
glenohumeral joint, the scapulothoracic articulation, the
acromioclavicular joint, and the sternoclavicular joint. The
coordinated activity of these articulations provides greater motion
than any other joint in the body. Bony constraints are limited. To
achieve stability during motion, the ligamentous restraints and
muscular activity are crucial to shoulder biomechanics.
static stability, and dynamic stability of the four main articulations
forming the shoulder complex. Clinical examples of applied biomechanics
are provided in each section.
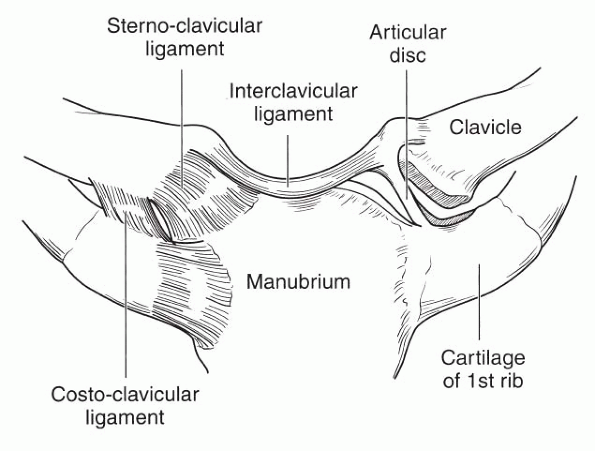
responsible for linking the upper extremity directly to the thorax. The
joint consists of the enlarged, saddle-shaped medial end of the
clavicle that articulates with the superolateral aspect of the
manubrium and a small facet on the first rib. The sternoclavicular
joint contains a fibrocartilaginous articular disc, or meniscus, that
completely covers the articular surfaces and divides the joint into two
compartments. The joint is surrounded by a capsule and the anterior and
posterior sternoclavicular ligaments. Joint stability is achieved from
the costoclavicular and interclavicular ligaments (Fig. 14-1).
The costoclavicular ligaments are lateral to the joint capsule and run
between the undersurface of the medial end of the clavicle and the
first rib.
thorax to the upper extremity and links the sternoclavicular joint to
the acromioclavicular joint. The clavicle is an S-shaped bone with the
medial two thirds of the body having an anterior convexity and the
lateral third having an anterior concavity. These curvatures contribute
to the normal appearance and contour of the upper chest. In addition to
serving
as the attachment site for many of the muscles that act on the
shoulder, the clavicle protects the underlying brachial plexus and
vascular structures.
 |
|
Figure 14-1
Anatomy of the sternoclavicular joint. Note that the articular disc divides the joint into two compartments. (From Squire ME, Esmail AN, Soslowsky LJ. Anatomy and biomechanics of the shoulder. In: McGinty JB, Burkhart SS, Jackson RW et al., eds. Operative Arthroscopy, 3rd ed. Philadelphia: Lippincott Williams & Wilkins, 2003:162.) |
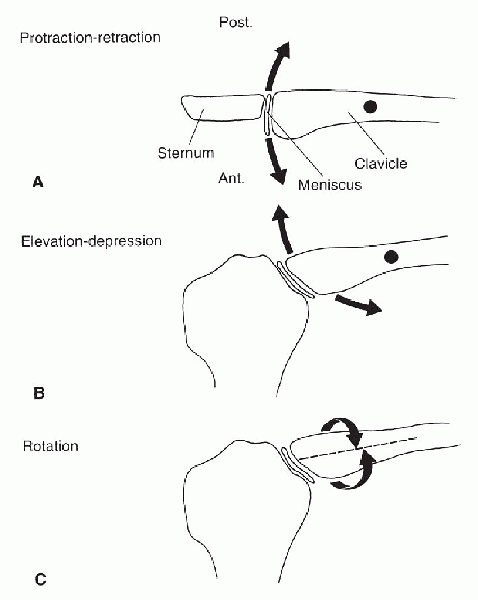
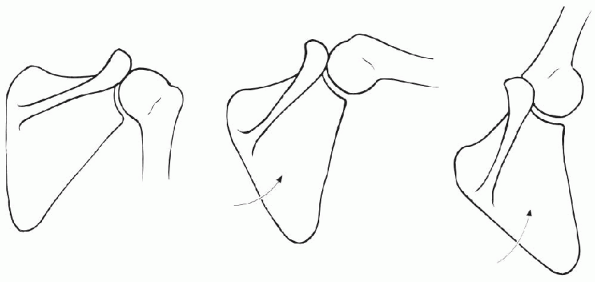
protraction-retraction, elevation-depression, and rotation. Elevation
and depression result in motion between the clavicle and the disc, and
rotary movements in motion between the disc and the sternum. The normal
range of motion of the sternoclavicular joint is up to 35 degrees of
protraction-retraction (Fig. 14-2A), and 35 degrees of upward elevation (Fig. 14-2B). Rotation along the axis of the clavicle is up to 50 degrees (Fig. 14-2C).
In the first 70 degrees of shoulder elevation, motion occurring at the
sternoclavicular joint is mostly clavicular elevation with little axial
rotation. Beyond approximately 70 degrees of arm elevation, clavicular
rotation starts to occur.
coordinated motion between the glenohumeral and sternoclavicular
joints. For every 10 degrees of arm elevation, there is approximately 4
degrees of clavicular elevation. If the sternoclavicular joint were to
be surgically fused, shoulder motion would be significantly impaired
with shoulder abduction limited to approximately 90 degrees.
bony stability. Stability is provided by the articular disc, in
conjunction with the anterior and posterior sternoclavicular ligaments,
the costoclavicular ligament, and the interclavicular ligaments (Fig. 14-1).
The major constraint to sternoclavicular motion is the costoclavicular
ligament, which resists upward, as well as posterior, displacement of
the clavicle. The anterior and posterior sternoclavicular ligaments
provide stability to anterior and posterior translations, as well as
superior displacement. The interclavicular ligament, connecting the
superomedial aspect of the clavicles, becomes taut when the arm is
depressed and relaxed when the arm is elevated. The interclavicular
ligament assists with restraining the joint superiorly, with the
posterior portion also contributing to anterior stability of the
sternoclavicular joint. Finally, the articular disc contributes to
limiting inferior displacement through articular contact and also
prevents medial displacement of the clavicle.
 |
|
Figure 14-2 Motion at the sternoclavicular joint. A: Axial (transverse) view with clavicular protraction and retraction. B: Coronal view demonstrating elevation and depression. C:
Coronal view demonstrating rotation along the longitudinal axis of the clavicle. (From Della Valle CJ, Rokito AS, Gallagher Birdzell M, et al. Biomechanics of the shoulder. In: Nordin M, Frankel VH, eds. Basic Biomechanics of the Musculoskeletal System. Baltimore: Lippincott Williams & Wilkins, 2001:321.) |
sufficient stability of the proximal clavicle to allow resection of the
medial clavicle in cases of arthrosis. However, if the costoclavicular
ligaments have been previously injured, as in the case of a
sternoclavicular dislocation, then excision of the medial clavicle
alone will lead to instability of the proximal clavicle, and
consideration must be given to costoclavicular ligament reconstruction.
the lateral clavicle to the acromion. The joint lies in an
anteroposterior direction and has a variable tilt anywhere from a
vertical orientation in the sagittal plane to a 50-degree tilt, with
the clavicle overriding the acromion (Fig. 14-3).
