
Editors: Frassica, Frank J.; Sponseller, Paul D.; Wilckens, John H.
Title: 5-Minute Orthopaedic Consult, 2nd Edition
Copyright ©2007 Lippincott Williams & Wilkins
> Table of Contents > Subacromial Injection
Subacromial Injection
Timothy S. Johnson MD
-
Shoulder injection sites:
-
Subacromial area: Most common site
-
Other potential sites include:
-
Bicipital tendon sheath
-
Glenohumeral joint
-
Sternoclavicular joint
-
AC joint
-
-
-
To avoid confusion:
-
Always refer to these injections by describing the anatomic location of the shot.
-
Avoid describing any of these injections as a “shoulder injection.”
-
-
Subacromial injection is reserved for pain that has been resistant to NSAIDs, activity modification, and physical therapy.
-
The most common sources of pain include:
-
Subacromial bursitis
-
Shoulder impingement
-
Rotator cuff tendinitis
-
Partial-thickness rotator cuff tearsTable 1 Impingement Test
Result upon Re-examination Potential Explanations 100% Pain relief Rotator cuff disease: Subacromial bursitis, rotator cuff tendonitis, rotator cuff tear Partial pain relief Rotator cuff disease plus
another source of shoulder pain. Re-examine thoroughly to define and
treat the other source (e.g., cervical radiculitis, AC joint arthritis,
labral tear, etc.).No pain relief Rotator cuff disease in not
the source of pain. Re-examine thoroughly to define and treat the true
source (e.g., cervical radiculitis, biceps tendonitis, labral tear,
etc.).The medication did not go into the subacromial space.
-
-
Impingement test:
-
This test involves injection with local anesthetic only.
-
It is used to confirm subacromial disease/rotator cuff abnormality as the source of pain.
-
Because diagnosing shoulder abnormality
is difficult to master, shoulders are injected diagnostically more
often than any other joint. -
Although rotator cuff disease is probably
the most common shoulder ailment, the clinician should keep in mind
that many other causes of shoulder pain exist. -
Always re-examine the patient after the local anesthetic has taken effect.
-
If the subacromial space was injected correctly, the local anesthetic should alleviate the pain (Table 1).
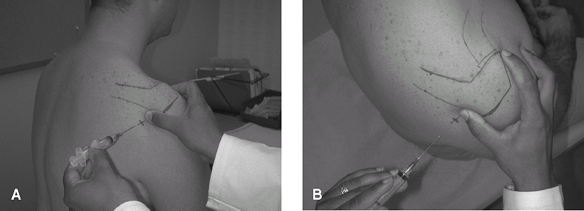 Fig. 1. Subacromial injection technique for the right shoulder. A: Posterior view. B: Superior view.
Fig. 1. Subacromial injection technique for the right shoulder. A: Posterior view. B: Superior view.
-
-
-
Therapeutic injection:
-
Repetitive corticosteroid injections into the subacromial space can lead to tendon rupture, atrophy, and retraction (1–3).
-
Always use a low dose (e.g., <10 mg of triamcinolone) of corticosteroid and re-examine the patient afterward (Table 1).
-
Inject local anesthetic with the corticosteroid.
-
Good pain relief shortly after the
injection (5 minutes, with recurrence of pain at a later date usually
bodes well for early surgical intervention; refer such patients for
surgical evaluation).
-
-
Chronic, massive, retracted rotator cuff tears with atrophy are not repairable surgically.
-
-
Several techniques are used for therapeutic injection of the shoulder, the easiest and most common of which follows (Fig. 1).
(Right shoulder injection is explained for demonstration purposes.
Switch hands when performing a left subacromial injection [2].)P.427-
Have the patient remove the shirt and expose the entire right shoulder girdle.
-
Identify bony landmarks of the shoulder; it may be helpful to mark the landmarks with a pen.
-
Acromion
-
Spine of the scapula
-
Greater tuberosity
-
Clavicle
-
AC joint
-
-
Perform a wide, standard sterile skin preparation of the posterior shoulder, and stand behind the patient.
-
The clinician should place the ulnar
border of the right thumb on the posterolateral border of the acromion
with the right index finger on the leading edge of the anterolateral
acromion. -
Insert the needle inferior to the
acromion (below the examiner’s right thumb), aiming anteriorly just
below the tip of the index finger.
-
References
1. Akpinar
S, Hersekli MA, Demirors H, et al. Effects of methylprednisolone and
betamethasone injections on the rotator cuff: An experimental study in
rats. Adv Ther 2002;19:194–201.
S, Hersekli MA, Demirors H, et al. Effects of methylprednisolone and
betamethasone injections on the rotator cuff: An experimental study in
rats. Adv Ther 2002;19:194–201.
2. Mathews PV, Glousman RE. Accuracy of subacromial injection: Anterolateral versus posterior approach. J Shoulder Elbow Surg 2005;14:145–148.
3. Scutt N, Rolf CG, Scutt A. Glucocorticoids inhibit tenocyte proliferation and tendon progenitor cell recruitment. J Orthop Res 2006;24:173–182.
Additional Reading
Ford LT, DeBender J. Tendon rupture after local steroid injection. South Med J 1979;72:827–830.
FAQ
Q: The subacromial injection is 1 of how many common locations injected in the shoulder?
A: 5: The subacromial bursa, bicipital tendon sheath, glenohumeral joint, sternoclavicular joint, and AC joint.
Q:
In addition to infection, what is 1 of the more common complications of
repetitive corticosteroid injection of the subacromial space?
In addition to infection, what is 1 of the more common complications of
repetitive corticosteroid injection of the subacromial space?
A: Rotator cuff rupture.