
Although cervical spine injuries outnumber thoracic and lumbar spinal
column injuries, fractures of the thoracolumbar region are certainly
not rare. The mechanisms of injury vary with age,13,58
while the classification of these injury patterns follow adult spine
fracture guidelines. These fractures can be broadly grouped as
compression, burst, flexion-distraction, and fracture-dislocations. The
treatment principles are based on the mechanism of injury and the
“stability” of the fracture
challenging, and controversy remains as to how to establish which
fractures require surgical stabilization. The status of the
neurological system is an important variable in treatment.2,21 In addition, other associated injuries are common,4 particularly with flexion-distraction “lap belt” injuries.27,32,40,44,55
Understanding the mechanism of injury, the neurologic status and
associated injuries will allow logical decision-making about the
treatment approach to a pediatric patient with thoracolumbar spinal
injury.
thoracolumbar spinal fractures is understanding the mechanism of
injury. In general, the mechanism of injury correlates with the age of
the patient.13 Spine trauma, just like appendicular trauma, should generate concern for nonaccidental injury in infants and young children.9,15,35 Levin et al.41 reported on seven unstable thoracolumbar spinal fractures in abused children.
The type of seatbelt restraint has clear implications in the mechanism
of forced transfer to the spine, with the lap belt a common cause of
both intra-abdominal and spinal injury.27,40,55,59,65
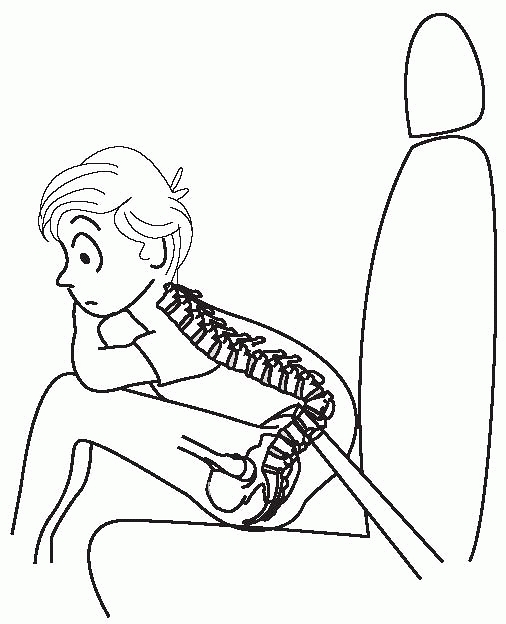
The lap belt has been long known to create hyperflexion of the trunk
over the belt with the spine pinching the intra-abdominal organs
anteriorly. The point of flexion is anterior to the spine leading to
anterior compression combined with posterior column distraction (Fig. 19-1).
Addition of a shoulder strap or child seat with a full frontal harness
limits flexion with frontal impact accidents and protects the spine
(and other parts of the body) from injury.
