
Editors: Berry, Daniel J.; Steinmann, Scott P.
Title: Adult Reconstruction, 1st Edition
Copyright ©2007 Lippincott Williams & Wilkins
> Table of Contents > Section
IV – Elbow Reconstruction > Part C – Operative Treatment Methods
> 57 – Surgical Exposures of the Elbow
IV – Elbow Reconstruction > Part C – Operative Treatment Methods
> 57 – Surgical Exposures of the Elbow
57
Surgical Exposures of the Elbow
Joaquin Sanchez-Sotelo
Adequate surgical exposure of the elbow joint is one of
the most critical factors in achieving a successful outcome in both
trauma and reconstruction. Elbow exposure is complicated by the need to
identify and protect surrounding neurovascular structures, some of
which are extremely close to the joint capsule. Various surgical
exposures have been developed to mobilize the extensor mechanism or to
allow access from the medial or lateral side of the joint while
preserving the collateral ligaments; anterior exposures are seldom used
for very specific indications (such as distal biceps tendon repair).
The skin incision will be determined by the selected deep exposure as
well as prior surgical skin incisions, but many elbow surgeons favor a
universal posterior midline skin incision that allows almost
circumferential exposure of the elbow joint. It is not the purpose of
this chapter to discuss all the approaches to the elbow joint but
rather to provide a summary of the approaches more commonly used by
elbow surgeons at the present time.
the most critical factors in achieving a successful outcome in both
trauma and reconstruction. Elbow exposure is complicated by the need to
identify and protect surrounding neurovascular structures, some of
which are extremely close to the joint capsule. Various surgical
exposures have been developed to mobilize the extensor mechanism or to
allow access from the medial or lateral side of the joint while
preserving the collateral ligaments; anterior exposures are seldom used
for very specific indications (such as distal biceps tendon repair).
The skin incision will be determined by the selected deep exposure as
well as prior surgical skin incisions, but many elbow surgeons favor a
universal posterior midline skin incision that allows almost
circumferential exposure of the elbow joint. It is not the purpose of
this chapter to discuss all the approaches to the elbow joint but
rather to provide a summary of the approaches more commonly used by
elbow surgeons at the present time.
Skin
Posterior Midline Skin Incision
Many elbow surgeons favor the use of a posterior midline
skin incision for many elbow procedures. It has several advantages: (i)
medial and/or lateral skin flaps can be elevated on demand to provide
access to virtually any deep exposure, (ii) the risk of neuromas is
minimized, as the number and diameter of nerve fibers crossing the
posterior aspect of the elbow are low compared to the medial or lateral
side, and (iii) should future surgery be needed, the same skin incision
can be used for almost any procedure. Exposures that involve
mobilization of the extensor mechanism are performed through this
incision. It is also extremely useful for the treatment of elbow
fracture-dislocations, which may require sequential access to both the
medial and lateral side of the joint depending on the pathology found.
skin incision for many elbow procedures. It has several advantages: (i)
medial and/or lateral skin flaps can be elevated on demand to provide
access to virtually any deep exposure, (ii) the risk of neuromas is
minimized, as the number and diameter of nerve fibers crossing the
posterior aspect of the elbow are low compared to the medial or lateral
side, and (iii) should future surgery be needed, the same skin incision
can be used for almost any procedure. Exposures that involve
mobilization of the extensor mechanism are performed through this
incision. It is also extremely useful for the treatment of elbow
fracture-dislocations, which may require sequential access to both the
medial and lateral side of the joint depending on the pathology found.
Wound-related complications are relatively uncommon
provided full-thickness fasciocutaneous flaps are elevated; seromas or
hematomas do happen occasionally, but they seldom compromise the
outcome. The posterior midline skin incision is placed slightly off the
tip of the olecranon either medially or laterally to facilitate
healing. When the elbow needs to be splinted, the splint can be placed
anteriorly to avoid direct pressure on the wound, and the elbow can be
immobilized in extension and kept elevated to decrease swelling and
surgical wound tension, as well as seroma or hematoma accumulation
underneath the skin flaps.
provided full-thickness fasciocutaneous flaps are elevated; seromas or
hematomas do happen occasionally, but they seldom compromise the
outcome. The posterior midline skin incision is placed slightly off the
tip of the olecranon either medially or laterally to facilitate
healing. When the elbow needs to be splinted, the splint can be placed
anteriorly to avoid direct pressure on the wound, and the elbow can be
immobilized in extension and kept elevated to decrease swelling and
surgical wound tension, as well as seroma or hematoma accumulation
underneath the skin flaps.