It is subject to high loads transmitted from the chest musculature and
is stabilized by the acromioclavicular joint ligaments (capsular
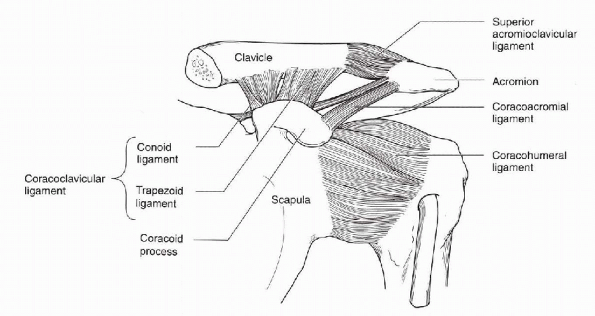
thickenings) and the coracoclavicular ligaments. The coracoclavicular
ligaments consist of the posteromedially directed conoid ligament and
the anterolaterally directed trapezoid ligament. The coracoacromial
ligament lies anterior and lateral to the acromioclavicular joint and
runs from the most lateral aspect of the coracoid to the medial aspect
of the acromion.
disc that originates from the superior aspect of the joint and whose
function is poorly understood. Unlike the disc of the sternoclavicular
joint, the acromioclavicular joint disc usually has a perforation at
the center. The joint is composed of hyaline cartilage early in life,
but transforms to fibrocartilage on the acromial side by age 17 and on
the clavicular side by age 23.
synchronous, with little relative motion at the acromioclavicular
joint. The majority of scapulothoracic motion occurs with coordinated
sternoclavicular joint movement, and thus rigid fixation or fusion of
the acromioclavicular joint produces little loss of overall shoulder
function.
 |
|
Figure 14-3
Anatomy of the acromioclavicular joint. The coracoclavicular ligaments (conoid and trapezoid) and the primary vertical stabilizer. The superior acromioclavicular ligament is the primary horizontal stabilizer. (From Squire ME, Esmail AN, Soslowsky LJ. Anatomy and biomechanics of the shoulder. In: McGinty JB, Burkhart SS, Jackson RW, et al., eds. Operative Arthroscopy, 3rd ed. Philadelphia: Lippincott Williams & Wilkins, 2003:163.) |
restraint to horizontal and rotational stability. Specifically, the
superior acromioclavicular ligament is the most important stabilizer to
anteroposterior translation. With some contribution of the
acromioclavicular ligaments, the primary restraint to vertical
stability is the coracoclavicular ligaments (conoid and trapezoid),
which can be viewed as suspending the scapula from the clavicle. The
smaller conoid ligament acts to limit superior-inferior displacement of
the clavicle. The quadrilaterally shaped trapezoid, lateral to the
conoid, is the larger and stronger of the two ligaments and resists
axial compression and motion about the horizontal axis. The deltoid and
trapezius muscles also help stabilize the acromioclavicular joint and
have fibers that blend with the superior acromioclavicular ligament.
The exact contribution of the deltoid and trapezius to stability is not
known.
clinical problem, and an understanding of the anatomy and biomechanics
will help guide proper diagnosis and treatment. When the
acromioclavicular joint ligaments have been disrupted with intact or
strained coracoclavicular ligaments (i.e., a type II injury), physical
examination will demonstrate horizontal instability but will not
demonstrate any vertical stability. When the coracoclavicular ligaments
are also injured (i.e., type III to type V injuries), vertical
instability of the acromioclavicular joint will also be clinically
evident. Finally, if the deltotrapezial fascia is also injured, leading
to complete joint dislocation (type V injury), then—in
addition
to horizontal and vertical instability—the acromion can be passively
brought under the distal clavicle with cross-body adduction of the arm.
 |
|
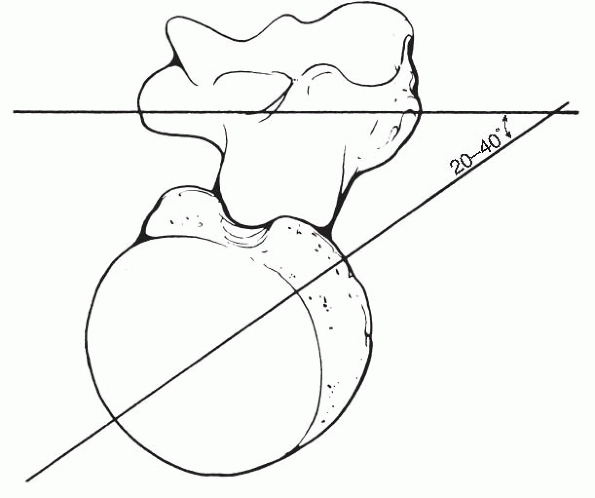
Figure 14-4
Orientation of the humeral head demonstrating retroversion with respect to the transepicondylar axis at the elbow. (From O’Brien SJ, Fealy S, Drakos M, et al. Developmental anatomy of the shoulder and anatomy of the glenohumeral joint. The normal retroversion is usually in the range from 20 degrees to 40 degrees. In: Rockwood CA Jr, Matsen FA III, Wirth MA, et al., eds. The Shoulder, 3rd ed. Philadelphia: Saunders-Elsevier, 2004:13.) |
 |
|
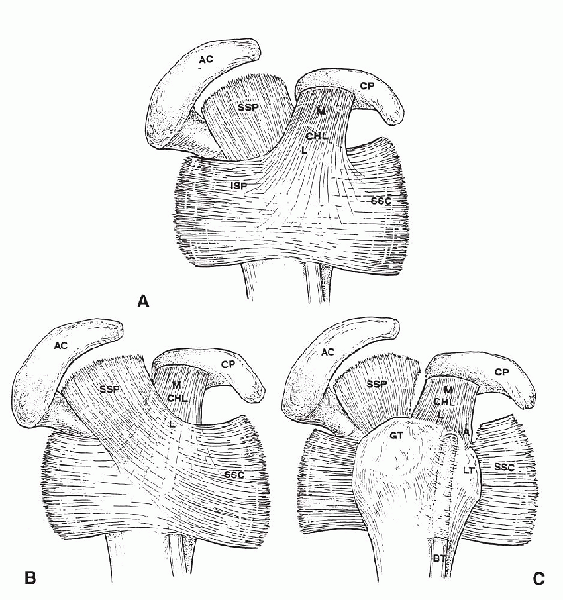
Figure 14-5 Anterolateral view of a right shoulder demonstrating rotator cuff insertions and the rotator interval. A: The superficial layer of the rotator interval consists of the superficial fibers of the coracohumeral ligament (CHL), which extend to the insertions of the supraspinatus (SSP) and subscapularis (SSC). B: The second layer of the rotator interval showing fibers of SSP and SSC crossing through the interval and uniting with CHL. C: The third layer of the rotator interval consists of deep fibers of CHL inserting into the greater tuberosity (GT) and lesser tuberosity (LT), and forming an anterior covering band (A) around the long biceps tendon (BT). AC, acromion; CP, coracoid process; ISP, infraspinatus; L, lateral; M,
medial. (From Jost B, Koch PP, Gerber C. Anatomy and functional aspects of the rotator interval. J Shoulder Elbow Surg 2000;9:336-341.) |
is nearly spherical in shape. The articular surface forms a 120-degree
arc and has an upward or medial inclination of 45 degrees. When
referenced from the transepicondylar axis of the distal humerus, the
humeral head is retroverted, or posteriorly directed, with respect to
the intercondylar plane of the distal humerus (Fig. 14-4).
There is a wide range of humeral retroversion among individuals, and
most surgeons use the range of 20 to 40 degrees of humeral retroversion
as a guide during reconstructive procedures.
are innervated from the suprascapular nerve, whereas the teres minor is
innervated by a branch of the axillary nerve, and the subscapularis is
innervated by the upper and lower subscapular nerves. The supraspinatus
originates from the supraspinatus fossa of the scapula and inserts on
the greater tuberosity on the superior aspect of the proximal humerus.
The infraspinatus and teres minor muscles originate from the posterior
aspect of the scapula below the scapular spine and insert on the
posterior aspect of the greater tuberosity. The subscapularis, which
lies on the anterior surface of the scapula, inserts on the lesser
tuberosity. The rotator cuff tendons have well-defined, relatively
broad insertions on the tuberosities, with the average
medial-to-lateral distance across the supraspinatus insertion measuring
12.7 mm.
