
Editors: Frassica, Frank J.; Sponseller, Paul D.; Wilckens, John H.
Title: 5-Minute Orthopaedic Consult, 2nd Edition
Copyright ©2007 Lippincott Williams & Wilkins
> Table of Contents > Nursemaid’s Elbow
Nursemaid’s Elbow
Paul D. Sponseller MD
Description
-
Nursemaid’s elbow results from injury to the annular ligament that surrounds the radial head at the elbow in a young child (Fig. 1).
-
The injury causes guarding and failure to use the elbow.
-
It is not a subluxation or dislocation.
-
Synonyms: Pulled elbow; Annular ligament entrapment
General Prevention
Care should be taken to avoid traction on the arm of a young child.
Epidemiology
-
It usually affects children 1–5 years old (1).
-
Boys and girls are affected equally.
Incidence
This is 1 of the most common elbow injuries in young children.
Risk Factors
-
Ages 1–5 years
-
Stubborn behavior (pulling away)
Genetics
No genetic predisposition is known.
Etiology
-
With traction, a small part of the
annular ligament that surrounds the radial head is pulled toward the
joint and may be partially torn, causing painful rotation of the radius. -
This injury usually does not result from
a fall on the outstretched hand, which typically produces a buckle
fracture of the distal radius or an elbow injury.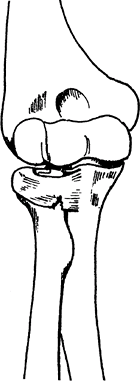 Fig. 1. Nursemaid’s elbow is a strain or a tear in the annular ligament around the radial neck.
Fig. 1. Nursemaid’s elbow is a strain or a tear in the annular ligament around the radial neck.
Signs and Symptoms
-
Pain in the elbow after a traction injury, such as pulling on the arm by a parent or sibling (Fig. 2)
-
Usually, minimal pain to palpation
-
No substantial swelling
-
Resistance by the patient to use the elbow
-
The response to reduction of the
displaced ligament is the most diagnostic feature of all: The child
starts using the elbow again shortly, and no residual tenderness is
present.
Physical Exam
The child usually holds the elbow at the side and refuses to use the extremity.
Tests
Lab
No laboratory tests aid in the diagnosis.
Imaging
-
Radiographs are not required if the diagnosis is clear.
-
If in doubt, order AP and lateral films of the elbow to rule out fracture.
-
If it is a true nursemaid’s elbow, the radiograph should be normal.
Pathological Findings
-
The ligament surrounding the radial head is partially, but not totally, torn.
-
Few specimens have been examined because the natural history of the condition is benign.
Differential Diagnosis
-
Buckle or greenstick fracture of the distal humerus
-
Growth plate injury of the distal humerus or proximal radius
-
Infection, juvenile rheumatoid arthritis,
and Lyme disease, which are all possibilities but which occur much less
frequently than nursemaid’s elbow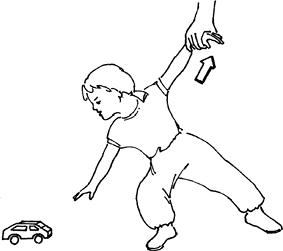 Fig. 2. The mechanism of nursemaid’s elbow is traction, not a fall.
Fig. 2. The mechanism of nursemaid’s elbow is traction, not a fall.
General Measures
-
Rule out other conditions (usually by physical examination).
-
Reduce the displaced annular ligament by
flexing the child’s elbow fully, bringing the child’s hand up to touch
the shoulder, while supinating the forearm (Fig. 3).-
Usually, no sedation is needed.
-
A slight “pop” often is felt.
-
The maneuver may be resisted initially by the child, but then the child begins to use the arm again.
-
-
A sling or splint usually is not needed unless the episode is a recurrence.
Activity
The child should be allowed to return to activities as tolerated.
Special Therapy
Physical Therapy
In children in this age group, physical therapy is not needed for this injury.
Medication
-
Medications usually are not needed once the injury is reduced, but acetaminophen may be given.
-
If stronger medication is needed, suspect another diagnosis.
Surgery
-
Not needed
-
Closed manipulation is always successful.
 Fig. 3. Nursemaid’s elbow usually is reduced by flexion and supination.
Fig. 3. Nursemaid’s elbow usually is reduced by flexion and supination.
P.279
Prognosis
-
The prognosis usually is excellent; there should be no sequelae.
-
A few children suffer a recurrence, which can be reduced and splinted for 1–2 weeks.
-
Sometimes several recurrences may happen within a year, but the child will eventually “grow out” of this predisposition.
Complications
-
None are known, except misdiagnosis, such as missing a fracture about the elbow.
-
This condition can be distinguished from a fracture by the latter’s different mechanism and greater swelling and tenderness.
Patient Monitoring
Monitoring is not needed unless problems persist.
References
1. Sponseller
PD. Disorders of bone, joint, and muscle problems. In: McMillan JA,
Feigin RD, DeAngelis CD, et al., eds. Oski’s Pediatrics: Principles and
Practice, 4th ed. Philadelphia: Lippincott Williams & Wilkins,
2006:2470–2505.
PD. Disorders of bone, joint, and muscle problems. In: McMillan JA,
Feigin RD, DeAngelis CD, et al., eds. Oski’s Pediatrics: Principles and
Practice, 4th ed. Philadelphia: Lippincott Williams & Wilkins,
2006:2470–2505.
Codes
ICD9-CM
832.0 Annular ligament disruption
Patient Teaching
-
Educate parents about the traction mechanism of the injury and the need to avoid pulling on the child’s elbow.
-
If a child has had several recurrences,
it is appropriate for a parent to learn the reduction maneuver so that
it can be handled at home.
Prevention
Avoid strong traction on the arm of a young child.
FAQ
Q: When should a radiograph be taken for a presumed nursemaid elbow?
A: When the swelling is excessive or the mechanism is atypical, such that a fracture may be suspected.