
Authors: Campbell, William W.
Title: Pocket Guide and Toolkit to DeJong’s Neurologic Examination, 1st Edition
Copyright ©2008 Lippincott Williams & Wilkins
> Table of Contents > Section G – The Reflexes > Chapter 31 – Associated Movements
Chapter 31
Associated Movements
An associated movement (AM)
is an unintentional, involuntary, spontaneous, automatic movement that
accompanies some other voluntary (or involuntary) movement. The
associated, or synkinetic, movement is often one that serves to fix a
part of the body as another part is voluntarily activated. Associated
movements often occur because of activation of the synergistic and
fixation muscles involved in a particular motion, or spread of the
activation to nearby motor neuron pools. This activity is normally
suppressed by the descending motor pathways, but in the face of disease
becomes clinically apparent. The corticospinal pathways are concerned
primarily with fine, fractionated, discrete movements of the distal
extremities. Disease in the corticospinal pathways may eliminate
discrete distal movement but not affect mass movements of the proximal
muscles. The mass movements usually play a secondary, supportive role,
particularly in fixation of the part to be moved. However, when the
distal movements are paralyzed, the primary movement left may be the
associated mass movement. Associated movements are, to a certain
extent, postural or righting reflexes that have a peculiarly widespread
distribution. They may be clinical homologues of movements seen in
decerebrate animals. Associated movements are more complex
manifestations of motor function than the simple reflexes, but are more
primitive than voluntary movements. They are probably initiated and
largely controlled by the extrapyramidal system and its connections,
although the corticospinal system also plays a role.
is an unintentional, involuntary, spontaneous, automatic movement that
accompanies some other voluntary (or involuntary) movement. The
associated, or synkinetic, movement is often one that serves to fix a
part of the body as another part is voluntarily activated. Associated
movements often occur because of activation of the synergistic and
fixation muscles involved in a particular motion, or spread of the
activation to nearby motor neuron pools. This activity is normally
suppressed by the descending motor pathways, but in the face of disease
becomes clinically apparent. The corticospinal pathways are concerned
primarily with fine, fractionated, discrete movements of the distal
extremities. Disease in the corticospinal pathways may eliminate
discrete distal movement but not affect mass movements of the proximal
muscles. The mass movements usually play a secondary, supportive role,
particularly in fixation of the part to be moved. However, when the
distal movements are paralyzed, the primary movement left may be the
associated mass movement. Associated movements are, to a certain
extent, postural or righting reflexes that have a peculiarly widespread
distribution. They may be clinical homologues of movements seen in
decerebrate animals. Associated movements are more complex
manifestations of motor function than the simple reflexes, but are more
primitive than voluntary movements. They are probably initiated and
largely controlled by the extrapyramidal system and its connections,
although the corticospinal system also plays a role.
PHYSIOLOGIC ASSOCIATED MOVEMENTS
Many AMs are present physiologically; in fact they play
a part in all normal motor activity. The activity of the antagonists,
synergists, and muscles of fixation in any motor response may be
considered AMs. Generally, the term is used for more widespread
responses. Common examples of normal AMs include the following:
pendular swinging of the arms when walking; facial contortions or
grimaces with violent exertion; movements of the head and neck with
movements of the eyes; and normal extension of the wrist with flexion
of the fingers. In some disease states, normal AMs may decrease or
disappear. The normal AMs are lost in diseases of the extrapyramidal
system, especially in the parkinsonian syndromes, where masking of
facial expression and absence of arm swing when walking are prominent
manifestations. In other conditions, normal AMs may be exaggerated, and
abnormal AMs may be present. With lesions of the corticospinal system,
a number of AMs may appear that are not present normally. Table 28.3
correlates the site of a lesion with the pattern of AMs. The AMs not
usually present in the normal individual are discussed in the following
paragraphs.
a part in all normal motor activity. The activity of the antagonists,
synergists, and muscles of fixation in any motor response may be
considered AMs. Generally, the term is used for more widespread
responses. Common examples of normal AMs include the following:
pendular swinging of the arms when walking; facial contortions or
grimaces with violent exertion; movements of the head and neck with
movements of the eyes; and normal extension of the wrist with flexion
of the fingers. In some disease states, normal AMs may decrease or
disappear. The normal AMs are lost in diseases of the extrapyramidal
system, especially in the parkinsonian syndromes, where masking of
facial expression and absence of arm swing when walking are prominent
manifestations. In other conditions, normal AMs may be exaggerated, and
abnormal AMs may be present. With lesions of the corticospinal system,
a number of AMs may appear that are not present normally. Table 28.3
correlates the site of a lesion with the pattern of AMs. The AMs not
usually present in the normal individual are discussed in the following
paragraphs.