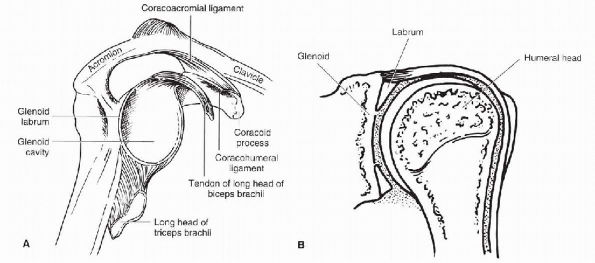
The triangular area bound by the superior edge of the subscapularis,
the anterior edge of the supraspinatus, and the base of the coracoid
define the rotator interval. Deep to the capsule of the rotator
interval lies the long head of the biceps tendon that exits the
glenohumeral joint at the apex of this triangular region.
 |
|
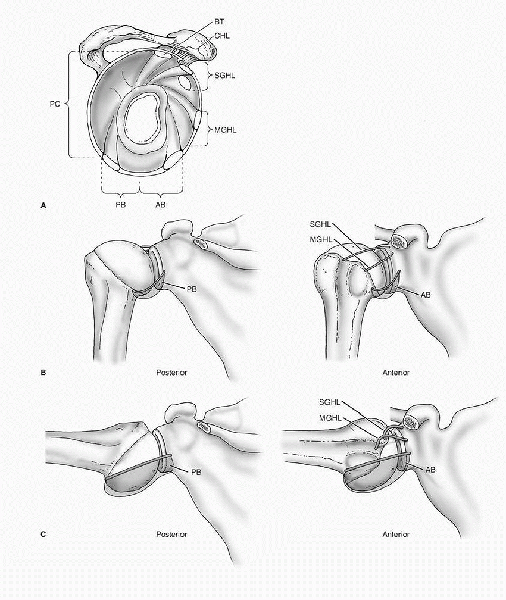
Figure 14-6 A: Section through the glenohumeral joint capsule perpendicular to the plane of the scapula. AB, anterior band of inferior glenohumeral ligament; BT, long head of biceps tendon; MGHL, middle glenohumeral ligament; PB, posterior band of inferior glenohumeral ligament; PC, posterior capsule; SGHL, superior glenohumeral ligament. B: In adduction and neutral rotation, the SGHL is the primary ligamentous restraint. C:
In abduction and neutral rotation, the AB and PB tighten to prevent inferior translation. (After Warner JP, Deng XH, Warren RF, et al. Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med 1992;20:677, 682-683.) |
the superior glenohumeral ligament, and the coracohumeral ligament. The
middle glenohumeral ligament, which has a great deal of anatomic
variability in the anterosuperior quadrant of the joint, may
occasionally form part of the rotator interval. Below the rotator
interval, the anterior band of the inferior glenohumeral ligament
originates from the inferior labrum at the level from midglenoid.
Additional detailed anatomy and the specific functions of these
ligaments are discussed further under the section on static stability.
interval laterally and travels in the bicipital (intertubercular)
groove, which is covered by the transverse humeral ligament. The
location
of the bicipital groove may be identified by positioning the shoulder
with the elbow at the side and the forearm internally rotated
approximately 10 degrees. The long head of the biceps should then lie
directly anterior and be palpable between the two tuberosities.
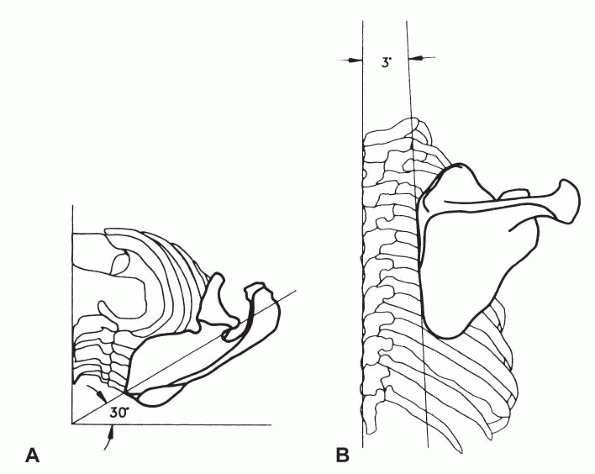
and muscular attachments to the chest wall. It lies on the
posterolateral aspect of the thorax between the second and seventh ribs
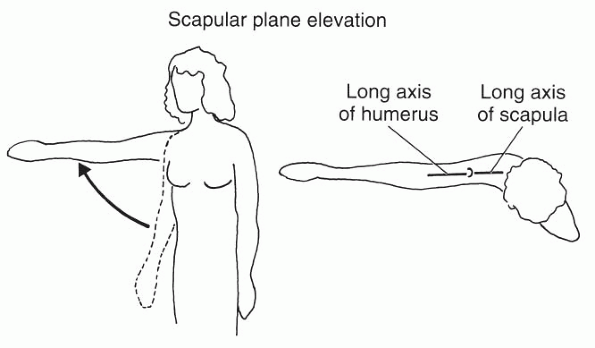
and is angled 30 degrees anterior to the coronal plane of the thorax (Fig. 14-7).
In the resting position, the scapula has a slight rotation of the
superior border toward the midline of approximately 3 degrees. When
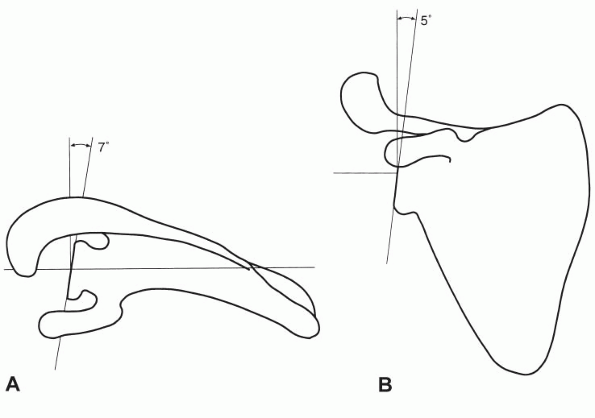
referenced to the medial border of the scapula, the glenoid has a
slight upward tilt of approximately 5 degrees. The glenoid fossa is
retroverted, compared with the scapular plane an average of 7 degrees,
although there is sizeable variation among individuals (Fig. 14-8).
the origin of all the rotator cuff muscles. The serratus anterior,
which helps to stabilize the scapula against the chest wall and thus to
prevent “scapular winging,” attaches to the medial undersurface of the
scapula and lies just anterior to the subscapularis. These two muscles
glide along one another with scapulothoracic movement. The rhomboids
and levator scapulae attach along the medial border of the scapula and
assist with elevation. Superiorly, the deltoid and trapezius attach to
the scapular spine and acromion process.
relatively flat surface. However, the articular cartilage is thicker
peripherally than it is centrally, which increases the depth of the
glenoid. In addition, the glenoid is surrounded by a fibrocartilaginous
rim called the labrum (Fig. 14-9).
As a result, the humeral head and glenoid are, in fact, quite
congruent. The radius of curvature for the glenoid is only slightly
larger than that of the humeral head. In 88% of cases, the radius of
curvature of the glenoid is no more than 2 mm greater than that of the
humeral head, and all cases will have less than a 3-mm mismatch.
 |
|
Figure 14-7 Scapular orientation on the chest wall demonstrating the scapular plane angled 30 degrees from the coronal plane (A) and with 3 degrees rotation toward the midline (B).
(From Itoi E, Morrey BF, An KN. Biomechanics of the shoulder. In: Rockwood CA, Matsen FA, Wirth MA, et al., eds. The Shoulder, 3rd ed. Philadelphia: Saunders-Elsevier, 2004:231.) |
as an outer layer consisting of the deltoid and pectoralis major
muscles, an inner layer consisting of the rotator cuff muscles
(subscapularis, supraspinatus, infraspinatus, and teres minor), and the
scapular stabilizing muscles (trapezius, levator scapulae, rhomboids,
and serratus anterior).
contour and is composed of the anterior, middle, and posterior
heads—all of which insert into the deltoid tuberosity on the
anterolateral aspect of the humerus. The origin of the deltoid is from
the anterior lateral third of the clavicle, the lateral acromion, and
the posteromedial scapular spine. The anterior head acts as a strong
flexor and internal rotator of the humerus, the middle head as an
abductor, and the posterior head as an extensor and external rotator.
and is composed of two heads: the clavicular head originating from the
medial two thirds of the clavicle and the sternocostal head originating
from the sternum, manubrium, and the upper costal cartilages. The two
heads converge at the sternoclavicular joint. The pectoralis major
insertion lies just anterior to the long head of the biceps and the
intertubercular groove. The prime function of the pectoralis major is
to adduct and internally rotate the humerus. The clavicular head also
serves as a forward elevator of the humerus, whereas the sternocostal
head extends the humerus. Beneath the outer layer of deltoid and
pectoralis lies the rotator cuff musculature, which is discussed in the
previous section.
and the thoracic vertebra and plays a critical role in scapular motion.
