutting edge. Overall length is 8 in.
(20 cm). These are available in ¼-in. to 1¼-in. widths, with straight
or curved blades. The Lambotte osteotome (B) has a length of 93/8 in. Straight and curved blades are available, and widths are ¼ to 1½ in. The Hibbs chisel (C) has a length of 9 in., may be
straight or curved, and comes with widths of ¼ to 1½ in. One side of the blade tip is straight. The Hoke osteotome (D) is 5½ in. long, is straight or curved, and comes in widths of 1/8 to ½ in.; it is useful for work on small bones. (Courtesy of Zimmer, Warsaw, IN.)
 |
|
Figure 6.5. Gouges.
|
curved from side to side and are designed to scoop bone away. They may
be straight or curved in the long axis. Gouges are used primarily to
harvest bone grafts and to prepare bone for the receipt of a bone
graft. Hibbs gouges (A) are available with
straight or curved blades in widths from ¼ in. (6.4 mm) to 1½ in. (38
mm). Handles are 9 in. (229 mm) long. Both the Hibbs and Smith-Petersen
gouges are excellent for most bone surgery. Cobb spinal gouges (B) have blades 5/16
in. (7.9 mm) wide and are 11 in. (279 mm) long. The blades available
are straight or curved with a medium, sharp, or reverse curve. These
gauges are especially designed for spinal surgery. (Courtesy of Zimmer,
Warsaw, IN.)
 |
|
Figure 6.6. Curets.
|
scrape or remove bone with a twisting action of the handle. The most
effective curets are fitted with large, long handles. The spoon sizes
range from 000 to 6. The Brun bone curet (A) has a hollow handle, but others (B)
may have solid handles. Curets have 6½-in. (165 mm) or 9-in. (229 mm)
handles and straight or curved oval cups from size 000 to 6. Curets
come in many forms, including Cobb curets. (Courtesy of Zimmer, Warsaw,
IN.)
 |
|
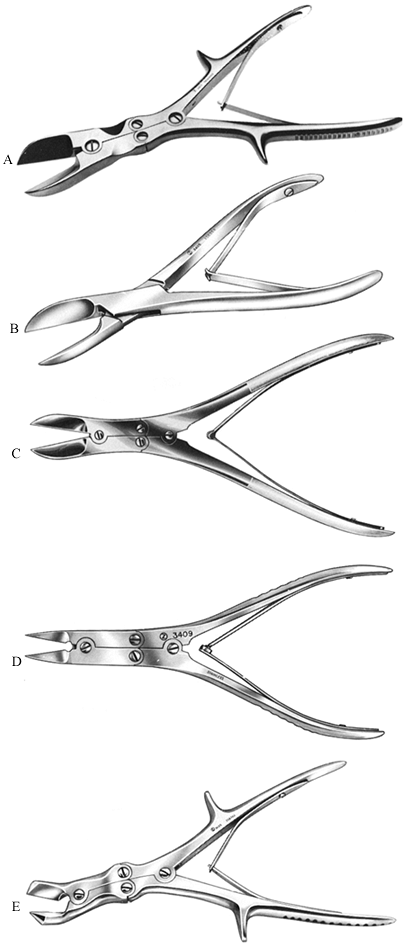
Figure 6.7. Bone-cutting forceps.
|
principles as wire cutters and are available in many sizes.
Single-action forceps are precise and useful for small or soft bone
work. Double-action forceps are required for most applications. Forceps
do not cut well near their tips and are most effective if the bone is
placed in the depths of the jaws. Stabilize both sides of the bone
while using forceps because sudden closure of the jaws could cause a
piece of bone to be ejected from the operating field. The Stille-Liston
bone-cutting forceps (A) is 10½ in. (267 mm) long; the blades are straight or curved. The Liston bone-cutting forceps (B) has straight blades with overall length from 5½ in. (140 mm) to 8½ in. (216 mm). Ruskin-Liston bone-cutting forceps (C) have straight and angled-up blades and an overall length of 7¼ in. (184 mm). Ruskin bone-splitting forceps (D) have a length of 7¼ in. (184 mm) and are available with delicate and standard jaws. Stille-Horsley rib forceps (E)
are 10½ in. (267 mm) long with bayonet jaws. They are designed to
transect ribs. All but the Liston forceps are double-action forceps,
which have better cutting power than single-action forceps but somewhat
less precision. (Courtesy of Zimmer, Warsaw, IN.)