P.282
PATHOLOGIC ASSOCIATED MOVEMENTS
Abnormal or pathologic AMs are usually activity in
paretic muscle groups that are brought out by active movement of other
groups, and seen predominantly in disease of the corticospinal
pathways. They usually accompany vigorous voluntary movements of
another part, and occur on the hemiplegic side. Associated movements
are slow, forceful movements of the already spastic parts that lead to
the adoption of new postures. The greater the spasticity, the greater
the extent and duration of the AMs.
paretic muscle groups that are brought out by active movement of other
groups, and seen predominantly in disease of the corticospinal
pathways. They usually accompany vigorous voluntary movements of
another part, and occur on the hemiplegic side. Associated movements
are slow, forceful movements of the already spastic parts that lead to
the adoption of new postures. The greater the spasticity, the greater
the extent and duration of the AMs.
Generalized Associated Movements
Generalized AMs occur in hemiplegia, where they tend to
emphasize or enhance the characteristic hemiplegic posture. The AMs
often occur with exertion. Straining and attempts to grip with the
paretic hand may cause an increase in the spasticity, with increased
flexion of the wrist, elbow, and shoulder; this is sometimes
accompanied by associated facial movements on the involved side. The
new posture may be maintained until the grip is relaxed. An
involuntary, automatic movement such as a yawn may cause the affected
arm to extend at the elbow, wrist, and fingers, remaining rigidly in
this new attitude until the yawn passes off. Movements such as coughing
or stretching may cause similar reactions. Tonic neck reflexes may also
influence these generalized AMs. Turning the head toward the hemiplegic
side may cause increased extensor tonus on that side, and turning it to
the normal side may be followed by either increased flexor tonus on the
paretic side or flexion of the arm and extension of the leg.
emphasize or enhance the characteristic hemiplegic posture. The AMs
often occur with exertion. Straining and attempts to grip with the
paretic hand may cause an increase in the spasticity, with increased
flexion of the wrist, elbow, and shoulder; this is sometimes
accompanied by associated facial movements on the involved side. The
new posture may be maintained until the grip is relaxed. An
involuntary, automatic movement such as a yawn may cause the affected
arm to extend at the elbow, wrist, and fingers, remaining rigidly in
this new attitude until the yawn passes off. Movements such as coughing
or stretching may cause similar reactions. Tonic neck reflexes may also
influence these generalized AMs. Turning the head toward the hemiplegic
side may cause increased extensor tonus on that side, and turning it to
the normal side may be followed by either increased flexor tonus on the
paretic side or flexion of the arm and extension of the leg.
Symmetric (Imitative or Contralateral) Associated Movements (Mirror Movements)
In the normal infant there is a tendency for movements
of one limb to be accompanied by similar involuntary movements of the
opposite limb; this disappears as coordination and muscle power are
acquired. Mirror movements usually disappear or become inconspicuous at
adolescence, their persistence to any marked degree should be
considered pathologic. They may occur in patients with brain injuries,
disturbances of cerebral development, and dysplasias of the upper
portion of the spinal cord; under such circumstances there are usually
associated abnormalities of motor function, tone, and reflexes.
Occasionally, persisting mirror movements are familial, and not
accompanied by other signs of neurologic disease.
of one limb to be accompanied by similar involuntary movements of the
opposite limb; this disappears as coordination and muscle power are
acquired. Mirror movements usually disappear or become inconspicuous at
adolescence, their persistence to any marked degree should be
considered pathologic. They may occur in patients with brain injuries,
disturbances of cerebral development, and dysplasias of the upper
portion of the spinal cord; under such circumstances there are usually
associated abnormalities of motor function, tone, and reflexes.
Occasionally, persisting mirror movements are familial, and not
accompanied by other signs of neurologic disease.
In certain neurologic disorders, forceful voluntary
movements of one limb may be accompanied by identical involuntary
movements of the same limb on the other side. They are usually seen in
the paretic limb when the opposite healthy one is forcefully moved,
although occasionally such movements may appear in the healthy limb on
extreme attempts to move the affected extremity (especially in
extrapyramidal disease). They appear particularly during exertion to
carry out a quick or strenuous movement. When squeezing the examiner’s
hand with the healthy hand, the paretic hand may flex. Any forceful
movement on the normal side may be followed by a similar but slow tonic
duplication of the movement on the paretic side. Imitation synkinesias
by themselves have little localizing significance, occurring with
lesions in various portions of the neuraxis. Their value in neurologic
assessment is in conjunction with other findings. Mirror movements may
occur on the unaffected or less affected side in early or mild
asymmetric parkinsonism.