the spine, which may result in a “burst” fracture or wedge compression
fracture, depending on the degree of flexion of the trunk at the time
of impact. These fracture patterns are possible with any mechanism
associated with axial compression and can occur with motor vehicle
accidents and sporting injuries.13
Compression of the vertebra with the trunk flexed creates the greatest
forces in the anterior aspect of the vertebra, leading more commonly to
anterior column wedging. This is in contrast
to
the trunk in an extended position, which loads the vertebral body more
symmetrically. Fractures in this case often collapse with radial
expansion or “bursting.” Displacement of the posterior vertebral body
fragments into the spinal canal may cause injury or compression of the
neurologic elements (spinal cord or cauda equina).30
 |
|
FIGURE 19-1
A lap belt used for a child can create a point of rotation about which the spine is flexed with an abrupt stop. This is a common mechanism for creating both intra-abdominal and flexion-distraction spinal injuries. |
proportion to the force applied, the possibility of an insufficiency
fracture due to weak bone should be considered. Osteoporotic
insufficiency fractures, common in the elderly, are rare in children;
however, several disease states may predispose children to these
fractures. Steroid use frequent in the management of many pediatric
diseases often leads to osteoporosis when taken chronically.68 In addition, primary lesions of the bone, such as Langerhans histiocytosis, often affects thoracic vertebrae.3,22 Other tumors and infections warrant consideration when nontraumatic compression fractures are identified.47,56
traumatic spinal injury begins as with any serious trauma victim. The
ABCs of resuscitation are performed while maintaining cervical and
thoracolumbar spinal precautions. The frequency of spinal injuries in
the setting of major trauma (motor vehicle accident, fall, etc.) is
particularly high. After stabilizing the cardiorespiratory systems,
symptoms of pain, numbness, and tingling should be sought if the
patient is old enough and alert enough to cooperate. Pain in the back
is often not appreciated when other distracting injuries exist and the
patient is immobilized on a backboard. Examination of the back must not
be forgotten and is performed by logrolling the patient. Visual
inspection, along with palpation, should seek areas of swelling,
deformity, ecchymosis, and/or tenderness that may provide a clue to the
presence of an injury. In trauma patients, thoracolumbar fractures are
more common in older children and adolescents, and there is a low
mortality rate and infrequent need for operative stabilization.60
integrity of the spinal cord. The age of the patient may limit the
thoroughness of this assessment, but some indication of sensory and
motor function should be sought. In cases of spinal cord deficit, a
detailed examination of the strength of each muscle group, sensory
levels, and rectal tone will need to be serially compared over time and
the quality of the documentation cannot be over emphasized. The
prognosis for recovery is significantly better if the spinal cord
injury (SCI) is incomplete.10,28,71
The status of the neurologic function over time may lead to important
treatment decisions regarding the necessity and timing of surgical
intervention. A progressive neurologic deficit warrants immediate
surgical attention, while an improving status may suggest a less urgent
approach. Overall, the physical examination has a sensitivity of 87% in
identifying thoracolumbar fractures.60
of a particular injury (e.g., lap belt injury and flexion-distraction
lumbar fracture pattern), so should the presence of one injury raise
suspicion of a concomitant associated injury. First, any spinal
fracture should be considered a significant risk factor for a spinal
fracture at another level. The traumatic force required to create one
fracture is often enough to result in one or more additional fractures
at other locations. Similarly, a cervical injury is frequently
associated with closed head injury and vice versa.
flexion-distraction injuries of the spine, but also is associated with
intra-abdominal injury.55 Compressed
between the seatbelt and the spinal column, the aorta, intestinal
viscera, and abdominal wall musculature are at risk for laceration.
Abdominal injuries are present in almost 50% of pediatric patients with
Chance fractures.49 Ecchymosis on
the anterior abdomen is suggestive of intra-abdominal injury that
warrants further evaluation with laparoscopy, laparotomy, or additional
imaging by computed tomography (CT).4,65 A high index of suspicion is required, because missed injuries may be life threatening.40
significance and may be present with many fracture patterns. Disruption
of the stability of the spinal column or bony intrusion into the spinal
canal may result in compromise of neurologic function. All patients
with a known spinal column fracture or dislocation warrant a careful
neurologic examination. Overall, most pediatric patients with
thoracolumbar fractures are neurologically intact (85%), and less
commonly present with SCIs (incomplete in 5% and complete in 10%).17
Similarly, patients with a traumatic neurologic deficit require a
careful evaluation of the spinal column integrity. There are, however,
a subset of patients who present with SCI without radiographic
abnormality.50,51
This scenario has been termed SCIWORA, a phenomenon much more common in
children than adults. It is thought that the flexibility of the
immature spine allows spinal column segmental displacements great
enough to lead to SCI without mechanically disrupting the bony and/or
ligamentous elements.50 Although
these injuries may not be visible on plain radiographs, nearly all will
have some evidence of soft tissue injury of the spine on
more sensitive magnetic resonance imaging (MRI) studies.25
The term SCIWORA is less relevant in the era of routine MRI, which is
now routinely obtained in all patients with possible spinal cord injury.33
maximize the potential for recovery of spinal cord function if an SCI
was present and/or to provide skeletal stability to the spinal column
to protect against future SCI. These two goals may be analyzed
separately when both instability and SCI exist. Optimizing return of
any lost spinal cord function is paramount, and the potential for
recovery of spinal cord function in general is greater in children than
in adults.21,71
In a study from a major metropolitan trauma center, complete SCIs were
associated with fatal injuries in one third and no neurologic recovery
in another third, while most of the remaining onethird of patients made
improvements that ultimately allowed functional ambulation. Less
surprisingly, nearly all patients with incomplete SCI made some
improvement over time as well.71
This ability to recover, even from complete injuries, has led some to
suggest more aggressive attempts at spinal cord decompression in the
early course of treatment,20,52 while others have suggested a period of “spinal cord rest” with observation.42
There is certainly no controlled series of patients treated by both
approaches to support either hypothesis. The data do, however, suggest
a more optimistic view regarding the potential recovery of traumatic
SCIs in children compared with adults.
