
Editors: Chelly, Jacques E.
Title: Peripheral Nerve Blocks: A Color Atlas, 3rd Edition
Copyright ©2009 Lippincott Williams & Wilkins
> Table of Contents > Section VII – Pain Blocks > 70 – Sacroiliac Joint Injection
70
Sacroiliac Joint Injection
Nashaat N. Rizk
Albert J. Carvelli
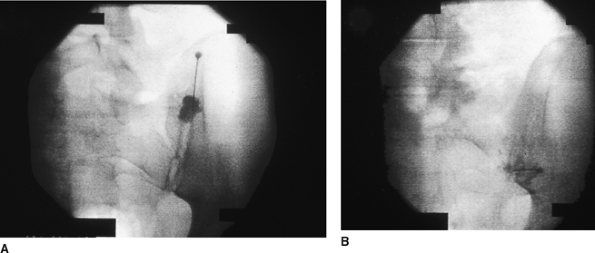
To gain access to this joint space, the fluoroscopic beam must be
rotated approximately 15° to 30° to the opposite side of the joint to
locate the posterior face of the sacroiliac joint, and then 20° to 30°
cephalad and caudad (Ferguson view; Fig. 70-1B).
Two separate injections can be performed. The first injection is aimed
at the inferior one-third of the joint. Accordingly, the 22-gauge
spinal needle is aimed in the same direction as the fluoroscopic beam
to gain access to the joint. A loss of resistance is often felt as the
joint space is entered. Next, the superior one-third of the joint space
is entered in a similar fashion. To help confirm the joint space
location, 0.5 to 1.0 mL of contrast dye can be injected prior to the
injection of the local anesthetic mixture.
-
The feeling of a “pop” or loss of
resistance when advancing the needle can be misleading. The joint space
itself can be difficult to enter with the needle. Always reconfirm the
correct positioning of the needle with fluoroscopy.
P.451
 |
|
Figure 70-1. A: Anteroposterior view. B: Ferguson view.
|
Suggested Readings
Kransdorf MJ. Sacroiliac joint injection. In: Fenton DS, Czervionke LF, eds. Image-guided spine intervention. Philadelphia: WB Saunders, 2003.
Manning DC, Rowlingson JC. Back pain and the role of neural blockade. In: Cousins MJ, Bridenbaugh PO, eds. Neural blockade in clinical anesthesia and management of pain, 3rd ed. Philadelphia: Lippincott-Raven, 1998.