Lateral and Medial Skin Incisions
Lateral or medial incisions are useful when no need for a more extensile approach is anticipated (Table 57-1);
they can be complicated occasionally by neuromas (from transected
branches of the lateral or medial antebrachial cutaneous nerves),
especially on the medial side, but these more limited skin incisions
are associated with a lower rate of wound complications than the
posterior midline skin incision.
they can be complicated occasionally by neuromas (from transected
branches of the lateral or medial antebrachial cutaneous nerves),
especially on the medial side, but these more limited skin incisions
are associated with a lower rate of wound complications than the
posterior midline skin incision.
Lateral Approaches
The Köcher Approach
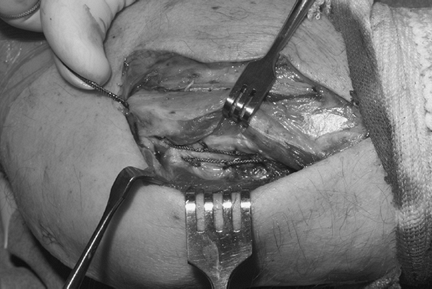
Classically, the lateral side of the elbow is exposed through the Köcher interval. This interval between the anconeus and the extensor carpi ulnaris
is easily identified distally and developed proximally in line with the
lateral epicondyle and humeral column. The underlying annular ligament,
lateral collateral ligament complex, and elbow capsule are easily
exposed. The Köcher approach can be used for radial head open reduction
and internal fixation (ORIF) or replacement and is especially useful
when the lateral collateral ligament complex is already injured, as in
most fracture-dislocations; it represents the standard approach for
reconstruction of the lateral collateral ligament (Fig. 57-1).
Release of the lateral collateral complex off the lateral epicondyle
through the Köcher interval allows great exposure of the subluxed or
is easily identified distally and developed proximally in line with the
lateral epicondyle and humeral column. The underlying annular ligament,
lateral collateral ligament complex, and elbow capsule are easily
exposed. The Köcher approach can be used for radial head open reduction
and internal fixation (ORIF) or replacement and is especially useful
when the lateral collateral ligament complex is already injured, as in
most fracture-dislocations; it represents the standard approach for
reconstruction of the lateral collateral ligament (Fig. 57-1).
Release of the lateral collateral complex off the lateral epicondyle
through the Köcher interval allows great exposure of the subluxed or
P.395
dislocated
joint. However, increased understanding of the role of the lateral
collateral ligament complex and concerns about its residual laxity
after detachment have prompted the use of alternative ligament-sparing
deep exposures.
|
TABLE 57-1 Procedures Commonly Performed Through a Lateral or Medial Skin Incision
|
||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
||||||||||||
Common Extensor Group Split
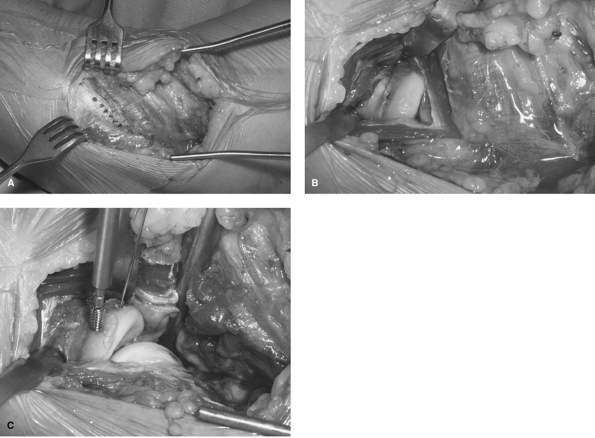
One of the best exposures for internal fixation or replacement of the radial head is through a split in the extensor carpi radialis brevis
(ECRB) in line with the Lister tubercle that is then continued
proximally by detachment of the common extensor origin and anterior
capsule off the lateral column. Incision of the annular ligament
underneath the ECRB provides access to the radial head, and the
supinator muscle can be elevated from proximal to distal if the radial
neck needs to be exposed (Fig. 57-2). Care
should be taken to protect the posterior interosseous nerve; placing
the forearm in pronation displaces this nerve distally and allows safe
exposure of at least 35 mm of proximal radius. A retractor placed
around the neck may be used to lever the radial head and neck
anteriorly for fixation or replacement.
