
Editors: Frassica, Frank J.; Sponseller, Paul D.; Wilckens, John H.
Title: 5-Minute Orthopaedic Consult, 2nd Edition
Copyright ©2007 Lippincott Williams & Wilkins
> Table of Contents > Elbow Anatomy and Examination
Elbow Anatomy and Examination
Timothy S. Johnson MD
Constantine A. Demetracopoulos BS
Description
-
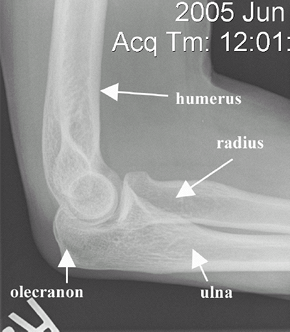
Bones (Figs. 1 and 2)
-
Ulnohumeral joint:
-
The trochlea of the humerus articulates with the trochlear notch of the proximal ulna.
-
The olecranon process of the ulna lies posterior to the joint.
-
Allows for elbow flexion and extension
-
-
Radiohumeral joint:
-
The capitulum of the humerus articulates with the radial head.
-
Allows for forearm supination and pronation
-
-
-
Ligaments:
-
UCL: Stabilizes the elbow medially
-
RCL: Stabilizes the elbow laterally
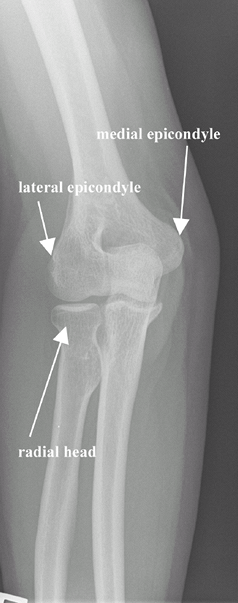 Fig. 1. AP radiograph of a normal elbow.
Fig. 1. AP radiograph of a normal elbow.
-
-
Muscles:
-
Biceps: Flexor and supinator
-
Brachialis: Flexor
-
Triceps brachii: Extensor
-
Pronator teres: Flexor and pronator
-
-
Nerves:
-
Median nerve:
-
Crosses the elbow anteriorly, superficial to the brachialis muscle, and medial to the brachial artery
-
Innervates the flexors of the forearm
-
-
Ulnar nerve:
-
Crosses the elbow superficially and posterior to the medial epicondyle in cubital tunnel
-
Innervates the intrinsic muscles of the hand
-
-
Radial nerve:
-
Crosses the elbow anteriorly to the lateral epicondyle
-
Innervates wrist, hand, and elbow extensors
-
-
Signs and Symptoms
Physical Exam
-
Initial assessment:
-
Assess completely the contralateral elbow for comparison.
-
Assess the neck, shoulder, and wrist.
-
Perform a complete neurovascular examination of the extremities.
-
-
Inspection:
-
Expose both upper extremities from the shoulder girdle to the hand, inspecting for asymmetry anteriorly and posteriorly.
-
The elbow-carrying angle should be 5–10° of valgus for males and 10–15° of valgus for females.
![]() Fig. 2. Lateral radiograph of a normal elbow.
Fig. 2. Lateral radiograph of a normal elbow.
-
-
Palpation:
-
Localize pain to an anatomic structure with digital palpation.
-
-
ROM and strength testing:
-
Compare active and passive ROM.
-
Flexion: 140–150°
-
Extension: 0–10° of hyperextension
-
Supination: 90°
-
Pronation: 80–90°
-
-
Activities of daily living require 30–130° of flexion, 50° of supination, 50° of pronation.
-
Test isometric strength, testing bilaterally
-
-
Elbow effusion:
-
Palpate elbow laterally in the center of
the anatomic triangle formed by the lateral epicondyle, radial head,
and tip of the olecranon. -
Effusion may indicate intra-articular abnormality and can be accompanied by loss of elbow extension.
-
-
Lateral epicondylitis (tennis elbow) (1):
-
Repetitive overuse of the wrist and finger extensors
-
Tenderness to palpation of lateral epicondyle
-
Resisted wrist extension test:
-
Test resisted dorsiflexion of the wrist with forearm in pronation.
-
Test is positive if it reproduces pain near the lateral epicondyle.
-
-
-
Medial epicondylitis (golfer’s elbow):
-
Resisted flexion/supination test:
-
Place the patient’s elbow in slight flexion and the forearm in full supination.