movements of one limb may be accompanied by identical involuntary
movements of the same limb on the other side. They are usually seen in
the paretic limb when the opposite healthy one is forcefully moved,
although occasionally such movements may appear in the healthy limb on
extreme attempts to move the affected extremity (especially in
extrapyramidal disease). They appear particularly during exertion to
carry out a quick or strenuous movement. When squeezing the examiner’s
hand with the healthy hand, the paretic hand may flex. Any forceful
movement on the normal side may be followed by a similar but slow tonic
duplication of the movement on the paretic side. Imitation synkinesias
by themselves have little localizing significance, occurring with
lesions in various portions of the neuraxis. Their value in neurologic
assessment is in conjunction with other findings. Mirror movements may
occur on the unaffected or less affected side in early or mild
asymmetric parkinsonism.
Coordinated Associated Movements
Coordinated associated movements are involuntary
movements of synergistic muscle groups that accompany a voluntary
movement of a paretic limb. They are exaggerations or perversions of
ordinary synergistic and cooperative movements, and may be classified
into three groups: (a) movements, not present normally, which accompany
movements of a paretic limb; (b) contralateral
movements of synergistic muscle groups that accompany a voluntary
movement of a paretic limb. They are exaggerations or perversions of
ordinary synergistic and cooperative movements, and may be classified
into three groups: (a) movements, not present normally, which accompany
movements of a paretic limb; (b) contralateral
P.283
coordinated
associated movements; and (c) associated movements, normally present,
which are abolished in cerebral hemiplegia. These responses may be
useful in the differentiation between organic and nonorganic deficits.
 |
|
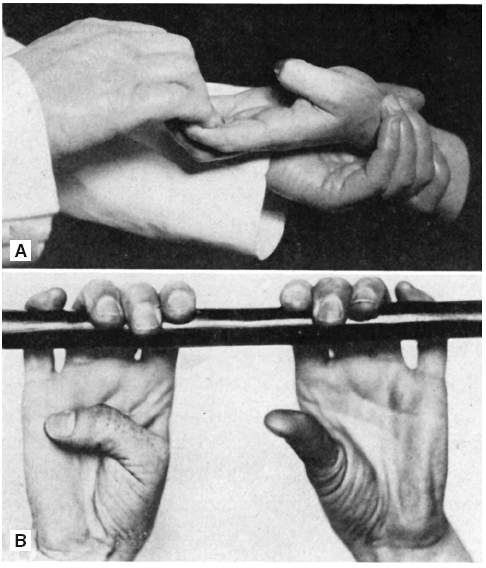
FIGURE 31.1 • Associated movement of thumb (Wartenberg sign). A.
Patient bends his last four fingers against resistance of four hooked fingers of examiner. Thumb moves toward palm. Mild spastic paralysis of hand. B. With his fingers hooked over a horizontally fastened rod, patient is asked to pull it down. Right thumb performs an associated movement toward the palm. Right-sided spastic hemiplegia. (From Wartenberg R. Diagnostic Tests in Neurology. Chicago: Year Book Medical Publishers, 1953.) |
Coordinated Associated Movements in the Paretic Limb
Coordinated AMs that accompany voluntary motion of
involved extremities in patients with hemiparesis are characterized by
a spread of movement from one muscle or group of muscles to others.
They alter the position of the part and lead to the adoption of new
postures. They do not appear in the normal individual or in nonorganic
weakness. The best known of these are the Wartenberg thumb adduction
sign, the Babinski trunk-thigh sign, and the tibialis sign of Strumpell.
involved extremities in patients with hemiparesis are characterized by
a spread of movement from one muscle or group of muscles to others.
They alter the position of the part and lead to the adoption of new
postures. They do not appear in the normal individual or in nonorganic
weakness. The best known of these are the Wartenberg thumb adduction
sign, the Babinski trunk-thigh sign, and the tibialis sign of Strumpell.
Wartenberg Sign
Active flexion of the terminal phalanges of the four
fingers of a paretic hand about a firm object, or against resistance
offered by the examiner’s fingers similarly flexed, is followed by
adduction, flexion, and opposition of the thumb (Figure 31.1).
In a normal extremity the thumb remains in abduction and extension. A
variation is for patient and examiner to hook and pull with only the
index fingers; the response is the same.
fingers of a paretic hand about a firm object, or against resistance
offered by the examiner’s fingers similarly flexed, is followed by
adduction, flexion, and opposition of the thumb (Figure 31.1).