(ECRB) in line with the Lister tubercle that is then continued
proximally by detachment of the common extensor origin and anterior
capsule off the lateral column. Incision of the annular ligament
underneath the ECRB provides access to the radial head, and the
supinator muscle can be elevated from proximal to distal if the radial
neck needs to be exposed (Fig. 57-2). Care
should be taken to protect the posterior interosseous nerve; placing
the forearm in pronation displaces this nerve distally and allows safe
exposure of at least 35 mm of proximal radius. A retractor placed
around the neck may be used to lever the radial head and neck
anteriorly for fixation or replacement.
 |
|
Figure 57-1
The Köcher approach uses the interval between anconeus and extensor carpi ulnaris. The interval is being used in this case to expose the lateral collateral ligament complex. |
Lateral Column
The proximal aspect of this approach, through detachment
of the extensor muscle group origin off the lateral column and distal
split of the extensor group in line with the Lister tubercle, allows
excellent exposure to the anterior compartment; the posterior
compartment can be easily exposed from the lateral side by elevation of
the triceps and anconeus off the lateral column. These two combined
form the basis of the so-called lateral column procedure (Fig. 57-3).
of the extensor muscle group origin off the lateral column and distal
split of the extensor group in line with the Lister tubercle, allows
excellent exposure to the anterior compartment; the posterior
compartment can be easily exposed from the lateral side by elevation of
the triceps and anconeus off the lateral column. These two combined
form the basis of the so-called lateral column procedure (Fig. 57-3).
Medial Approaches
As noted above, the skin of the medial aspect of the
elbow is richly innervated by multiple branches of the medial
antebrachial cutaneous nerve. Incisions placed on this area have a high
risk of neuroma formation, and some authors recommend identification
and preservation of these branches when a medial skin incision is used.
Alternatively, the medial aspect of the elbow may be exposed through a
posterior midline skin incision by elevation of a medial skin flap.
elbow is richly innervated by multiple branches of the medial
antebrachial cutaneous nerve. Incisions placed on this area have a high
risk of neuroma formation, and some authors recommend identification
and preservation of these branches when a medial skin incision is used.
Alternatively, the medial aspect of the elbow may be exposed through a
posterior midline skin incision by elevation of a medial skin flap.
Deep medial exposures vary depending on the procedure to be performed (Table 57-1). The medial side of the elbow joint is covered by the flexor-pronator group anteriorly and the triceps posteriorly. Medial collateral ligament (MCL) reconstruction
used to be performed through detachment of the flexor-pronator group;
currently, a muscle split is used for most MCL reconstructions, and
detachment of the flexor-pronator group is reserved for submuscular
transposition of the ulnar nerve, and may also be used for coronoid
exposure and sometimes resection of heterotopic ossification.
used to be performed through detachment of the flexor-pronator group;
currently, a muscle split is used for most MCL reconstructions, and
detachment of the flexor-pronator group is reserved for submuscular
transposition of the ulnar nerve, and may also be used for coronoid
exposure and sometimes resection of heterotopic ossification.
Different approaches may be used for coronoid exposure.
Coronoid plating and reconstruction require ample exposure. The author
favors elevation of the flexor-pronator group off the subcutaneous
border of the ulna from proximal to distal (Fig. 57-3).
This exposure allows identification and preservation of the MCL which
appears as a white collection of fibers as the fleshy flexor-pronator
group is elevated; it does not require formal transposition of the
ulnar nerve and limits the amount of muscle that needs to be detached
from the distal humerus, providing good exposure to both the coronoid
and the ulnar shaft.
Coronoid plating and reconstruction require ample exposure. The author
favors elevation of the flexor-pronator group off the subcutaneous
border of the ulna from proximal to distal (Fig. 57-3).
This exposure allows identification and preservation of the MCL which
appears as a white collection of fibers as the fleshy flexor-pronator
group is elevated; it does not require formal transposition of the
ulnar nerve and limits the amount of muscle that needs to be detached
from the distal humerus, providing good exposure to both the coronoid
and the ulnar shaft.