The uppermost fibers insert into the lateral third of the clavicle, the
middle fibers insert into medial margin of the acromion the spine of
the scapula, and the inferior fibers converge near the medial margin of
the scapular spine. Deep to the trapezius lies the levator scapulae and
the rhomboid major and minor. The levator attaches to the vertebral
border of the scapula just above the level of the scapular spine, and
the rhomboids attach just below the scapular spine.
to scapular motion. It originates from digitations of the outer upper
eight or nine ribs and runs along the chest wall toward the scapula.
The serratus inserts along the full length of the vertebral border of
the scapula.
but rather consists of a series of bursae to permit muscles to glide
past one another. The largest and most consistent bursa is the
scapulothoracic bursa located between the serratus anterior and the rib
cage. Another large bursa, although not always present, is the
subscapularis bursa between the subscapularis and the serratus. A
consistent, well-defined bursal structure is also present between the
superomedial
angle of the scapula and the undersurface of the trapezius. Finally, a
less consistently observed bursa may sometimes be located between the
inferior angle of the scapula and the latissimus dorsi.
 |
|
Figure 14-8 A: The glenoid fossa is retroverted approximately 7 degrees with respect to the scapular plane. B:
When referenced to the medial border of the scapula, there is a slight superior tilt to the glenoid of approximately 5 degrees. (From Simon SR, Alaranta H, An KN, et al. Kinesiology. In: Buckwalter JA, Einhorn TA, Simon SR. Orthopaedic Basic Science. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2000:737.) |
motion of the shoulder complex, coordinated activity of the
acromioclavicular, sternoclavicular, and scapulothoracic articulations
is vital to the overall function of the shoulder complex. To help
understand the function of the shoulder girdle musculature, Jobe and
Pink have categorized the shoulder girdle muscles into the glenohumeral
protectors, humeral positioners, scapular pivoters, and the propeller
muscles. The rotator cuff muscles are the glenohumeral protectors and
primarily function to provide dynamic joint stability. The humeral
positioners are composed of the three parts of the deltoid and serve as
the prime mover of the glenohumeral joint. The scapular pivoters
consist of the serratus anterior, the trapezius, the rhomboids, and the
levator scapulae. The pivoter muscles all function to position the
glenoid in space for optimal glenohumeral function. Finally, the
propellers are made up of the pectoralis major and the latissimus
dorsi. The propeller muscles do not attach to the scapula; rather, they
run from the torso to the humerus. They assist in transferring energy
from the trunk and lower extremities during throwing activities and
also serve as powerful interval rotators and adductors.
 |
|
Figure 14-9 A:
The glenoid labrum attached to the underlying bony glenoid and is continuous with the anchor of the tendon of the long head of the biceps. B: In cross section, the labrum has a triangular configuration and helps to deepen the glenoid, thereby, increasing stability of the glenohumeral joint. (From Della Valle CJ, Rokito AS, Gallagher Birdzell M, et al. Biomechanics of the shoulder. In: Nordin M, Frankel VH, eds. Basic Biomechanics of the Musculoskeletal System. Baltimore: Lippincott Williams & Wilkins, 2001:324.) |
 |
|
Figure 14-10
With forward elevation or abduction, synchronous rotation of the scapula occurs with an overall 2:1 ratio of glenohumeral to scapulothoracic motion. (From Simon SR, Alaranta H, An KN, et al. Kinesiology. In: Buckwalter JA, Einhorn TA, Simon SR, eds. Orthopaedic Basic Science. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2000:745.) |
difficult to assess in isolation since shoulder motion involves
contributions from the glenohumeral joint and the scapulothoracic
articulation (Fig. 14-10). Glenohumeral and
scapulothoracic kinematics are reviewed individually below, followed by
a discussion on composite shoulder motion.
glenohumeral junction functions almost as a ball-and-socket joint.
Active motion of the shoulder is also accompanied by obligate humeral
head translations that are small and usually in the range of 0 to 2 mm.
Pathology of the glenohumeral joint capsule or rotator cuff, however,
alters the normal kinematics. With asymmetric capsular contractures,
increased translations are observed in the direction opposite to the
contracture. For example, when the anterior capsule has been
overtightened following an instability procedure, increased posterior
translation of the humeral head occurs, and degenerative changes in the
joint may follow. In the case of large rotator cuff tears, excessive
superior translation may be observed because the rotator cuff can no
longer stabilize the humeral head from the upward pull of the deltoid.
glenohumeral joint, glenohumeral translations with passive range of
motion may be dramatically increased—up to 12 mm in some cases. These
higher translations may be observed in the operating room with patients
under anesthesia or in the clinical setting, when a patient can relax
their shoulder musculature.
and arm. Scapular motion is generated by the scapular pivoters
(serratus anterior, upper and lower trapezius, rhomboids, and levator
scapulae), with the primary function to position the glenoid in space
for optimal glenohumeral function. Appropriate placement of the glenoid
in space (a) assists with glenohumeral stability, (b) provides adequate
clearance of the rotator cuff tendons under the acromion to prevent
impingement, and (c) maintains deltoid tension to allow for optimal
power, regardless of arm position. The primary movements of the scapula
are elevation, depression, protraction, retraction, and rotation. As
previously noted, scapular motion is almost always coupled with
glenohumeral motion.
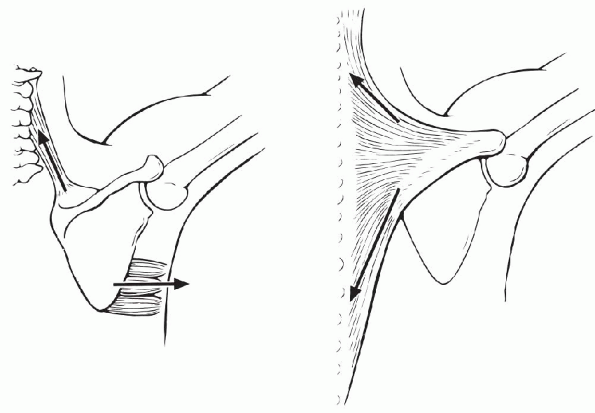
couples: muscle groups acting in opposite directions to provide
stability and control movement. In the case of scapular elevation,
rotation of the scapula occurs by synergistic contraction of the upper
trapezius, the levator scapula, and the upper serratus anterior (Fig. 14-11).
To stabilize the scapula, the force of these muscles is balanced by the
activity from the scapular depressors, the lower portions of the
trapezius, and serratus anterior.
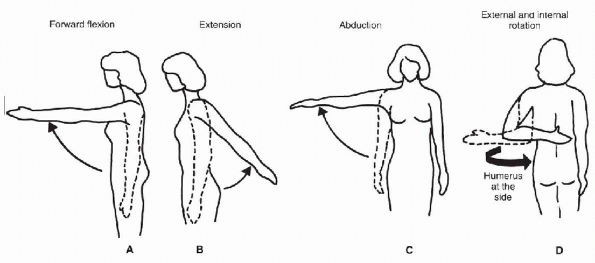
components: the glenohumeral joint and the scapulothoracic articulation
(see Fig. 14-10). Traditional assessment of
motion involved flexion in the sagittal pane, extension and abduction
in the coronal plane, and internal/external rotation (axial rotation of
the humerus with the arm held in an adducted position) (Fig. 14-12).
