
Editors: Frassica, Frank J.; Sponseller, Paul D.; Wilckens, John H.
Title: 5-Minute Orthopaedic Consult, 2nd Edition
Copyright ©2007 Lippincott Williams & Wilkins
> Table of Contents > Knee Anatomy and Examination
Knee Anatomy and Examination
Timothy S. Johnson MD
Constantine A. Demetracopoulos BS
Description
-
Anatomy of the knee consists of compartments, bones, menisci, ligaments, muscles, and nerves.
-
3 compartments:
-
Medial, lateral, and patellofemoral
-
-
Bones: Patella:
-
Serves as fulcrum to aid knee extension
-
-
Medial and lateral menisci:
-
Fibrocartilaginous structures in medial and lateral femorotibial compartments
-
Aid in joint lubrication and nutrition and in load distribution across articular cartilage
-
-
Ligaments/tendons:
-
Patellar ligament/tendon: Distal part of
quadriceps tendon originating from the apex of the patella and
inserting on the tibial tuberosity -
ACL:
-
Originates from the posteromedial aspect of the lateral femoral condyle and attaches to the tibia’s anterior intercondylar spine
-
Prevents anterior displacement of the tibia on the femur
-
-
PCL:
-
Originates from the anterolateral aspect
of the medial femoral condyle and inserts on the posterior
intercondylar spine of the tibia -
Prevents posterior displacement of the tibia on the femur during knee flexion
-
-
MCL:
-
Originates on the medial femoral epicondyle and inserts on the medial tibial plateau and medial meniscus
-
Stabilizes the knee against valgus loads
-
-
LCL and posterolateral corner complex:
-
Originates on the lateral femoral epicondyle and inserts on the fibular head
-
Stabilizes the knee against varus loads
-
Resists tibial external rotation
-
-
-
Muscles:
-
Quadriceps (extensors): Rectus femoris, vastus lateralis, vastus intermedius, vastus medialis
-
Hamstrings (flexors): Biceps femoris, semimembranosus, semitendinosus, gracilis
-
-
Nerves:
-
Femoral: Innervates quadriceps
-
Sciatic: Bypasses knee posteriorly with popliteal vessels
-
Common peroneal: Major branch of the sciatic that travels laterally around the fibular neck
-
Signs and Symptoms
History and Physical Exam
-
Initial assessment:
-
Assess the contralateral knee for comparison.
-
Assess for referred pain from the spine or hip.
-
Perform a complete neurovascular examination of the extremities.
-
ROM:
-
Normal = 0–155°
-
Flexion contracture: Incomplete passive and active extension
-
Extension lag: Full passive extension with incomplete active extension
-
-
-
Inspection:
-
Observe knees for erythema, effusion, and skin abrasion.
-
Observe for muscular atrophy.
-
Assess standing varus/valgus alignment.
-
Physiologic alignment is approximately 5° of valgus for males and 7° of valgus for females.
-
-
Assess gait.
-
Antalgic gait: Shortened stride and decreased stance phase on the affected leg
-
-
-
Palpation:
-
With the knee at 90° of flexion, palpate
along the course of the patellar and quadriceps tendons, medial and
lateral joint lines, the MCL, the LCL, and the iliotibial band. -
Localize painful structures.
-
-
Knee effusion:
-
Marked effusion can be secondary to
hemarthrosis (fracture, ligamentous or meniscal tear) or inflammation
(arthritis, gout, infection). -
Assess the knee joint for warmth, which may indicate active inflammation.
-
Blot test:
-
Press the patella against the femoral groove.
-
If a large effusion is present, the fluid will be forced out of the groove and cause the patella to rebound as it flows back in.
-
-
-
Prepatellar bursitis:
-
A fluctuant, painful subcutaneous swelling anterior to the patella with anterior knee pain
-
-
Popliteal cyst (Baker cyst):
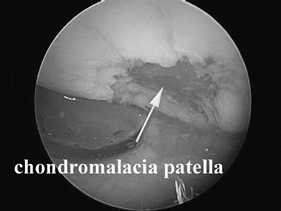 Fig. 1. Arthroscopic photo of an articular cartilage injury on the patella.