The so-called medial column procedure
provides access to both the anterior and the posterior compartments of
the elbow and is used mainly for contracture release The principles of
this approach are similar to those of the lateral column approach:
preservation of the collateral ligament and ample access to the joint
through a somewhat limited muscle dissection. The posterior compartment
of the elbow is exposed by elevation of the triceps off the medial
column. The anterior compartment is exposed by elevation of the
pronator teres off the medial intermuscular septum and the anterior
column; the exposure is extended distally
provides access to both the anterior and the posterior compartments of
the elbow and is used mainly for contracture release The principles of
this approach are similar to those of the lateral column approach:
preservation of the collateral ligament and ample access to the joint
through a somewhat limited muscle dissection. The posterior compartment
of the elbow is exposed by elevation of the triceps off the medial
column. The anterior compartment is exposed by elevation of the
pronator teres off the medial intermuscular septum and the anterior
column; the exposure is extended distally
P.396
through a split in the raphe between the flexor and pronator components of the flexor-pronator group.
 |
|
Figure 57-2 Radial head exposure through a muscle-splitting approach. A: The split in extensor carpi radialis brevis (ECRB) and proximal extension along the lateral column are marked in blue. B: The radial head is easily exposed through the split. C: Proximal extension of the approach along the column provides an excellent exposure for fixation or replacement.
|
 |
|
Figure 57-3
Coronoid fractures may be exposed medially by elevation of the flexor-pronator group from distal to proximal. The medial collateral ligament, deep to the muscle group, is pointed out by the forceps. The medial side of the trochlea and the coronoid lie just anterior to the ligament. |
The Extensor Mechanism
Internal fixation of most distal humerus fractures and
reconstruction of the elbow joint with either a joint prosthesis or
interposition arthroplasty often require mobilization of the extensor
mechanism. Table 57-2 summarizes surgical approaches to mobilize the triceps with some of their advantages and disadvantages.
reconstruction of the elbow joint with either a joint prosthesis or
interposition arthroplasty often require mobilization of the extensor
mechanism. Table 57-2 summarizes surgical approaches to mobilize the triceps with some of their advantages and disadvantages.
Working on Both Sides of the Triceps
This approach was originally described by Alonso-Llames
for the treatment of children’s supracondylar fractures and their
sequelae. Access to the distal humerus working on both sides of the
triceps is ideal, as it preserves the extensor mechanism intact.
However, it provides limited exposure to the articular surface. It is
used mainly for internal fixation of selected simple distal humerus
fractures, elbow arthroplasty in the presence of distal humeral bone
loss, and supracondylar osteotomies.
for the treatment of children’s supracondylar fractures and their
sequelae. Access to the distal humerus working on both sides of the
triceps is ideal, as it preserves the extensor mechanism intact.
However, it provides limited exposure to the articular surface. It is
used mainly for internal fixation of selected simple distal humerus
fractures, elbow arthroplasty in the presence of distal humeral bone
loss, and supracondylar osteotomies.
P.397
 |
|
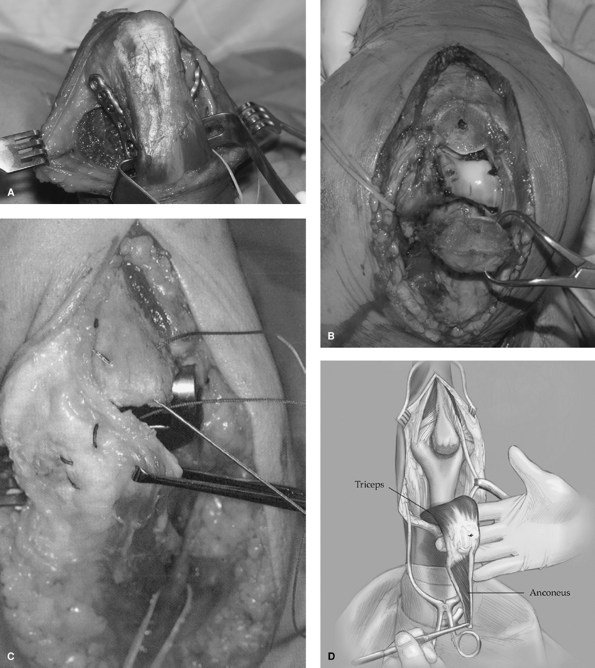
Figure 57-4 Some of the posterior exposures of the elbow joint. A: Paratricipital approach. B: Olecranon osteotomy. C: Bryan-Morrey triceps reflection. D: Triceps-reflecting anconeus pedicle (TRAP) approach.
|
Triceps-Reflection
The triceps can be detached off the olecranon and
reflected in continuity with the anconeus, forearm fascia, and ulnar
periosteum from either lateral to medial or medial to lateral (Fig. 57-4).
Reflection from medial to lateral, the Bryan-Morrey approach, is more
commonly used, especially for elbow arthroplasty. The Köcher interval
may be identified and developed laterally and the approach extended by
reflecting the triceps and anconeus from lateral to medial, the
so-called Mayo modified extensile Köcher approach. Both approaches
require secure reattachment of the extensor mechanism with
nonabsorbable transosseous sutures and avoidance of extension against
resistance for about 6 weeks.
reflected in continuity with the anconeus, forearm fascia, and ulnar
periosteum from either lateral to medial or medial to lateral (Fig. 57-4).