-
Test resisted wrist flexion and/or pronation against resistance.
-
The test is positive if pain is reproduced at the medial epicondyle.
-
-
-
Olecranon bursitis:
-
Bursa lies subcutaneous and posterior to the olecranon process.
-
Bursitis may be secondary to trauma, hemorrhage, sepsis, or a rheumatologic condition.
-
Effusion can present with or without erythema and may be tender to palpation over the tip of the olecranon.
-
-
Instability (2):
-
UCL insufficiency (valgus stress test):
-
Secure the wrist between the examiner’s forearm and trunk.
-
Flex the elbow to 30° and apply a valgus stress.
-
Palpate the UCL along its course from the medial epicondyle toward the proximal ulna during this maneuver.
-
Increased medial joint-space opening with loss of a firm endpoint suggests UCL insufficiency.
-
-
RCL insufficiency (posterolateral rotatory instability test) (3):
-
With the patient supine and the shoulder flexed overhead, externally rotate the humerus to stabilize it.
-
Grasp the forearm in full supination.
-
Starting with forearm supination and elbow extension, slowly flex the elbow while applying a slight valgus.
-
A positive test results in a palpable
clunk, a posterior prominence of the radial head, and an obvious dimple
in the skin proximal to the radial head as the elbow subluxates.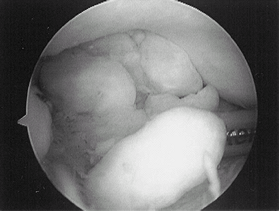 Fig. 3. Arthroscopic view of loose bodies in the posterior elbow.
Fig. 3. Arthroscopic view of loose bodies in the posterior elbow.
-
-
-
Valgus extension overload (2):
-
Overuse injury associated with a throwing athlete
-
Often associated with UCL insufficiency, intra-articular loose bodies, and radiocapitellar articular cartilage injury (Fig. 3)
-
Caused by posterior medial impingement of
ulnohumeral articulation and compression of radiocapitellar joint
during throwing motion -
Passive hyperextension of the elbow reproduces pain posteromedially.
-
-
Elbow arthritis:
-
Commonly presents with flexion contracture (incomplete passive and active extension) and pain at terminal extension
-
Can present with limitation in elbow flexion
-
Elbow effusion can be variable.
-
-
Cubital tunnel syndrome:
-
Created by compression of ulnar nerve at the elbow
-
Usually presents with pain
-
May be associated with numbness and paresthesias in distribution of the ulnar nerve
-
Symptoms worsen with prolonged elbow flexion
-
Positive Tinel sign: Tapping of the ulnar
nerve at the posterior aspect of lateral epicondyle reproduces
radicular pain and or paresthesia down the ulnar aspect of forearm/hand.
-
-
Distal biceps rupture:
-
Nonpalpable biceps tendon
-
Pain to palpation in the antecubital space
-
Popeye sign:
-
The biceps resembles a “Popeye” muscle when resisted elbow flexion is tested.
-
Note: The Popeye sign also occurs with proximal biceps tendon rupture.
-
-
P.111
References
1. Jobe FW, Ciccotti MG. Lateral and medial epicondylitis of the elbow. J Am Acad Orthop Surg 1994;2:1–8.
2. Chen FS, Rokito AS, Jobe FW. Medial elbow problems in the overhead-throwing athlete. J Am Acad Orthop Surg 2001;9:99–113.
3. Mehta JA, Bain GI. Posterolateral rotatory instability of the elbow. J Am Acad Orthop Surg 2004;12:405–415.
Additional Reading
Hoppenfeld S. Physical examination of the elbow. In: Physical Examination of the Spine & Extremities. Norwalk, CT: Appleton & Lange, 1976:35–57.
Hoppenfeld S, deBoer P. The elbow. In: Surgical Exposures in Orthopaedics: The Anatomical Approach, 3rd ed. Philadelphia: Lippincott Williams & Wilkins, 2003:105–139.
Morrey BF. Anatomy of the elbow joint. In: Morrey BF, ed. The Elbow and its Disorders, 2nd ed. Philadelphia: WB Saunders Co, 1993:16–52.
FAQ
Q: What are 3 common causes of atraumatic elbow pain?
A: Lateral epicondylitis, olecranon bursitis, and ulnar neuritis.