all cases of injury because the functional capacity of the vertebral
elements to protect the spinal cord will continue to be required. This
evaluation may be performed with functional radiographs, such as
flexion-extension views (much more common in the cervical spine) or
with an MRI evaluation of associated soft tissue injuries that may
coexist with more obvious bony fractures. Several methods of estimating
spinal column stability have been proposed including the three-column
concept of Denis.14 Based on
division into anterior, middle, and posterior columns, injuries to two
and certainly three of these sagittal columns may be associated with an
unstable injury pattern. Plain radiography with a CT scan is
appropriate for evaluating the bony elements. An MRI is often required
to elucidate the nature of the disc and ligamentous injuries.26,33,67
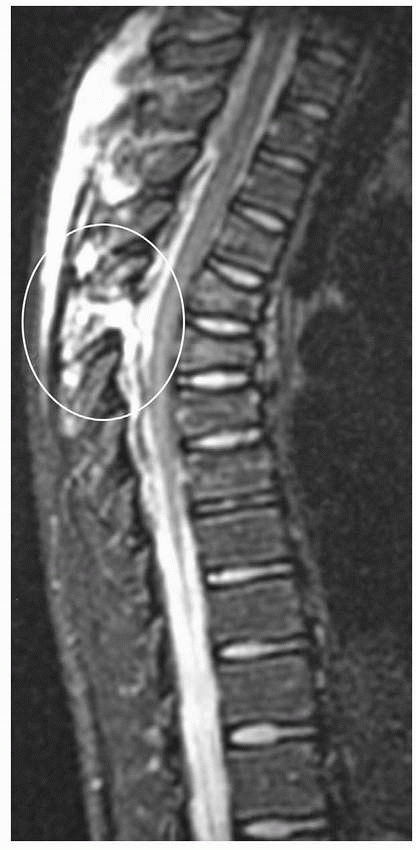
MRI is extremely sensitive and, given the brightness of edema fluid on
T2 images, may be overinterpreted. A study correlating MRI and
intraoperative surgical findings, however, demonstrated high levels of
both sensitivity and specificity in the MRI evaluation of posterior
soft-tissue injuries (Fig. 19-2).39
often requires surgical treatment in unstable fracture patterns. In
contrast, most stable injuries can be managed nonoperatively. There are
particular exceptions to these generalizations, of course. At times the
associated SCI or a substantial associated deformity may alter the
treatment approach to an otherwise mechanically stable injury. The
presence of a complete SCI in a child younger than 10 years is also a
determinant that may affect treatment strategies. The incidence of
paralytic spinal deformity (scoliosis) is nearly 100% in such cases,38,53
and a long instrumented fusion will likely be required at some point.