Fig. 1. Arthroscopic photo of an articular cartilage injury on the patella.-
Painful swelling of the popliteal fossa.
-
Usually indicates intra-articular pathology
-
-
ITBS:
-
Lateral knee pain, localized specifically over the lateral epicondyle commonly seen as an overuse injury in runners and cyclists
-
Ober test:
-
With the patient lying on the unaffected side, and with the unaffected hip and knee flexed to 90°, stabilize the pelvis.
-
With the affected leg abducted and extended, lower it into adduction.
-
If the iliotibial band is tight, the leg
will remain in the abducted position and/or the patient may complain of
lateral knee pain.
-
-
-
Patellar fracture, patellar tendon/quadriceps tendon rupture:
-
Palpable defect of affected structure
-
Extension lag
-
-
Patellofemoral syndrome
-
Anterior knee pain with standing from a seated position, squatting, or stair-climbing
-
Q angle:
-
Angle of the anterior superior iliac spine, patella, and tibial tubercle
-
An angle >15° may suggest patellar instability.
-
-
Medial and lateral glide test:
-
With the affected knee extended, determine the number of quadrants the patella will translate over the trochlear groove.
-
<1 quadrant medially suggests lateral patellofemoral compression syndrome.
-
-
Apprehension test:
-
With the affected knee in full extension, translate the patella laterally.
-
Apprehension during this maneuver suggests patella instability.
-
-
Grind test:
-
Press the patella distally against the trochlear groove.
-
Then have the patient contract the quadriceps while palpating for crepitus indicative of patellofemoral arthrosis (Fig. 1).
![]() Fig. 2. MRI of an ACL rupture of the femur.
Fig. 2. MRI of an ACL rupture of the femur.
-
-
-
Ligamentous instability:
-
Mechanism of injury may indicate cause of instability.
-
ACL: Noncontact, twisting/pivoting motion with foot firmly planted and audible “pop”
-
PCL: Dashboard injuries
-
MCL/LCL: Extreme valgus/varus force about the knee
-
-
Ligament tears frequently are accompanied by an acute hemarthrosis.
-
Knee feels like it “gives out” or “buckles.”
-
Varus and valgus stress test (MCL/LCL) (1):
-
With the knee flexed to 30°, place 1 hand on the patient’s distal thigh and with the other, grasp the patient’s ankle.
-
Apply varus/valgus stress in coronal plane with the knee in 30° of flexion.
-
If instability is detected, the collateral ligament has been injured.
-
Grades: 1, <5 mm; 2, 5–10 mm; 3, >10 mm
-
-
Lachman test (ACL) (Fig. 2):
-
Most sensitive test for ACL integrity
-
With the patient’s knee relaxed and flexed at 30°, place 1 hand on the distal thigh and the other on the proximal tibia.
-
Then translate the tibia anteriorly.
-
Test is abnormal if there is >5 mm of
translation and/or >3 mm difference between the values for the
affected and uninjured knees.
-
-
Anterior and posterior drawer test (ACL/PCL) (2):
-
Place the knee in 90° of flexion and neutral rotation, and stabilize the foot.
-
Place both hands around the proximal tibia and attempt to translate the tibia anteriorly and posteriorly on the femur.
-
Subluxation anteriorly suggests ACL instability. Similarly, subluxation posteriorly suggests PCL instability.
-
Grades: 1, <5 mm; 2, 5–10 mm; 3, >10 mm
-
-
External rotation test (posterolateral corner):
-
Test with the patient prone.
-
Simultaneously compare the affected and normal knees.
-
Starting at 0° of knee flexion, externally rotate the tibia and observe the thigh–foot angle.
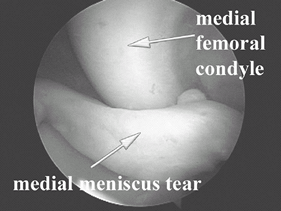 Fig. 3. Arthroscopic photograph of an unstable bucket-handle medial meniscus tear.
Fig. 3. Arthroscopic photograph of an unstable bucket-handle medial meniscus tear. -
Look for excessive external rotation (>10°) on the affected side.