Reflection from medial to lateral, the Bryan-Morrey approach, is more
commonly used, especially for elbow arthroplasty. The Köcher interval
may be identified and developed laterally and the approach extended by
reflecting the triceps and anconeus from lateral to medial, the
so-called Mayo modified extensile Köcher approach. Both approaches
require secure reattachment of the extensor mechanism with
nonabsorbable transosseous sutures and avoidance of extension against
resistance for about 6 weeks.
P.398
Olecranon Osteotomy
This approach provides excellent exposure to the elbow
joint, especially for the management of complex distal humerus
fractures. There are some controversies regarding the ideal osteotomy
configuration and fixation technique. Currently, most authors favor a
chevron-shaped osteotomy initiated with a saw and completed with an
osteotome to create additional microinterdigitation at the osteotomy
site and avoid inadvertent damage to the articular cartilage. The
osteotomy should be centered at the bare area of the olecranon (Fig. 57-4).
joint, especially for the management of complex distal humerus
fractures. There are some controversies regarding the ideal osteotomy
configuration and fixation technique. Currently, most authors favor a
chevron-shaped osteotomy initiated with a saw and completed with an
osteotome to create additional microinterdigitation at the osteotomy
site and avoid inadvertent damage to the articular cartilage. The
osteotomy should be centered at the bare area of the olecranon (Fig. 57-4).
Plate fixation provides excellent stability, but it
seems to increase the rate of wound complications. Tension band wiring
using either a large-fragment partially threaded cancellous screw or
two Kirschner wires is commonly used. When screw fixation is selected,
drilling and tapping should be completed before performing the
osteotomy, and screw length should be enough to provide cortical
engagement while avoiding mediolateral translation of the osteotomized
fragment with introduction of a long straight screw in the bowed ulnar
canal. When Kirschner wires are used, wire placement through the
anterior ulnar cortex may decrease the risk of postoperative migration.
The main complications
seems to increase the rate of wound complications. Tension band wiring
using either a large-fragment partially threaded cancellous screw or
two Kirschner wires is commonly used. When screw fixation is selected,
drilling and tapping should be completed before performing the
osteotomy, and screw length should be enough to provide cortical
engagement while avoiding mediolateral translation of the osteotomized
fragment with introduction of a long straight screw in the bowed ulnar
canal. When Kirschner wires are used, wire placement through the
anterior ulnar cortex may decrease the risk of postoperative migration.
The main complications
P.399
of olecranon osteotomy are nonunion and hardware-related complications.
Triceps Split
The triceps can be split in the midline to expose the
distal part of the humerus. The split may be extended distally by
elevation of medial and lateral subperiosteal flaps off the ulna. This
approach is recommended by some mainly for elbow arthroplasty. It
maintains the extensor mechanism centralized, but the attachment of the
medial half of the triceps is often thin, which may compromise the
quality of the repair.
distal part of the humerus. The split may be extended distally by
elevation of medial and lateral subperiosteal flaps off the ulna. This
approach is recommended by some mainly for elbow arthroplasty. It
maintains the extensor mechanism centralized, but the attachment of the
medial half of the triceps is often thin, which may compromise the
quality of the repair.
The Triceps-Reflecting Anconeus Pedicle Approach
The triceps-reflecting anconeus pedicle (TRAP) approach
was developed for internal fixation of complex distal humerus fractures
to avoid the disadvantages of olecranon osteotomy while providing
improved exposure over triceps-reflection approaches. It basically
involves complete detachment of the triceps and anconeus off the
proximal ulna by combining the Bryan-Morrey and the extensile Köcher
approaches (Fig. 57-4). The joint can be
exposed by elbow hyperextension, and the ulna is kept intact to be used
as a template for reconstruction of the distal humerus articular
surface or in case conversion to elbow replacement becomes necessary.
It may lead to weakness in terminal extension.
was developed for internal fixation of complex distal humerus fractures
to avoid the disadvantages of olecranon osteotomy while providing
improved exposure over triceps-reflection approaches. It basically
involves complete detachment of the triceps and anconeus off the
proximal ulna by combining the Bryan-Morrey and the extensile Köcher
approaches (Fig. 57-4). The joint can be
exposed by elbow hyperextension, and the ulna is kept intact to be used
as a template for reconstruction of the distal humerus articular
surface or in case conversion to elbow replacement becomes necessary.