During most activities, however, the limb is seldom active in these
specific planes of motion. For example, abduction in the coronal plane
is limited by bony impingement of the greater tuberosity on the
acromion. Elevation in the plane of the scapula, therefore, is
considered to be a more functional measure; as in this plane, the
inferior portion of the capsule is not twisted, and the musculature of
the shoulder is optimally aligned for elevation of the arm (Fig. 14-13).
For clinical assessment of motion, the American Shoulder and Elbow
Surgeons have recommended that four planes of shoulder motion be
assessed in the clinical setting: total forward elevation, external
rotation with the elbow at the side, external rotation with the arm
abducted 90 degrees, and internal rotation behind the back.
171 degrees in women. In the first 30 degrees of elevation in the
scapular plane, motion occurs mostly at the glenohumeral joint. As the
arm is elevated further, scapulothoracic motion plays a larger role,
with an equal contribution of glenohumeral and scapulothoracic movement
in the last 60 degrees of elevation. Overall, there is a 2:1 ratio of
glenohumeral to scapulothoracic motion in elevation. Elevation of the
arm also involves a complex rotatory
motion
of the scapula, with anterior rotation during the first 90 degrees
followed by posterior rotation, with a total arc of approximately 15
degrees.
 |
|
Figure 14-11
Rotation of the scapula is generated by force couples. Synergistic contraction of the levator scapulae and serratus anterior occur, along with synergistic contraction of the upper and lower portions of the trapezius. (From Simon SR, Alaranta H, An KN, et al. Kinesiology. In: Buckwalter JA, Einhorn TA, Simon SR. Orthopaedic Basic Science. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2000:745.) |
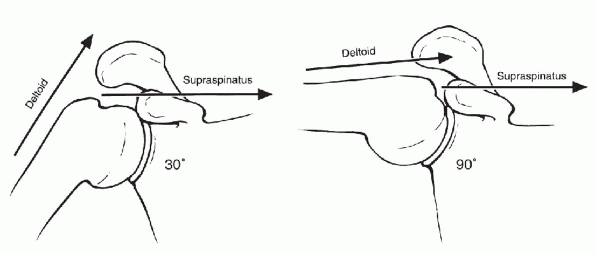
supraspinatus work synergistically to raise the arm, and
electromyographic studies have shown that both muscles are active
throughout the range of elevation. With the arm at the side in the
resting position, the line of pull of the deltoid is more vertical,
whereas the supraspinatus pulls in a more horizontal direction (Fig. 14-14).
The supraspinatus, therefore, is thought to play a larger role in
initiating abduction. As the arm is progressively elevated from the
side, the vertical or shearing component of the deltoid force is
lessened, and the direction of pull approximates that of the
supraspinatus. The combined function of the supraspinatus and deltoid
muscles has been clinically demonstrated with selective anesthetic
blocks. With an axillary nerve block and resulting deltoid paralysis,
forward elevation is possible, although it is significantly weakened.
Similarly, a suprascapular nerve block with resultant supraspinatus
paralysis has a similar effect. However,
when both the axillary and suprascapular nerves are blocked, there is a substantial loss of arm elevation.
 |
|
Figure 14-12 Traditional assessment of shoulder motion. Flexion (A) and extension (B) in the sagittal plane; abduction (C) and internal and external rotation (D).
(From Della Valle CJ, Rokito AS, Gallagher Birdzell M, et al. Biomechanics of the shoulder. In: Nordin M, Frankel VH, eds. Basic Biomechanics of the Musculoskeletal System. Baltimore: Lippincott Williams & Wilkins, 2001:320.) |
 |
|
Figure 14-13
Elevation in the scapular plane, usually approximately 30 degrees forward from the coronal plane. (From Della Valle CJ, Rokito AS, Gallagher Birdzell M, et al. Biomechanics of the shoulder. In: Nordin M, Frankel VH, eds. Basic Biomechanics of the Musculoskeletal System. Baltimore: Lippincott Williams & Wilkins, 2001:320.) |
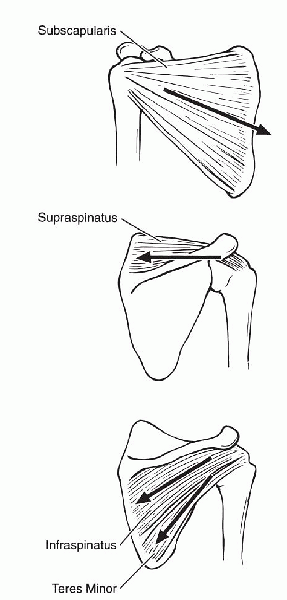
proximal humerus superiorly under the acromion, the rotator cuff
muscles are active to provide a humeral head depressor function. The
subscapularis, infraspinatus, and teres minor have an oblique
orientation that provides both a compressive force and a downward
directed force (Fig. 14-15).
muscles of the shoulder girdle have been grouped according to relative
importance with regard to elevation (Box 14-1).
shoulder is approximately 60 degrees, and the maximum range is limited
by capsular tension. The posterior and middle heads of the deltoid are
the prime movers for extension of the arm. The supraspinatus and
subscapularis are continually active throughout arm extension to
stabilize the glenohumeral joint by resisting forces tending to
dislocate
the
humerus anteriorly. The latissimus dorsi and teres major also
contribute to extension, and when the elbow is extended, the triceps
brachii may also contribute.
 |
|
Figure 14-14
In the initial phases of glenohumeral abduction, the deltoid has a more vertically oriented direction of pull, whereas the supraspinatus remains relatively constant throughout motion. (From Simon SR, Alaranta H, An KN, et al. Kinesiology. In: Buckwalter JA, Einhorn TA, Simon SR. Orthopaedic Basic Science. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2000:743.) |
 |
|
Figure 14-15
The direction of pull of the infraspinatus, teres minor, and subscapularis are in an oblique direction to provide a vertical component of humeral head depression and horizontal compressive force across the joint. The supraspinatus has a more horizontal orientation, therefore, contributing little to humeral head depression. (From Simon SR, Alaranta H, An KN, et al. Kinesiology. In: Buckwalter JA, Einhorn TA, Simon SR. Orthopaedic Basic Science. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2000:744.) |
|
Most important |
Anterior and middle thirds of the deltoid |
|
|
Inferior portion of the trapezius |
|
Supraspinatus |
|
|
Serratus anterior |
|
|
Middle portion of the trapezius |
|
|
Infraspinatus |
|
|
Long head of the biceps |
|
|
Posterior head of the deltoid |
|
|
Clavicular head of the pectoralis major |
|
|
Superior portion of the trapezius |
|
|
Sternal head of the pectoralis major |
|
|
Latissimus dorsi |
|
|
Least important |
Long head of the triceps |

shoulder with significant contributions made by the posterior deltoid
and the teres minor. With progressive shoulder abduction, the posterior
deltoid increases in efficiency as an accessory external rotator of the
humerus through improvement of its moment arm. The subscapularis is
also active but serves an antagonistic role as the main stabilizer,
preventing anterior displacement of the humeral head with external
rotation.
combined activity of the subscapularis, the sternal head of the
pectoralis major, the latissimus dorsi, and the teres major. The
subscapularis is active during all phases of internal rotation, with
relatively decreased activity toward the limits of abduction. With
increasing abduction, the activity of the sternal head of the
pectoralis major and the latissimus dorsi also decrease. The posterior
and middle heads of the deltoid compensate by increasing eccentric
activity in the abducted position.
pectoralis major, teres major, subscapularis, and latissimus dorsi,
with the latissimus dorsi being the most powerful adductor. In the
upright position, the weight of the limb also assists with adduction.
lumbar spine contributes to the ability to position the upper extremity
in space. Movement of the spine in a direction away from an extremity
attempting to reach an object enhances the attainable range of motion.
In addition, the latissimus dorsi, the pectoralis major, and the
periscapular muscles help transmit energy from the lower extremities
and trunk to the upper extremity. The spinal contribution enhances the
overall motion and function of the shoulder complex, which is of great
importance in overhead activities, such as throwing and racquet sports.
in the human body and requires contributions from both static
structures and musculotendinous activity to maintain stability. Static
restraints include the joint capsule and ligaments, the glenoid labrum,
the thicker peripheral glenoid cartilage, and a negative
intra-articular pressure. In the clinical setting of recurrent
instability, the presence of bony glenoid deficiency or humeral head
defects (e.g., Hill-Sachs lesions) also become critical factors.
