
Editors: Frassica, Frank J.; Sponseller, Paul D.; Wilckens, John H.
Title: 5-Minute Orthopaedic Consult, 2nd Edition
Copyright ©2007 Lippincott Williams & Wilkins
> Table of Contents > Femoral Shaft Fracture in the Child
Femoral Shaft Fracture in the Child
Paul D. Sponseller MD
Description
-
Femoral shaft fractures are defined as
those >5 cm below the lesser trochanter, but above the distal
metaphyseal (wider) portion of the lower femur. -
The location usually is specified as:
-
Proximal
-
Midshaft
-
Distal
-
-
Although the femur usually requires a
large amount of energy to fracture, fractures can occur with low
amounts of energy in infants and toddlers, and in those with a weak
area in the bone (1).
General Prevention
-
Appropriate supervision
-
Avoidance of contact sports if a substantial weakness of the bone or a known lesion in the femur is present
Epidemiology
-
Fractures of the femur are more common:
-
In areas of high population density or low socioeconomic level
-
In children 0–3 and 12–16 years old
-
Pathophysiology
-
Femur fractures may occur in different patterns, which are suggestive of, but do not prove, a particular mechanism (1).
-
“Buckle” fracture suggests direct impact.
-
Spiral fracture suggests twisting.
-
Transverse fracture suggests a hit from the side.
-
Comminuted (shattered) and/or open fracture suggests very high energy or weak bone.
-
-
Femur fractures in children usually are
followed by a 1.0–1.5 cm “overgrowth” during the 18 months after
healing, which accommodates some shortening during fracture treatment.
Etiology
-
The most common mechanisms by age are:
-
0–2 years old:
-
Nonaccidental injury (child abuse) in those <12 months old
-
Fall from a height
-
-
2–5 years old:
-
Fall from a height
-
Fall while playing
-
Pedestrian–motor vehicle accident
-
-
5–16 years old:
-
Bicycle
-
Pedestrian–motor vehicle accident
-
Motor vehicle occupant
-
Sports
-
-
Associated Conditions
-
Some underlying bone disorders:
-
OI
-
Bone cyst
-
Fibrous cortical defect or NOF
-
Cerebral palsy
-
Fibrous dysplasia
-
-
Other injuries that occur with femur fractures:
-
Head injury
-
Spine fracture
-
Upper extremity fracture
-
Signs and Symptoms
History
-
Patients should be asked about antecedent pain if a question of a pathologic lesion arises.
-
In cases of possible nonaccidental injury, caregivers or witnesses should be questioned about specifics of the event, including:
-
Child’s position before the injury
-
Mechanism of injury
-
What happened after the injury
-
Physical Exam
-
The thigh is swollen with a femur fracture.
-
If the fracture is displaced, it usually is shortened and externally rotated.
-
Any internal or external rotation motion of the lower extremity causes pain.
-
The knee may be swollen, even in the absence of a ligament injury.
-
Pulses and muscle function below the knee should be checked.
-
If nonaccidental injury is suspected, check for other bruises or tenderness, including fundus of the eye.
Tests
Imaging
-
Plain radiographs usually are sufficient.
-
MRI or CT scan may be needed if a nondisplaced or stress fracture is suspected.
-
If nonaccidental injury is suspected, a skeletal survey or bone scan may be necessary to rule out other injuries.
Diagnostic Procedures/Surgery
If a malignant lesion is suspected, a biopsy is indicated before surgical treatment, but this scenario is rare.
Pathological Findings
-
Thin cortices and bowing suggest OI.
-
Broad loss of cortical definition suggests fibrous dysplasia.
-
Focal lesions suggest unicameral cyst (centrally) or fibrous cortical defect (eccentrically)
-
Initial Stabilization
If the fracture is displaced and unstable, a Hare traction apparatus or a long splint should be used for comfort.
General Measures
Physical Therapy
-
Physical therapy is helpful in children >8–10 years old.
-
Younger children usually do well on their own.
-
Weightbearing depends on treatment and stage of healing, and should be prescribed by the orthopaedist.