Depending on the fracture pattern and age of the patient, it may be
prudent to include much of the thoracic and lumbar spine in the initial
instrumented fusion.45
 |
|
FIGURE 19-2
This sagittal MRI demonstrates marked increased signal in the posterior ligamentous complex. Anteriorly a loss of height at the vertebra can be seen, suggesting a three-column spinal injury. |
each with purported advantages. Designed primarily with the adult spine
fracture patterns in mind, the Denis classification translates well for
the categorization of most pediatric thoracolumbar injuries.37
Based on theories of stability related to the three-column
biomechanical concept of the spine (anterior, middle, posterior
columns), the Denis classification in its simplest form includes
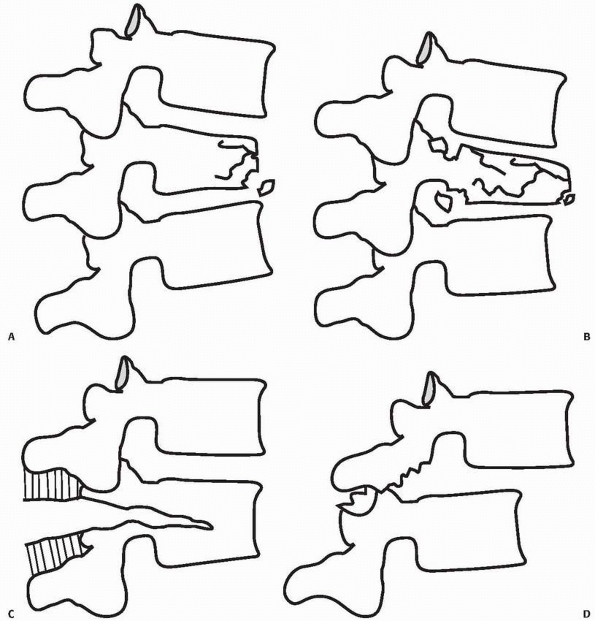
compression, burst, flexion-distraction, and fracture-dislocations (Fig. 19-3).
The vertebral body loses height anteriorly compared to the posterior
wall. Axial load with flexion is the common mechanism. Depending on the
degree and direction of flexion, the wedging may vary between the
coronal and sagittal planes (Fig 19-4). The
percentage of lost height defines the severity of compression
fractures, which rarely have an associated neurologic deficit. However,
the fractures are often associated with similar or occasionally more
severe fractures at adjacent or distant levels. Contiguous compression
fractures, each of a modest degree, together may result in a
substantial kyphotic deformity. Because the cause of these injuries,
such as a fall, are fairly common, it is at times necessary to
determine if a
wedged
vertebra seen radiographically represents an acute compression
fracture, sequelae of Scheuermann kyphosis, or a remote injury.
Clinical examination can localize pain to the site of the fracture in
acute injuries; however, MRI or bone scanning can confirm acute
fracture based on signal changes and increased isotope uptake.
 |
|
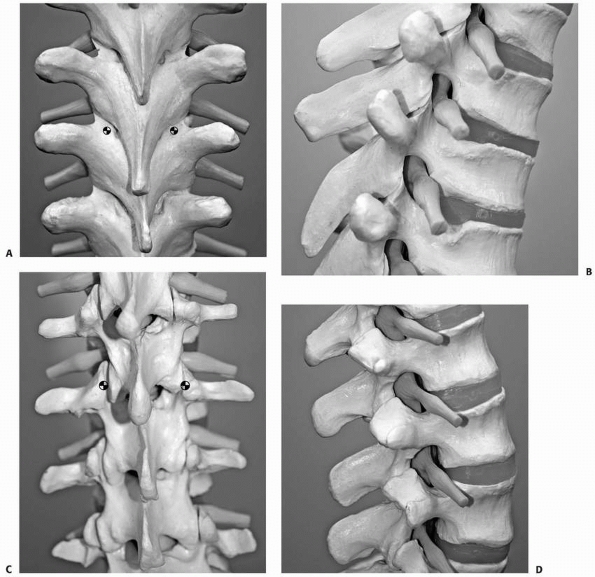
FIGURE 19-3 Denis classification of thoracolumbar fractures. A.