It may lead to weakness in terminal extension.
Anterior Approaches
Anterior approaches to the elbow have very specific
indications. Some authors recommend an anterior approach for
contracture release, but access to the posterior compartment is
required for most contracted elbows, which makes this approach somewhat
unappealing. Currently, the anterior aspect of the elbow is exposed
most commonly for repair of distal biceps tendon injuries. Either a
small anterior incision used to retrieve the tendon is then combined
with a second incision in the proximal aspect of the dorsal forearm, or
a single larger anterior approach is used for both tendon retrieval and
reattachment. Care should be taken to protect the median and radial
nerves as well as the brachial artery. Care should also be taken to
avoid crossing the elbow flexion crease at a right angle to decrease
the chance of skin contracture limiting elbow extension. Moisture
accumulated in the elbow flexion crease when the joint is immobilized
in some flexion may increase the risk of wound-related complications
after any anterior approach.
indications. Some authors recommend an anterior approach for
contracture release, but access to the posterior compartment is
required for most contracted elbows, which makes this approach somewhat
unappealing. Currently, the anterior aspect of the elbow is exposed
most commonly for repair of distal biceps tendon injuries. Either a
small anterior incision used to retrieve the tendon is then combined
with a second incision in the proximal aspect of the dorsal forearm, or
a single larger anterior approach is used for both tendon retrieval and
reattachment. Care should be taken to protect the median and radial
nerves as well as the brachial artery. Care should also be taken to
avoid crossing the elbow flexion crease at a right angle to decrease
the chance of skin contracture limiting elbow extension. Moisture
accumulated in the elbow flexion crease when the joint is immobilized
in some flexion may increase the risk of wound-related complications
after any anterior approach.
Suggested Readings
Aldridge JM III, Atkins TA, Gunneson EE, et al. Anterior release of the elbow for extension loss. J Bone Joint Surg. 2004;86A(9):1955–1960.
Alonso-Llames
M. Bilaterotricipital approach to the elbow. Its application in the
osteosynthesis of supracondylar fractures of the humerus in children. Acta Orthop Scand. 1972;43(6):479–490.
M. Bilaterotricipital approach to the elbow. Its application in the
osteosynthesis of supracondylar fractures of the humerus in children. Acta Orthop Scand. 1972;43(6):479–490.
Bryan RS, Morrey BF. Extensive posterior exposure of the elbow. A triceps-sparing approach. Clin Orthop. 1982;166:188–192.
Diliberti
T, Botte MJ, Abrams RA. Anatomical considerations regarding the
posterior interosseous nerve during posterolateral approaches to the
proximal part of the radius. J Bone Joint Surg. 2000;82A:809–813.
T, Botte MJ, Abrams RA. Anatomical considerations regarding the
posterior interosseous nerve during posterolateral approaches to the
proximal part of the radius. J Bone Joint Surg. 2000;82A:809–813.
Dowdy PA, Bain GI, King GJ, et al. The midline posterior elbow incision. An anatomical appraisal. J Bone Joint Surg. 1995;77B:696–699.
Frankle MAMD. Triceps split technique for total elbow arthroplasty. Techniques Shoulder Elbow Surg. 2002;3(1):23–27.
Husband JB, Hastings H II. The lateral approach for operative release of post-traumatic contracture of the elbow. J Bone Joint Surg. 1990;72A:1353–1358.
Mansat P, Morrey BF. The column procedure: a limited lateral approach for extrinsic contracture of the elbow. J Bone Joint Surg. 1998;80A:1603–1615.
Morrey BF. Anatomy and surgical approaches. In: Morrey BF, ed. Joint Replacement Arthroplasty. Philadelphia: Churchill-Livingstone; 2003:269–285.
O’Driscoll SW. The triceps-reflecting anconeus pedicle (TRAP) approach for distal humeral fractures and nonunions. Orthop Clin North Am. 2000;31(1):91–101.
Ring D, Gulotta L, Chin K, et al. Olecranon osteotomy for exposure of fractures and nonunions of the distal humerus. J Orthop Trauma. 2004;18(7):446–449.
Schildhauer TA, Nork SE, Mills WJ, et al. Extensor mechanism-sparing paratricipital posterior approach to the distal humerus. J Orthop Trauma. 2003;17(5):374–378.
Wada T, Ishii S, Usui M, et al. The medial approach for operative release of post-traumatic contracture of the elbow. J Bone Joint Surg. 2000;82B:68–73.