
Editors: Frassica, Frank J.; Sponseller, Paul D.; Wilckens, John H.
Title: 5-Minute Orthopaedic Consult, 2nd Edition
Copyright ©2007 Lippincott Williams & Wilkins
> Table of Contents > Posterior Interosseous Nerve Entrapment
Posterior Interosseous Nerve Entrapment
Paul D. Sponseller MD
Dawn M. LaPorte MD
Description
-
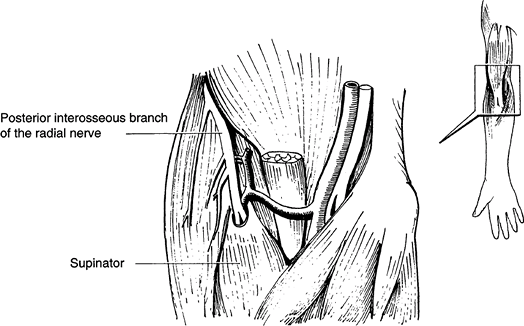
PINS occurs when muscles innervated by
the posterior interosseous nerve are affected secondary to entrapment
of the posterior interosseous nerve by 1 of several structures (Fig. 1). -
The related, but separate, radial tunnel
syndrome is characterized by pain and weakness on the lateral side of
the elbow after activities with forceful elbow extension or forearm
rotation.
Epidemiology
-
Most common in individuals 20–50 years old
-
Male and females are affected approximately equally.
Incidence
Uncommon
Risk Factors
Repetitive supinating or gripping motions are risk factors.
Genetics
No Mendelian pattern is known.
Etiology
-
Typically, involvement of ≥1 of the following structures:
-
Fibrous edge of the supinator muscle (most common cause), known as the “arcade of Frohse”
-
Fibrous bands over the radial head
-
Radial recurrent vessels to the elbow, known as the “leash of Henry”
-
Fibrous edge of the extensor radialis brevis muscle
-
Distal edge of the supinator (1)
-
Associated Conditions
Lateral epicondylitis
 |
|
Fig. 1. The posterior interosseous branch of the radial nerve may become entrapped in the arcade around the supinator muscle.
|
Signs and Symptoms
-
Aching pain in the muscles of the lateral forearm, just distal to the elbow (the extensor-supinator mass)
-
Symptoms usually occur after muscular effort.
-
Numbness is rare in PINS because the course of the sensory nerve is separate from that of the motor nerve.
Physical Exam
-
Complete neurovascular examination of the affected limb:
-
The area of tenderness in PINS is ~4 fingerbreadths distal to the lateral epicondyle of the elbow.
-
Pain is worsened by active supination of the forearm (turning the palm up) or extension of the wrist.
-
Pain is worsened by pressing down on the extended long finger.
-
Sensation of the forearm and hand is normal.
-
Motor strength may be diminished in chronic cases because of longstanding compression.
-
-
Diagnostic local anesthetic injection:
-
Inject local anesthetic into the
extensor-supinator mass and lateral side of the elbow, on separate
days, to determine where pain relief occurs.
-
Tests
Lab
Laboratory tests are not helpful for this diagnosis.
Imaging
Imaging studies are not needed unless an unusual mass is felt in the area.
Pathological Findings
-
On surgical exploration, compression of the radial nerve
-
Nerve possibly having constricted area from long-standing pressure
Differential Diagnosis
-
Lateral epicondylitis (tennis elbow):
Usually a more proximal pain, directly over the lateral epicondyle or
radial head (i.e., over the elbow itself) -
Cervical radiculopathy (nerve compression in the neck): Usually associated with a more radiating pain
-
Cheiralgia paresthetica (Wartenberg symptom): Entrapment of the radial sensory nerve, producing numbness
P.341
General Measures
-
Rest from the causative activity, if one can be identified
-
If no cause identified, immobilization of the elbow and forearm in a splint
-
Surgery if nonoperative measures are not successful
-
After nonoperative or surgical cure, slow resumption of activity
-
Repetitive supination or gripping activities limited to the extent that they do not cause discomfort
Special Therapy
Physical Therapy
-
Occupational therapy for gradual mobilization and strengthening of the elbow is begun when the splint is removed.
-
Therapy should be performed by an experienced hand therapist.
Medication
NSAIDs
Surgery
-
Surgical exploration of the path of the posterior interosseous nerve in this region, which may be an outpatient procedure (2)
-
Release of constricting structures
-
Usually satisfactory results
-
No permanent deficit resulting from release
Prognosis
-
Most patients have a good result after nonoperative or surgical cure.
-
Causative activities should be modified or eliminated, if possible.
Complications
Recurrence is possible.
Patient Monitoring
Patients are followed every 3 months until the symptoms resolve.
References
1. Gupta R. Nerve. In: Beredjiklian PK, Bozentka DJ, eds. Review of Hand Surgery. Philadelphia: WB Saunders, 2004:79–100.
2. Arle JE, Zager EL. Surgical treatment of common entrapment neuropathies in the upper limbs. Muscle Nerve 2000;23:1160–1174.
Additional Reading
Lister GD, Belsole RB, Kleinert HE. The radial tunnel syndrome. J Hand Surg 1979;4A:52–59.
MacKinnon SE, Novak CB. Compression neuropathies. In: Green DP, Hotchkiss RN, Pederson WC, et al., eds. Green’s Operative Hand Surgery, 5th ed. Philadelphia: Elsevier Churchill Livingstone, 2005;999–1045.
Codes
ICD9-CM
723.4 Brachial neuritis or radiculitis not otherwise specified
Patient Teaching
-
Demonstrate motions that constrict the nerve.
-
Explain the dosing and side effects of analgesics.
-
Explain that changing manual jobs or repetitive motions may prevent the development of full-blown PINS.
FAQ
Q: How do patients with PINS present?
A: Patients present with pain at the proximal lateral forearm and weakness in the extensor muscles of the digits and wrist.
Q: Is radial tunnel syndrome different from PINS entrapment?
A:
Yes. Radial tunnel syndrome affects only the sensory component of the
radial nerve, and patients present with pain but not motor weakness.
Yes. Radial tunnel syndrome affects only the sensory component of the
radial nerve, and patients present with pain but not motor weakness.