Dynamic stability is achieved by the ability of the periscapular
muscles to optimally position the glenoid in space, the ability of the
rotator cuff muscles to provide stabilizing compressive forces to hold
the humeral head in joint (concavity compression), and activity from
the long head of the biceps.
one third of the diameter of the humeral head. The ability of the
glenoid to provide static stability to the glenohumeral joint stems
from the relative height of the peripheral glenoid, compared with the
central glenoid. Although the bony glenoid appears relatively flat
radiographically, the articular cartilage is thicker peripherally than
it is centrally to help increase the depth of the glenoid. The glenoid
labrum, which is a fibrocartilaginous rim, also serves to augment the
height of the peripheral glenoid by providing 50% of the overall depth
of the glenohumeral joint (see Fig. 14-9). The
labrum is triangular in cross section and has firm attachments
inferiorly to the underlying bone. In the anterosuperior portion of the
glenoid, the labrum has a more variable and looser attachment. As noted
previously, with soft tissues taken into account, the humeral head and
glenoid are in fact quite congruent, with less than 3 mm of radius of
curvature mismatch.
anteroinferior glenoid bone stock may become deficient. Clinical and
laboratory studies have suggested that, when more than 25% of the
anteroposterior diameter of the glenoid has been eroded, a soft-tissue
reconstruction alone is not sufficient and a structural bone graft is
required to achieve stability.
both directly onto the glenoid labrum anteroinferiorly and beyond the
glenoid labrum. Laterally, the capsule attaches to the anatomical neck
of the humerus. Superiorly, it is attached at the base of the coracoid
and envelops the long head of the biceps tendon, making the long head
an intra-articular structure. The surface area of the joint capsule is
twice that of the humeral head, and the average fluid volume that the
capsule can hold is approximately 15 mL in women and 20 mL in men.
Thus, there is a significant degree of inherent laxity, and this
capsular redundancy allows for a wide range of motion.
joint, portions of the capsule will tighten to limit range of motion
and provide stability. With shoulder adduction, the
capsule
is taut superiorly and lax inferiorly. Conversely, with shoulder
abduction, this relationship is reversed and the inferior capsule
tightens. With external rotation, the anterior capsule tightens, and in
internal rotation, the posterior capsule tightens. As any portion of
the shoulder capsule tightens, there is generally a small obligate
humeral head translation in a direction opposite the contracture (e.g.,
at the limit of external rotation, the anterior capsule tightens and a
posteriorly directed obligate translation occurs).
three distinct ligamentous extensions critical to shoulder stability
and function—the superior, middle, and inferior glenohumeral ligaments
(see Fig. 14-4). The superior glenohumeral
ligament originates from the anterosuperior labrum, just anterior to
the long head of the biceps, and inserts onto the upper part of the
lesser tuberosity. It is present in the majority of shoulders but is
only well developed in 50%. With the arm positioned at the side in the
resting or adducted position, the superior glenohumeral ligament is the
primary restraint to external rotation and inferior translation. The
inferior glenohumeral ligament also contributes to stability, with
abduction up to 50 degrees.
glenohumeral ligament and originates from the lateral side of the base
of the coracoid (see Fig. 14-5). It is
composed of two bands that insert above and below the long head of the
biceps on the greater and lesser tuberosities. The coracohumeral
ligament reinforces the capsule of the rotator interval between the
subscapularis and supraspinatus. In terms of static restraint, the
coracohumeral ligament has the same function as the superior
glenohumeral ligament: stability in adduction and external rotation and
resistance to inferior translation.
the superior glenohumeral ligament within the 1 to 3 o’clock position
(for a right shoulder) and inserts further inferiorly on the lesser
tuberosity. It may also originate from the anterosuperior portion of
the labrum, the supraglenoid tubercle, or the scapular neck; several
morphologic variants have also been described. Whereas the superior
glenohumeral ligament may be difficult to see at arthroscopy, the
middle glenohumeral ligament is usually seen to be crossing the
subscapularis from superomedial to inferolateral. There is great
variability in the anatomy of this structure, and it is absent in as
many as 30% of shoulders. It may be present as a cord-like variant
(Buford complex) that may be mistaken for a detached anterior labrum or
a sheet-like variant blending with the anterior band of the inferior
glenohumeral ligament. Although these anatomic variants have been
associated with increased glenohumeral internal rotation, the anatomic
variants themselves do not appear to predispose to instability.
Functionally, the middle glenohumeral ligament is the primary static
restraint in external rotation over the range of abduction from 45 to
60 degrees; however, it does demonstrate a contribution to glenohumeral
stability throughout the arc of abduction.
clinical and functional significance with regard to anterior shoulder
stability. It originates from the inferior labrum and has been shown to
have three distinct components inserting on the anatomic neck of the
humerus—an anterior band originating from 2 to 4 o’clock (right
shoulder), a posterior band originating from 7 to 9 o’clock (right
shoulder), and an intervening axillary pouch (see Fig. 14-4).
The inferior glenohumeral ligament is the primary anterior stabilizer
of the shoulder with the arm in 90 degrees of abduction. As the arm is
abducted and externally rotated, the anterior band of the inferior
glenohumeral ligament tightens and resists anterior translation. With
internal rotation of the abducted arm, the posterior band becomes taut,
and posterior translation is resisted. The inferior glenohumeral
ligament complex also serves to help resist inferior translation with
the arm in the abducted position.
an important consideration in the clinical setting of instability. In
the case of an anterior shoulder dislocation, the posterior aspect of
the humeral head may sustain an impaction fracture (Hill-Sachs lesion)
as it rests on the anteroinferior glenoid rim after dislocation. Most
humeral head lesions are small (less than 20% of the articular
surface), and capsulolabral detachments (Bankart lesions) are the most
likely causes of recurrent instability in these cases. However, even
when the capsulolabral detachments have been repaired, instability may
still be problematic with larger humeral head lesions. In these cases,
the rotational arc length of the humeral head has now been effectively
shortened, with no change to the capsule length. As the shoulder is
externally rotated, the posterior humeral head defect may then engage
the glenoid rim before the capsule tightens to limit the range of
motion, and dislocation follows.
after posterior dislocations. The posterior glenoid rim, in these
cases, creates an impaction fracture of the anterior humeral head
(reverse Hill-Sachs or McLaughlin lesion). With larger defects (less
than 20% of the articular surface), forward flexion and internal
rotation may allow the humeral head defect to engage the posterior
glenoid rim, leading to recurrent posterior dislocation.
less than 1 mL of fluid. The synovial fluid adheres to the articular
cartilage overlying the glenoid and proximal humerus and lubricates the
joint. Cohesive and adhesive forces are present within this lubricating
layer, adding some stability to the joint by making it difficult to
pull the two articular surfaces apart. The contributions of these
cohesive and adhesive forces, however, are relatively small.
glenohumeral joint is lower than atmospheric, resulting in the
so-called negative intra-articular pressure. This relatively lower
joint pressure pulls the overlying capsule and glenohumeral ligaments
inward and adds to joint stability. This stabilizing effect will be
lost when the intra-articular pressure rises to, or exceeds, the
ambient pressure, as occurs with joint effusions or hemarthroses. The
intra-articular pressure will also increase if the joint is vented by
any capsular injury, leading to increases in glenohumeral translation.
shown to have a significant effect on increasing glenohumeral
translation. However, the compressive forces generated by active
rotator cuff muscles will decrease the allowed
glenohumeral translation and are ultimately more important for joint stability.
to shoulder motion, the primary function of the rotator cuff is to
stabilize the glenohumeral joint. This stability is achieved through
compressive forces generated to hold the humeral head in the
glenohumeral joint (“concavity compression”) and assists with muscular
balance during coordinated shoulder movement.
rotator cuff muscles are active to stabilize the glenohumeral joint.