-
Repeat at 30° and 90°.
-
Increased external rotation only at ≤30° of knee flexion indicates an isolated PLC injury.
-
Increased external rotation at ≤30° and at 90° of knee flexion indicates posterolateral corner and PCL insufficiency.
-
-
-
Meniscal pathology (3) (Fig. 3):
-
Patient complains of episodic painful “mechanical symptoms” that may present with the knee locked in flexion.
-
Patient presents with focal tenderness to palpation on the affected joint line (best examined with the knee flexed at 90°).
-
McMurray test:
-
With the patient supine and the knee in
full flexion, internally rotate the tibia and apply a valgus force to
load the lateral meniscus. -
Then passively extend the knee to 0° of flexion while palpating the lateral joint line.
-
The test is positive if an audible or palpable click is produced during extension.
-
Reposition the knee in full flexion and
repeat the test with the tibia in external rotation by applying varus
force and palpating the medial joint line to test the medial meniscus. -
Pain may be associated with this maneuver.
-
-
Apley compression and dislocation test:
-
With the patient prone and the knee
flexed at 90°, grasp the heel and axially load the tibia while
simultaneously externally and internally rotating the foot. -
Pain localized to the medial joint line with compression and rotation suggests medial meniscus abnormality.
-
Pain localized to the lateral joint line with compression and rotation suggests lateral meniscus abnormality.
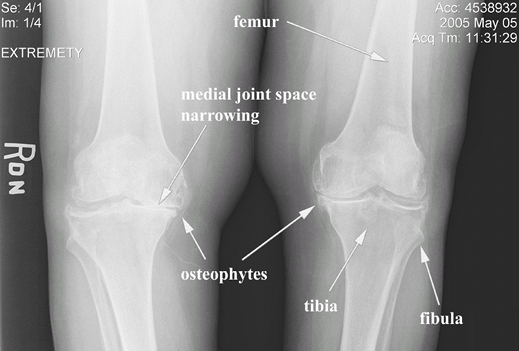
![]() Fig. 4. Radiograph of advanced knee osteoarthritis.
Fig. 4. Radiograph of advanced knee osteoarthritis.
-
-
-
Knee arthritis (Fig. 4):
-
Patients complain of morning stiffness and soreness.
-
Intra-articular swelling can be variable.
-
Osteophytes and crepitus may be palpable.
-
Flexion contractures with reduced ROM and marked functional limitations are common.
-
Late stages of degenerative arthritis are associated with pseudolaxity on valgus/varus testing.
-
Radiographs show joint space narrowing and osteophytes (Fig. 3).
-

P.211
References
1. Grood
ES, Noyes FR, Butler DL, et al. Ligamentous and capsular restraints
preventing straight medial and lateral laxity in intact human cadaver
knees. J Bone Joint Surg 1981;63A:1257–1269.
ES, Noyes FR, Butler DL, et al. Ligamentous and capsular restraints
preventing straight medial and lateral laxity in intact human cadaver
knees. J Bone Joint Surg 1981;63A:1257–1269.
2. Cosgarea AJ, Jay PR. Posterior cruciate ligament injuries: evaluation and management. J Am Acad Orthop Surg 2001;9:297–307.
3. Greis PE, Bardana DD, Holmstrom MC, et al. Meniscal injury: I. Basic science and evaluation. J Am Acad Orthop Surg 2002;10:168–176.
Additional Reading
Hoppenfeld S. Physical examination of the knee. In: Physical Examination of the Spine and Extremities. Norwalk, CT: Appleton-Century-Crofts, 1976:171–196.
Hoppenfeld S, deBoer P. The knee. In: Surgical Exposures in Orthopaedics: The Anatomical Approach, 3rd ed. Philadelphia: Lippincott, Williams & Wilkins, 2003:493–568.
FAQ
Q: In addition to pain, of what do people with knee ligament injuries complain most commonly?
A: Instability or buckling of the knee.
Q: In addition to pain, what is the classic chief complaint of a person with an unstable meniscus tear?
A: Locking of the knee in a flexed position.