 |
|
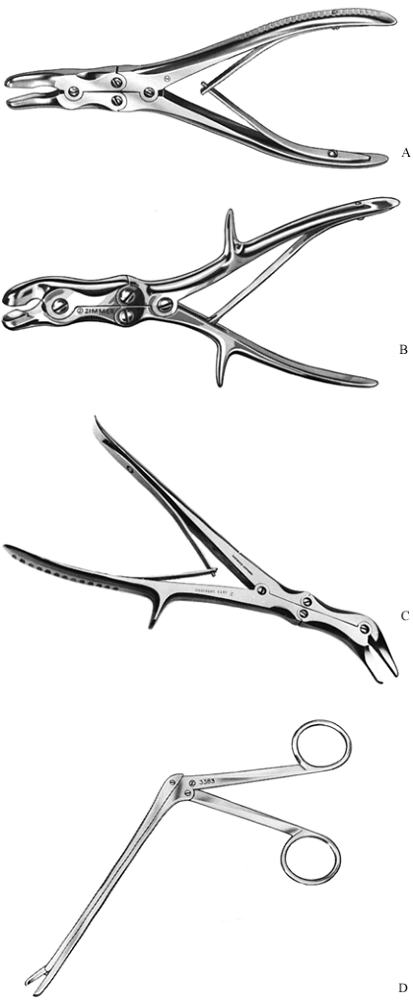
Figure 6.8. Rongeurs.
|
forceps, but the cutting end resembles a double set of opposed curets.
Use of rongeurs follows the same principles as the use of forceps. One
effective method of using a rongeur is to stabilize one cup against the
bone surface and cut or scrape with the other cup. Rongeurs are
available in 20 or more different designs. The bites are available in
oval, round, and other patterns. They can be used on bone and to remove
tough soft tissues such as fibrous scar. Many are specially designed
for spinal or neurosurgical applications. Four typical designs are
illustrated. Small, large, straight, and curved bites are available for
the Ruskin rongeur (A). Its length is 7¼ in. (184 mm). The Stille-Leur rongeur (B) has a 10-mm bite and straight or curved blades. Its lengths are 8½ in. (216 mm) and 10½ in. (267 mm).
The Echlin duckbill rongeur (C)
has a narrow, angular jaw in the plane of the handles. Bites of 2, 3,
and 4 × 10 mm can be taken. Its length is 9 in. (229 mm). The Cushing
rongeur (D) has a 5-in. (127 mm) shaft with 2 × 10-mm bite and straight or up- and down-angled jaws. (Courtesy of Zimmer, Warsaw, IN.)
 |
|
Figure 6.9. Bone rasp.
|
and shaping bone surfaces. Most effective are those resembling
woodworking tools. The fine patterns seen in metalworking tools fill so
rapidly with bone that they are less effective. The Putti bone rasp has
round and semiround ends or flat tapered and curved ends. Its overall
length is 11¾ in. (30 cm) or 10½ in. (27 cm). (Courtesy of Zimmer,
Warsaw, IN.)
 |
|
Figure 6.10. Mallet.
|
are not hammers. Most mallets are composed entirely of stainless steel
and are available in different sizes. Most surgeons feel that the
metal-to-metal contact of a steel mallet on a steel instrument provides
the best proprioceptive feedback. Shock-absorbing faces of plastic or
other materials are available, but their tendency to rebound makes them
less effective than all-metal ones. The orthopaedic bone mallet shown
here is all stainless steel. Its length is 7¾ in. (197 mm), and its
weight is 1 lb (454 g) or 2 lb (908 g). Mallets are also available in
aluminum with nylon or metal heads. Most surgeons prefer all metal.
(Courtesy of Zimmer, Warsaw, IN.)
 |
|
Figure 6.11. Bone-holding instruments.
|
manipulate bones. For major diaphyseal fractures, one of the most
useful bone holders is the Lowman bone-holding forceps (A).
It is particularly useful if there is a need to hold a plate against
the bone. Its disadvantage is that it requires considerable soft tissue
stripping to place. The Lowman bone clamp (A)
is available in three lengths [4¾ in. (121 mm) to 8 in. (203 mm)] and
three jaw sizes [3/4 in. (19 mm) to 1¼ in. (32 mm)]. It is calibrated
to measure the diameter of bone and can be disassembled to apply or
remove. In my hands, it is the most effective bone-holding clamp,
particularly for the femur and humerus. It holds plates to bone with
excellent security. In the Lane bone-holding forceps (B),
toothed jaws provide a firm grip on bone but are not ideal for holding
plates. A ratchet makes them self-retaining, an important feature.
Available in 13-in. (33 cm) and 17-in. (43 cm) lengths, they are useful
only for large bone surgery. The Kern bone-holding forceps are nearly
identical in appearance but are supplied in 6½ in. (165 mm) and 8½ in.
(216 mm) lengths for small bone work. In self-retaining bone-holding
forceps (C), the teeth are designed to grip bone. They are not to be used on plates. Verbrugge forceps (D), designed to hold plates on bone, have offset handles to facilitate placement. Tenaculum forceps (E)
resemble a stout towel clip. They are excellent for reducing and
holding small bone fragments, particularly in cancellous areas, and
they often are used in pairs. Tenaculums are much kinder to the soft
tissues. (A, B, C, E are courtesy of Zimmer, Warsaw, IN.)
 |
|
Figure 6.12. Bone drills.
|
tools because they require the use of two hands. Additionally, the
wobble introduced by the hand activating the drill handle produces a
less accurate drill hole than a power drill. Nevertheless, always keep
hand drills available in case the power drills fail. Hand drills are
more efficient to use than power drills for tasks such as inserting
traction pins. To run smoothly, drills must be cleaned and lubricated
frequently. The universal bone drill (A) is available in various combinations of 11-in. (279 mm) and 13-in. (330 mm) lengths and 5/32-in.