Because of the inherent lack of bony stability in the glenohumeral
joint, the force generated by one muscle requires the activation of an
antagonistic muscle, so that a dislocating force does not result. For
example, with active internal rotation of the shoulder, forces from the
subscapularis and pectoralis will tend to pull the humeral head out
anteriorly. The infraspinatus and teres minor are, therefore, also
active to help stabilize the glenohumeral joint. The antagonist muscles
(the infraspinatus and teres minor in this example) usually provide
stability via an eccentric contraction whereby the muscle is lengthened
while actively contracting. The antagonist may also act by producing a
neutralizing force of equal magnitude, but opposite in direction, as in
the case of the periscapular muscles stabilizing the scapula.
have functions of providing both shoulder motion and glenohumeral
stability. These cuff muscles all have a more oblique orientation
compared with the supraspinatus (see Fig. 14-15).
The subscapularis and infraspinatus are inferiorly directed
approximately 45 degrees and the teres minor approximately 55 degrees.
The oblique orientation of the infraspinatus, teres minor, and
subscapularis thus provide both compression and a downward directed
force (see Fig. 14-15), whereas the horizontally oriented supraspinatus strictly provides a compressive force (see Fig. 14-14).
The subscapularis, along with the middle and inferior glenohumeral
ligaments, has also been shown to act as an important anterior
stabilizer of the glenohumeral joint, particularly with the arm held at
45 degrees of abduction.
glenohumeral joint but has little humeral head depressor function to
counteract the tendency for the deltoid to sublux the proximal humerus
superiorly under the acromion.
but inserts on the humerus below the surgical neck, posterior to the
intertubercular groove, and is not part of the rotator cuff. It
functions to assist with arm adduction and internal rotation and does
not contribute to glenohumeral stability.
is a useful tool to assess the clinical presentation of rotator cuff
pathology. In cases of massive rotator cuff tears with involvement of
the supraspinatus, infraspinatus, and subscapularis, the patient is
frequently unable to achieve any functional elevation. As the deltoid
activates to elevate the arm, the antagonist action of the
infraspinatus and subscapularis are too weak to keep the humeral head
centered. As a result, the humeral head migrates superiorly and comes
into contact with the acromion.
head, which originates from the tip of the coracoid process, and a long
head, which originates from the superior glenoid labrum and
supraglenoid tubercle. Although the primary function of the biceps
muscle is to supinate the forearm and flex the elbow, the long head
plays an additional role in shoulder stability. The clinical importance
of the long head of the biceps tendon, however, has been controversial
in the nonathlete population.
been demonstrated to be an important static restraint to
anterior-superior instability. Recently, however, the contribution of
the biceps to shoulder function has been questioned. When
electromyography has been used to measure biceps activity during active
shoulder motion but with the elbow held fixed in a brace, negligible
biceps activity was demonstrated. However, almost any purposeful
movement of the upper extremity would require both active elbow and
shoulder motion, and it is unclear to what extent biceps activity
contributes to shoulder stability with combined shoulder and elbow
movement.
debate as to the importance of the biceps tendon. When the long head of
the biceps is loaded in cadaveric models, decreased anterior humeral
head translations are observed with the shoulder in a position of 90
degrees of abduction and 60 to 90 degrees of external rotation. The
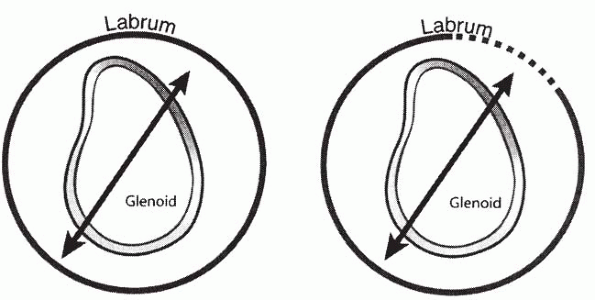
biceps anchor and superior labrum may become detached as a result of
trauma or stress, producing an injury to the superior labrum anterior
and posterior (SLAP) lesion. In cadaveric models, the creation of a
SLAP lesion resulted in an increased strain on the anterosuperior band
of the inferior glenohumeral ligament of between 102% and 120%, with
the shoulder in abduction and external rotation. When an anterior load
is applied to a cadaveric shoulder with an induced SLAP lesion,
increases in both the anterior and inferior translations have been
observed. This has been described as a “circle concept” in which the
increase in humeral head translation, or “pseudolaxity,” occurs as a
result of injury to the posterosuperior labrum (Fig. 14-16).
motion, the scapula provides a stable socket for the articulation of
the humeral head. As the extremity is positioned in space, the
periscapular muscles are active to position the glenoid optimally in
space. This permits maximizing the rotator cuff compressive forces and
glenohumeral joint stability.
activities represent a complex biomechanical problem. Although the
descriptive anatomy of a joint may be readily understood, a true
understanding of joint forces is a challenging three-dimensional
spatial
problem requiring knowledge of limb position, kinematics, applied
loads, and the activity level of each muscle crossing the joint.
 |
|
Figure 14-16
“Circle concept of instability,” demonstrating how disruption of the labral attachment on one side of the glenoid may create laxity on the opposite side of the ring. (From Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology. Part I: pathoanatomy and biomechanics. Arthroscopy 2003;19:417.) |
on the force generated by the muscle and the moment arm (or lever arm).
The moment arm is defined as a perpendicular line from the center of
rotation of the joint to the line of action of a force. The resultant
moment is then calculated as the product of the force and the moment
arm. Note that in biomechanics, the term moment
is usually used to characterize bending across a long bone or joint in
a direction other than along the axis of a long bone. The term torque
is used to describe a rotational moment acting along the axis of a
bone. In either case, bending moments and torques are equivalent
concepts and calculated in the same manner.
first to consider the joint in a stationary, or static, position, while
simplifying the anatomy and geometry. A free-body diagram is then
constructed and a force balance carried out. When the limb is not
accelerating, the sum of all forces at any point must be equal to zero,
and the sum of all moments at any point must also be equal to zero.
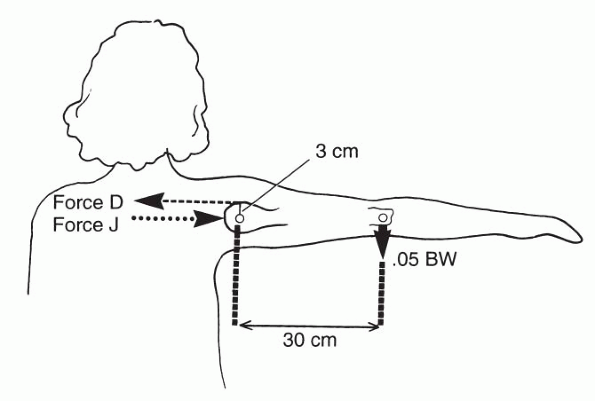
degrees, where we are interested in estimating the force of pull of the
deltoid muscle and the glenohumeral joint reaction force. In this
example, we will ignore the contribution of the rotator cuff muscles,
which would normally be active to help stabilize the humeral head. The
analysis begins with a free-body diagram. The extremity is modeled with
the glenoid removed from the diagram and replaced by the joint reaction
force, J (Fig. 14-17). Similarly, the deltoid
is replaced by the force of the deltoid muscle, D, which will be
modeled approximately parallel to the arm in the position of 90 degrees
of abduction. The perpendicular distance from the force, D, to the
center of rotation of the humeral head is taken as 3 cm. We will assume
that only the deltoid is active, and no other muscle forces will be
considered. The weight of the arm will be estimated to be 0.05 times
body weight (BW), and the center of gravity of the limb as 30 cm from
the center of rotation of the shoulder. The final free-body diagram is
shown in Figure 14-17.
solved using equilibrium equations. Because the arm is not
accelerating, the sum of all forces in any direction must be equal to
zero, and the sum of all moments about any point must be equal to zero.