Medication
-
Usually strong (narcotic) analgesics are needed in the early stages after fracture.
-
Pain usually is minimal after 2–3 weeks.
-
NSAIDs may slow healing.
Surgery
-
Many different options for treatment of a femoral shaft fracture (1–9):
-
Choice depends on patient age and fracture characteristics.
-
All options produce good results.
-
-
Immediate spica cast (3):
-
Best for children ≤6 years old, <32 kg
-
Leg(s) is immobilized in a cast that extends distally from just below the ribs.
-
Applied in the emergency department or operating room with the patient sedated or anesthetized
-
≤2.5 cm of shortening and 10–15° of angulation can be accepted because of remodeling and overgrowth.
-
Healing usually is complete by 6–8 weeks.
-
-
Traction (2–3 weeks) followed by spica cast (3):
-
Controls length and angulation well
-
Requires substantial hospital stay
-
No age limit
-
Not commonly used today because of desire for early mobilization
-
-
Flexible intramedullary nails (Fig. 1) (5,7):
-
Used mostly for children ~5–11 years old
-
Not for fractures near the proximal or distal ends or those with comminution
-
Sometimes no cast needed
-
Nail removal necessary at 3–6 months
-
-
External fixation (9):
-
Mostly for severe open fractures
-
Ages ~5–16 years
-
Slightly slower healing than that with nails (10–16 weeks) and, therefore, a higher risk of refracture
-
-
Plate fixation (2,8):
-
May be open or minimally invasive
-
Slight risk of plate failure
-
Usually used in comminuted or emergent situations
-
-
Rigid intramedullary nails (4,6):
-
Usually for children >10–11 years old
-
Avoid piriformis entry, which could cause AVN.
-
Allows early weightbearing
-
Subsequent nail removal recommended for young teens
-
P.131
-
Patients usually are seen every 4–8 weeks until healing.
-
Radiographs usually are needed.
-
No sports are allowed until the fracture is well healed.
-
Implant removal usually is required.
-
Follow-up may continue for 2 years to assess overgrowth.
-
Disposition
Issues for Referral
Physical therapy referral is needed if the patient is not progressing well or has special complications.
Prognosis
-
Most children have full return to function.
-
Concomitant internal knee ligament injury in a child <12 years old may produce long-term impairment.
-
Examine at time of stabilization and healing.
-
MRI if indicated
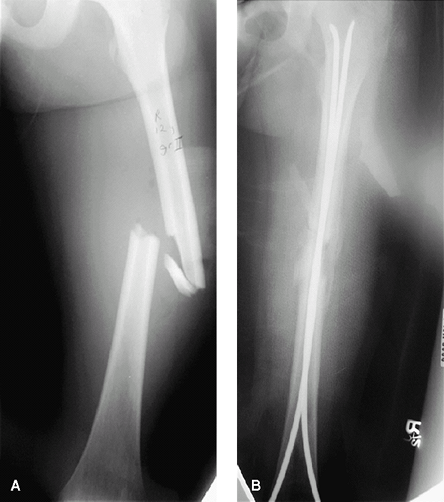 Fig. 1. Femur fracture in a 10-year-old (A) treated with flexible intramedullary nails (B).
Fig. 1. Femur fracture in a 10-year-old (A) treated with flexible intramedullary nails (B).
-
Complications
-
Nonunion:
-
Occurs in <1% of closed pediatric femur fractures (5–9)
-
Occurs in 10–20% of open fractures (5–9)
-
-
Malunion:
-
Up to 15–20° are acceptable proximally.
-
10° are acceptable distally.
-
Remodeling usually is good if the patient is <10 years old.
-
-
Shortening:
-
2.5–3 cm of shortening are acceptable if the patient is <10 years old.
-
Overgrowth compensates for up to 1.5 cm.
-
Contralateral epiphysiodesis is an option.
-
-
Neurovascular injury:
-
Most common with open fractures
-
Risk of femoral artery injury or compartment syndrome
-
-
Infection:
-
1% risk with operative treatment (5–9)
-
Risk is higher with open than with closed fractures.