In a normal extremity the thumb remains in abduction and extension. A
variation is for patient and examiner to hook and pull with only the
index fingers; the response is the same.
The Trunk-Thigh Sign of Babinski, or Combined Flexion of the Trunk and Thigh
The patient, lying supine with legs abducted, attempts
to sit up while holding the arms crossed on the chest. Normally, the
legs remain motionless and the heels down. In corticospinal
hemiparesis, the hip flexes as the trunk flexes and there is an
involuntary elevation of the paretic limb off the bed
to sit up while holding the arms crossed on the chest. Normally, the
legs remain motionless and the heels down. In corticospinal
hemiparesis, the hip flexes as the trunk flexes and there is an
involuntary elevation of the paretic limb off the bed
P.284
(Figure 31.2).
The toes may spread out in a fanlike fashion. The normal limb remains
on the bed or rises slightly, but not as high as the paretic one. In
paraparesis, both legs rise equally. In nonorganic weakness, the normal
leg rises and the paretic one does not, or neither leg rises. If the
patient tries to sit up with the legs hanging over the edge of the bed,
the hip flexes and the knee extends on the involved side. The same
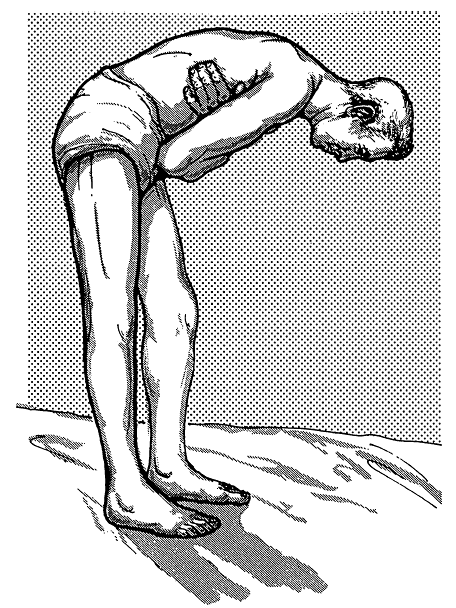
phenomenon occurs if the standing patient bends over (Figure 31.3).
 |
|
FIGURE 31.2 • Trunk-thigh sign in patient with left hemiparesis.
|
The Tibialis Sign of Strümpell
Normally, vigorous flexion of the hip and knee are
accompanied by plantarflexion of the foot. In lower-extremity weakness
due to a corticospinal tract lesion, voluntary flexion of the hip and
knee is accompanied by involuntary dorsiflexion and inversion of the
paretic foot; there may also be dorsiflexion of the great toe or of all
the toes. The patient is unable to flex the hip and knee without
dorsiflexing the foot (Figure 31.4). The response is accentuated if the movement is carried out against resistance.
accompanied by plantarflexion of the foot. In lower-extremity weakness
due to a corticospinal tract lesion, voluntary flexion of the hip and
knee is accompanied by involuntary dorsiflexion and inversion of the
paretic foot; there may also be dorsiflexion of the great toe or of all
the toes. The patient is unable to flex the hip and knee without
dorsiflexing the foot (Figure 31.4). The response is accentuated if the movement is carried out against resistance.
 |
|
FIGURE 31.3 • Combined flexion of the thigh and leg in a patient with left hemiparesis.
|
P.285
 |
|
FIGURE 31.4 • Tibialis sign in a patient with left hemiparesis.
|
Contralateral Coordinated Associated Movements
Coordinated AMs in which the response is contralateral
are similar to the symmetric AMs, but the response is not always
imitative and may involve muscles other than those used in the primary
movement.
are similar to the symmetric AMs, but the response is not always
imitative and may involve muscles other than those used in the primary
movement.
Loss of Coordinated Associated Movements
Certain coordinated AMs normally present are abolished
in pyramidal lesions. Normal associated and automatic movements, such
as swinging of the arms in walking and synergistic movements used in
rising and sitting down, are also lost in disorders of the
extrapyramidal system, especially parkinsonian syndromes. In upper
motor neuron facial weakness, the platysma may fail to contract as it
normally does when the patient opens the mouth as widely as possible,
grimaces, or touches the chin to the chest (platysma sign of Babinski).
in pyramidal lesions. Normal associated and automatic movements, such
as swinging of the arms in walking and synergistic movements used in
rising and sitting down, are also lost in disorders of the
extrapyramidal system, especially parkinsonian syndromes. In upper
motor neuron facial weakness, the platysma may fail to contract as it
normally does when the patient opens the mouth as widely as possible,
grimaces, or touches the chin to the chest (platysma sign of Babinski).