
Editors: Chelly, Jacques E.
Title: Peripheral Nerve Blocks: A Color Atlas, 3rd Edition
Copyright ©2009 Lippincott Williams & Wilkins
> Table of Contents > Section III – Continuous Nerve Blocks > 27 – Continuous Axillary Block
27
Continuous Axillary Block
Ralf Gebhard
Anesthesia and postoperative analgesia for surgery at the elbow and
below (hand and forearm) and continuous sympathectomy following finger
reimplantation.
The axillary artery pulse is palpated and marked in the middle of the
axilla. After disinfection, sterile draping, and local infiltration
with 1% lidocaine, a 50-mm insulated introducer needle or cannula
connected to a nerve stimulator (1.5 mA, 2 Hz, 0.1 ms) is inserted
above the artery, pointing in a proximal direction almost parallel to
the artery at a 30° to 45° angle to the skin (Fig. 27-1A).
After identification of a median, or radial nerve response at a current
below 0.5 mA, the volume is injected slowly (10 mL/min) and in 5 mL
increments. The catheter is then introduced and threaded approximately
5 cm beyond the needle tip (Fig. 27-1B). The introducing needle is removed and the catheter is secured in place and covered with a transparent dressing (Fig. 27-1C).
-
To facilitate threading of the catheter,
it can be helpful to lower the needle to an angle of approximately 15°
to the skin. In contrast, if a Tuohy needle is used, elevation of the
P.235
needle to an angle of approximately 45° may be necessary to allow for easy catheter insertion.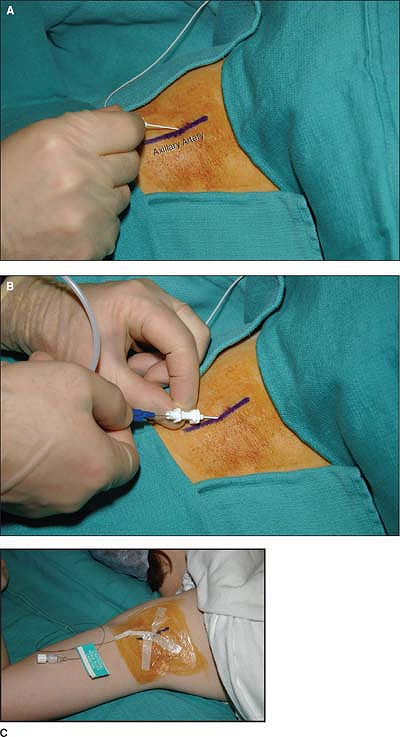 Figure 27-1. A: An insulated introducer needle or cannula connected to a nerve stimulator is inserted above the artery. B: The catheter is introduced and threaded. C: The introducing needle is removed and the catheter is secured in place and covered with a transparent dressing.
Figure 27-1. A: An insulated introducer needle or cannula connected to a nerve stimulator is inserted above the artery. B: The catheter is introduced and threaded. C: The introducing needle is removed and the catheter is secured in place and covered with a transparent dressing. -
The catheter should be aspirated with a
2-ml syringe before a continuous infusion is started. Catheter
dislocation into a blood vessel is possible, even if no blood could be
aspirated after the initial needle placement. -
Patient-controlled local anesthetic
administration via axillary catheters has been associated with
reduction of local anesthetic requirements and has resulted in higher
patient satisfaction. -
These catheters can be used for up to
several weeks. However, careful local care and daily inspection of the
catheter site are recommended to avoid infection. -
This technique represents an interesting
alternative to the stellate ganglion block for the treatment of reflex
sympathetic dystrophy.
P.236
Suggested Readings
Ang ET, Lassale B, Goldfarb G. Continuous axillary brachial plexus block: a clinical and anatomical study. Anaesth Analg 1984;63:680–684.
Iskandar
H, Rakotondriamihary S, Dixmerias F, et al. Analgesia using continuous
axillary block after surgery of severe hand injuries:
self-administration versus continuous injection. Ann Fr Anesth Reanim 1998:1099–1103.
H, Rakotondriamihary S, Dixmerias F, et al. Analgesia using continuous
axillary block after surgery of severe hand injuries:
self-administration versus continuous injection. Ann Fr Anesth Reanim 1998:1099–1103.
Matuszczak M, Gebhard R, Schmitz B, et al. Continuous axillary block for effective long-term postoperative analgesia. The Internet Journal of Anesthesiology 2000;4.
Mezzatesta
JP, Scott DA, Schweitzer SA, et al. Continuous axillary brachial plexus
block for postoperative pain relief. Intermittent bolus versus
continuous infusion. Reg Anesth 1997;22:357–362.
JP, Scott DA, Schweitzer SA, et al. Continuous axillary brachial plexus
block for postoperative pain relief. Intermittent bolus versus
continuous infusion. Reg Anesth 1997;22:357–362.
Murray P, Floor K, Atkinson RE. Continuous axillary brachial plexus blockade for reflex sympathetic dystrophy. Anaesthesia 1995;50:633–635.
Neimkin RJ, May JW Jr, Roberts J, et al. Continuous axillary block through an indwelling Teflon catheter. J Hand Surg 1984;9:830–833.
Salonen
MH, Haasio J, Bachman M, et al. Evaluation of efficacy and plasma
concentrations of ropivacaine in continuous axillary brachial plexus
block: high dose for surgical anesthesia and low dose for postoperative
analgesia. Reg Anesth Pain Med 2000;25:47–51.
MH, Haasio J, Bachman M, et al. Evaluation of efficacy and plasma
concentrations of ropivacaine in continuous axillary brachial plexus
block: high dose for surgical anesthesia and low dose for postoperative
analgesia. Reg Anesth Pain Med 2000;25:47–51.
Selander D. Catheter technique in axillary plexus block. Presentation of a new method. Acta Anaesthesiol Scand 1977;21:324–329.