-
-
AVN:
-
Risk with adult-type nails inserted through the piriformis fossa
-
Do not use in children <15 years old.
-
-
Ligament injury:
-
May coexist with fracture
-
Check for this injury when the fracture is stable.
-
Patient Monitoring
Neurovascular checks for the first 1–2 days
References
1. Pierce
MC, Bertocci GE, Janosky JE, et al. Femur fractures resulting from
stair falls among children: An injury plausibility model. Pediatrics 2005;115:1712–1722.
MC, Bertocci GE, Janosky JE, et al. Femur fractures resulting from
stair falls among children: An injury plausibility model. Pediatrics 2005;115:1712–1722.
2. Caird MS, Mueller KA, Puryear A, et al. Compression plating of pediatric femoral shaft fractures. J Pediatr Orthop 2003;23:448–452.
3. Epps HR, Molenaar E, O’Connor DP. Immediate single-leg spica cast for pediatric femoral diaphysis fractures. J Pediatr Orthop 2006;26:491–496.
4. Gordon
JE, Swenning TA, Burd TA, et al. Proximal femoral radiographic changes
after lateral transtrochanteric intramedullary nail placement in
children. J Bone Joint Surg 2003;85A:1295–1301.
JE, Swenning TA, Burd TA, et al. Proximal femoral radiographic changes
after lateral transtrochanteric intramedullary nail placement in
children. J Bone Joint Surg 2003;85A:1295–1301.
5. Ho CA, Skaggs DL, Tang CW, et al. Use of flexible intramedullary nails in pediatric femur fractures. J Pediatr Orthop 2006;26:497–504.
6. Kanellopoulos
AD, Yiannakopoulos CK, Soucacos PN. Closed, locked intramedullary
nailing of pediatric femoral shaft fractures through the tip of the
greater trochanter. J Trauma 2006;60:217–223.
AD, Yiannakopoulos CK, Soucacos PN. Closed, locked intramedullary
nailing of pediatric femoral shaft fractures through the tip of the
greater trochanter. J Trauma 2006;60:217–223.
7. Sink
EL, Gralla J, Repine M. Complications of pediatric femur fractures
treated with titanium elastic nails: A comparison of fracture types. J Pediatr Orthop 2005;25:577–580.
EL, Gralla J, Repine M. Complications of pediatric femur fractures
treated with titanium elastic nails: A comparison of fracture types. J Pediatr Orthop 2005;25:577–580.
8. Sink
EL, Hedequist D, Morgan SJ, et al. Results and technique of unstable
pediatric femoral fractures treated with submuscular bridge plating. J Pediatr Orthop 2006;26:177–181.
EL, Hedequist D, Morgan SJ, et al. Results and technique of unstable
pediatric femoral fractures treated with submuscular bridge plating. J Pediatr Orthop 2006;26:177–181.
9. Skaggs DL, Leet AI, Money MD, et al. Secondary fractures associated with external fixation in pediatric femur fractures. J Pediatr Orthop 1999;19:582–586.
Codes
ICD9-CM
821.01 Femur shaft fracture
Patient Teaching
-
Early in the treatment, it is helpful to
explain the concepts of remodeling and overgrowth to the parents, so
that they can understand when they see an acceptable alignment on their
child’s radiographs. -
Illustrative radiographs are helpful.
-
Parents of children treated in a spica cast require special teaching about hygiene and transportation.
Activity
Children may return to school as the environment allows.
Prevention
The management of motor vehicle traffic, as well as
appropriate intervention in instances of nonaccidental injury, may
prevent future injuries.
appropriate intervention in instances of nonaccidental injury, may
prevent future injuries.
FAQ
Q: Are there specific fracture patterns that prove nonaccidental injury?
A:
Not really. Only multiple unreported fractures in different stages of
healing, or metaphyseal “corner” fractures, are diagnostic.
Not really. Only multiple unreported fractures in different stages of
healing, or metaphyseal “corner” fractures, are diagnostic.
Q: Will a child who fractures a femur be able to return to sports?
A: Yes, barring complications, no sequelae should present.