We will use the convention that moments acting in a counterclockwise
direction are positive, and moments in a clockwise direction are
negative. Therefore,
 |
|
Figure 14-17
Free-body diagram of the static shoulder in 90 degrees of abduction. (From Della Valle CJ, Rokito AS, Gallagher Birdzell M, et al. Biomechanics of the shoulder. In: Nordin M, Frankel VH, eds. Basic Biomechanics of the Musculoskeletal System. Baltimore: Lippincott Williams & Wilkins, 2001:337.) |
principle that the sum of all forces in any direction must be equal to
zero. If the direction to the left is taken as negative, then in the
horizontal direction:
deltoid force are essentially equal and opposite forces. This simple
analysis highlights the very high loads transmitted to the relatively
small glenoid (J): a force of one half of body weight with the arm
simply held out to the side. Loads will increase when a mass is held in
the hand a known distance from the shoulder. With an object held in the
hand, the analysis can be repeated by including the moment and weight
generated by the additional mass.
predicting the loads that a musculotendinous unit must generate to
support a given limb position and applied load. The analysis does not
address the physiologic ability of a muscle to produce the required
force, nor does it consider the maximum joint forces based on the
muscles maximum strength. Knowing the muscle cross-sectional area, an
estimate of
the
maximum muscle forces may be made. Maximal muscle force is dependent on
muscle pretension, and estimates from the literature provide a broad
range of results that are usually in the range from 4 to 9 kg/cm2 (57
to 128 lb/in2).
During windup, the pitcher places the body in a position to optimize
the contribution of all parts of the body toward accelerating the ball.
Approximately 50% of the velocity of the overhand throw results from
the forward step of the stride leg and the body rotation. The remainder
of the ball propulsion is generated from the shoulder, elbow, and
wrist. In the windup phase, shoulder muscle activity is low, and few
injuries occur during this phase.
muscle show moderate-to-high activity as these muscles protract and
upwardly rotate the scapula. The scapular positioning places the
glenoid in proper position to avoid the occurrence of impingement and
instability. The middle deltoid achieves peak activity during the early
cocking phase, and the supraspinatus is active to help stabilize the
humeral head. Once the humerus is abducted beyond 90 degrees, humeral
head translation is limited by the inferior glenohumeral ligament.
160 to 185 degrees in professional pitchers. As the anterior capsule
tightens in abduction and external rotation, an obligate posterior
glenohumeral translation occurs. The scapular protractor (serratus
anterior) and the retractors (middle trapezius, rhomboids, and levator
scapulae) are all active to support a stable base for rapid humeral
external rotation. The long head of the biceps compresses the humeral
head into the glenoid and contributes to anterior stability. The
activity of the deltoid diminishes in late cocking, and the rotator
cuff muscles become more active. In particular, the teres minor and
infraspinatus are primarily responsible for the extreme external
rotation. The supraspinatus becomes oriented more posteriorly and
becomes less effective in providing a stabilizing superior compressive
force. The end of late cocking occurs as the pectoralis major,
latissimus dorsi, and serratus anterior muscles show increased activity
to generate maximum horizontal adduction.
 |
|
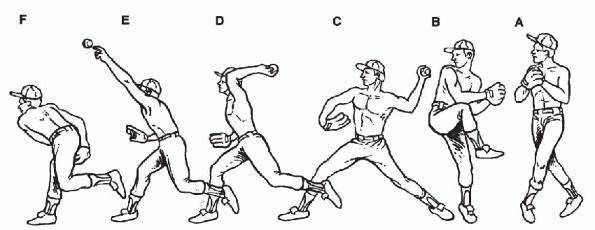
Figure 14-18 The six phases of the pitching motion. A,B: Windup begins when the pitcher initiates motion and ends when the ball is removed from the glove. C:
The stride leg extends toward the batter, and the knee and hip of the pivot leg extend to propel the body forward into the stride. D: In late cocking, the trunk rotates forward while the shoulder achieves a position of maximum external rotation. E: The shoulder is rapidly internally rotated during the acceleration phase. F: After ball release, deceleration forces are applied to the shoulder as it continues to internally rotate. Deceleration is complete when the arm reaches a position of 0 degrees internal rotation. The arm is then adducted across the body in follow-through phase. (From Park SS, Loebenberg ML, Rokito AS, et al. The shoulder in baseball pitching. Biomechanics and related injuries. Bull Hosp Joint Dis 2002-2003;61:81.) |
shoulder is rapidly internally rotated during the acceleration phase,
over a period of 42 to 58 ms in professional players. All scapular
muscles remain active to stabilize the scapula during this phase. The
latissimus dorsi and the pectoralis major are the primary muscles
contributing to the acceleration of the ball, with the latissimus
showing the highest activity and oriented anatomically to provide the
greatest torque. Energy is also transferred from the lower extremities
and the rotation of the trunk. The subscapularis, teres minor, and
infraspinatus remain active to stabilize the glenohumeral joint. The
acceleration phase is terminated when the ball is released, and the arm
then undergoes deceleration and follow-through.
the residual kinetic energy in the limb after the ball is released. It
has been recognized as the most violent phase of throwing, whereby the
shoulder continues its internal rotation while opposing muscles around
the shoulder activate simultaneously to control deceleration. The teres
minor contracts eccentrically and demonstrates the highest level of
activity of all the cuff muscles, whereas the subscapularis also
remains active to stabilize the humeral head. The middle and posterior
heads of the deltoid are active to decelerate
the
arm. It was initially proposed that labral injuries occurred most
commonly in the deceleration phase; however, recent studies have
demonstrated that labral injuries may more commonly occur in the
acceleration phase.
less active as the body essentially catches up to the throwing arm. The
shoulder adducts and the elbow flexes with all shoulder and upper
extremity muscles showing low-to-moderate electromyographic activity.
challenges of shoulder anatomy and biomechanics. For optimal shoulder
girdle function, coordinated activity of the glenohumeral joint, the
scapulothoracic articulation, the acromioclavicular joint, and the
sternoclavicular joint is essential. Both static and dynamic
stabilizers play critical roles in preventing instability and injury.
However, when the shoulder is afflicted by trauma or chronic disease,
an understanding of shoulder anatomy and biomechanics enables the
physician to prescribe an effective course of treatment and
rehabilitation.
AC, Debski RE. Anatomy and function of the glenohumeral ligaments in
anterior shoulder instability. Clin Orthop Relat Res 2002;400:32-39,
AM, O’Driscoll SW, Heers G, et al. Biomechanical comparison of effects
of supraspinatus tendon detachments, tendon defects, and muscle
retractions. J Bone Joint Surg Am 2002;84:780-785.
E, Morrey BF, An KN. Biomechanics of the shoulder. In: Rockwood CA Jr,
Matsen FA III, Wirth MA, et al., eds. The Shoulder, 3rd ed.
Philadelphia: Saunders-Elsevier, 2004:223-267.
CM, Coen MJ. Gross anatomy of the shoulder. In: Rockwood CA Jr, Matsen
FA III, Wirth MA, et al., eds. The Shoulder, 3rd ed. Philadelphia:
Saunders-Elsevier, 2004:33-95.
FW, Pink M. Classification and treatment of shoulder dysfunction in the
overhead athlete. J Orthop Sports Phys Ther 1993;18: 427-432.
K. Injuries to the shoulder in the throwing athlete. Part one:
Biomechanics/pathophysiology/classification of injury. Am J Sports Med
2000;28:265-275.
LA, McClure PW, Karduna AR. Anatomical and biomechanical mechanisms of
subacromial impingement syndrome. Clin Biomech 2003;18:369-379.
AG, Kim TK, Chronopoulos E, et al. Anatomical variants in the
anterosuperior aspect of the glenoid labrum: a statistical analysis of
seventy-three cases. J Bone Joint Surg Am 2003;85:653-659.
KJ, Wright TW. Anatomy and biomechanics of the acromioclavicular and
sternoclavicular joints. Clin Sports Med 2003;22: 219-237.
GR Jr, Shakil M, Klimkiewicz J, et al. Anatomy of the scapulothoracic
articulation. Clin Orthop Relat Res 1999;359:237-246.