(4.0 mm) and ¼-in (6.4 mm) chucks. The drill uses a 2-to-1 gear ratio
and is cannulated for long pins and wires. A small hand drill (B) (Bunnell type), 5-in. long, cannulated, with a 5/32-in. chuck, is designed for small bone surgery. (Courtesy of Zimmer, Warsaw, IN.)
 |
|
Figure 6.13. Screwdrivers.
|
simple screwdrivers and automatic ones that retain the screw on the
screwdriver tip and release it automatically (trinkle drive). Screw
heads that require different screwdriver tips include single slot,
cruciate, Phillips, woodruff (i.e., cruciate with rounded teeth), torx
drive, and the hexagonal hole. The hexagon is used most commonly today,
but the torx provides more turning power and is less likely to slip,
particularly in titanium screws. Free bits for use in power drives are
available. Do not use power to drive screws into osteoporotic or
pathologic bone. Have the proper screwdriver available when removing
hardware implanted by others. Sometimes you can determine which one you
need by radiographic examination, but often you must
review the operative report. With an automatic screwdriver (A),
a grip holds the screw onto the bit. They are available with single
slot, cruciate, or universal bits. These screwdrivers have a unique
handle shape to increase grip power (B) and
have a hexagonal tip. The torx driver provides the best turning power
and is least likely to slip, particularly in titanium screws. (B is
courtesy of Zimmer, Warsaw, IN.)
 |
|
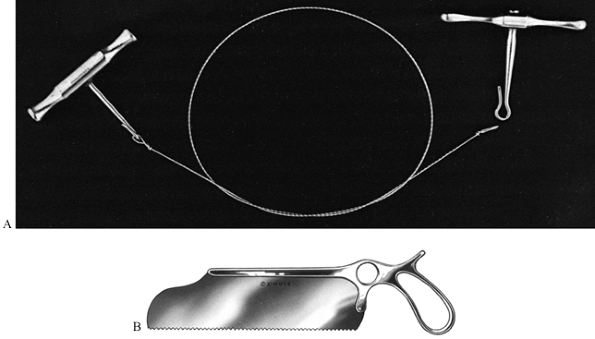
Figure 6.14. Hand bone saws.
|
are commonly used to transect bone when power tools are deemed
unnecessary or dangerous. They are useful for cutting away from vital
structures, such as the sciatic nerve in Salter’s innominate osteotomy.
To effectively use handles, keep the wire taut, and do not bend the
wire more than approximately 45°. The sharper the curve of the wire,
the more likely it is to jam. Protect the soft tissues with retractors.
The Gigli spiral saw (A) is available in 12-in. (305 mm) and 20-in. (508 mm) lengths with a pair of handles. The Satterlee bone saw (B) is used for amputations, but most surgeons have abandoned it in favor of power saws. (B is courtesy of Zimmer, Warsaw, IN.)
 |
|
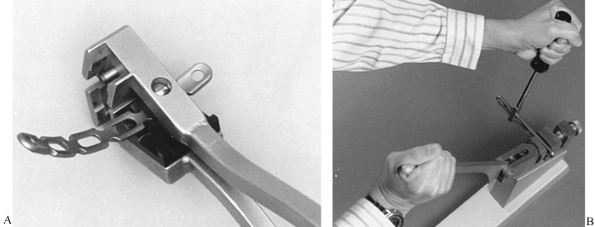
Figure 6.15. Plate benders.
|
 |
|
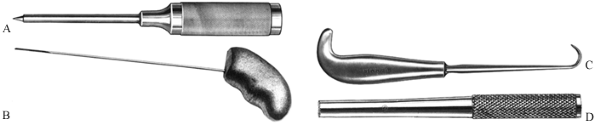
Figure 6.16. Miscellaneous instruments.
|
or desirable, as in a classic Bankart repair of the shoulder. Bone awls
are available with curved and straight tapered tips, like the Zuelzer
bone awl (A) and Rush rod awl-reamer (B) shown here. Bone hooks (C),
available in various sizes and shapes, are used to retract and
manipulate bone fragments. These are available in many sizes and
shapes. The inside diameter of the hooks range from 3/8 in. (9.5 mm) to 1 in. (25 mm). Bone tamps (D) are used to pack bone graft into place and to countersink wires. These are 6 in. (152 mm) long, with a 3/8-in. (9.5 mm) or ½-in. (13 mm) end diameter. (B—D are courtesy of Zimmer, Warsaw, IN.)