
Editors: Chelly, Jacques E.
Title: Peripheral Nerve Blocks: A Color Atlas, 3rd Edition
Copyright ©2009 Lippincott Williams & Wilkins
> Table of Contents > Section IV – Ultrasound > 34 – Ultrasound Guided Supraclavicular Block
34
Ultrasound Guided Supraclavicular Block
Paul Bigeleisen
Steve Orebaugh
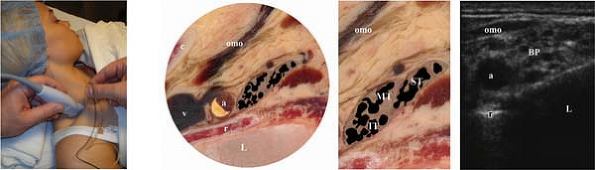
The subclavian artery is situated on top of the first rib. The plexus
lies posterosuperior to the subclavian artery. The anterior scalene
muscle is found anterior to the brachial plexus and subclavian artery.
The subclavian vein lies anterior to the anterior scalene muscle. The
pleura is immediately deep to the first rib (Fig. 34-1).
The plexus at this level appears to be a “cluster of grapes,” made up
of small fascicles. The superior, middle, and inferior trunks may be
contained in separate fascial compartments or lie within a single
epineurial compartment.
Sterile skin preparation, followed by application of a sterile probe
cover or sterilization of the transducer. Sterile sonographic gel
should be placed on the skin. After the optimum probe position is
obtained, local anesthetic is injected subcutaneously at the anterior
margin of the transducer. The block needle is inserted in-plane (along
the long axis of the transducer), aiming toward the brachial plexus as
imaged on the ultrasound unit screen. Whenever possible, the needle tip
should be placed immediately superior to the first rib between the rib
and the inferior trunk. This will ensure that the inferior trunk is
well anesthetized. The peripheral nerve stimulator should be switched
on at 0.4 to 1 mA to confirm the needle is in close proximity to the
plexus. When motor
P.281
stimulation
of the upper extremity is obtained, or sensory paresthesia of the
shoulder, arm, forearm, or hand is sensed by the patient, the
stimulator can be switched off. At this point, local anesthetic is
injected in small increments below the inferior trunk, with attention
to avoiding pain or paresthesias, and the syringe is aspirated for
intravascular position. The needle should then be repositioned to
ensure that local anesthesia is injected around the middle and superior
trunks. Distension of the tissues by local anesthetic, as evidenced on
the ultrasound unit screen, should occur with each injection, as
confirmation that the needle tip is not intravascular.
 |
|
Figure 34-1.
a, subclavian artery; c, clavicle; IT, inferior trunk; L, lung; MT, middle trunk; omo, omohyoid muscle; r, first rib; ST, superior trunk; v, subclavian vein. |
-
The needle tip must be kept in full view to avoid inadvertent insertion beyond the first rib, possibly causing a pneumothorax.
-
The in-plane approach can also be carried out from the posterior margin of the transducer. The same safety precautions apply.
-
Before inserting the needle through the
skin, depress the tip against the skin and indent it, looking for this
motion on the ultrasound screen. This confirms the orientation of
needle and probe. -
Unlike the situation at the level of
interscalene block, the entire plexus is compactly arranged at this
level. Thus, stimulation may result in motor (or sensory) excitement at
any portion of the upper extremity. -
Use of a tourniquet or surgery on the
medial aspect of the arm may necessitate a separate block of the
intercostobrachial nerve in the axilla.
Suggested Readings
Chan VWS, Perlas A, Rawson R, et al. Ultrasound-guided supraclavicular brachial plexus block. Anesth Analg 2003;97:1514–1517.
Gruber H, Kovacs P. Sonographic anatomy of the peripheral nervous system. In: Peer S, Bodner G, eds. High resolution sonography of the peripheral nervous system. Berlin: Springer-Verlag, 2003:13–36.
Perlas A, Chan VWS, Simons M. Brachial plexus examination and localization using ultrasound and electrical stimulation. Anesthesiology 2003;99:429–435.
Williams
S, Chouinard P, Arcand G, et al. Ultrasound guidance speeds execution
and improves the quality of supraclavicular block. Anesth Analg 2003;97:1518–1523.
S, Chouinard P, Arcand G, et al. Ultrasound guidance speeds execution
and improves the quality of supraclavicular block. Anesth Analg 2003;97:1518–1523.