Compression fracture: This injury results in mild wedging of the vertebra primarily involving the anterior aspects of the vertebral body. The posterior vertebral height and posterior cortex remain intact. B. Burst fracture: A burst fracture involves both the anterior and middle columns with loss of height throughout the vertebral body. There may be substantial retropulsion of the posterior aspect of the vertebra into the spinal canal. In addition, posterior vertebral fractures and/or ligamentous injury may occur. C. Flexion distraction injuries: This fracture, which occurs commonly with a seatbelt injury mechanism, results in posterior distraction with disruption of the ligaments and bony elements of the posterior column, commonly extending into the anterior columns with or without compression of the most anterior aspects of the vertebra. D. Fracture dislocation: These complex injuries involve marked translation of one vertebra on another with frequently associated SCI as a result of translations through the spinal canal. |
compression fracture that extends posteriorly in the vertebral body to
include the posterior wall (middle column). Axial compression is the
primary mechanism, although posterior ligamentous injury and/or
posterior element fractures may also occur. Laminar fractures have been
known to entrap the dural contents. The fractures are most common in
the lower thoracic and upper lumbar levels. Associated neurologic
injury is related
to the severity of injury (greater injury index scores correlate with greater frequency of spinal cord injury42) and the degree of spinal canal encroachment by retropulsed bony fragments.30
SCI at the thoracolumbar junction may result in conus medullaris
syndrome or cauda equina syndrome. Careful examination of the perineal
area is required to identify these spinal lesions.
 |
|
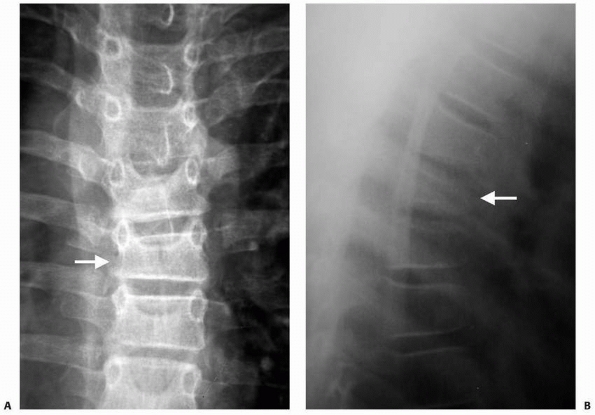
FIGURE 19-4 Compression fractures. A. This PA view demonstrates wedging in the coronal plane. B.
The more commonly recognized compression fractures involve wedging primarily in the sagittal plane with loss of anterior vertebral height. |
the pediatric population because this classic lap belt injury is more
frequent in back seat passengers, particularly when a shoulder strap is
lacking. Motor vehicle accidents are the primary cause of this injury.
The lap belt, which restrains the pelvis in adults, may ride up onto
the abdomen in children. Chance, and later Smith, described how with a
frontal impact, the weight of the torso is driven forward, flexing over
the restraining belt. With the axis of rotation in front of the spine,
distractive forces are placed on the posterior elements, with variable
degrees of anterior vertebral compression. This three-column injury is
generally unstable. The disruption of the posterior elements may occur
entirely through the bony (Chance) or ligamentous (Smith) elements,
although many times the fracture propagates through both soft and hard
tissues.
however, if no fracture exists, widening of the intraspinous distance
may be the only finding on an anteroposterior (AP) radiograph. Standard
transverse plain CT imaging may also miss this injury because the plane
of injury lies within the plane of imaging. One classic finding in
ligamentous flexion-distraction injuries is the “empty facet” sign.
When the inferior articular process of the superior vertebra is no
longer in contact with the superior articular process of the inferior
vertebra, the facet appears empty in the transverse CT image.23
Sagittal reconstructions are most revealing and MRI will provide
information about the integrity of the posterior ligamentous complex.
Identification of a purely intravertebral flexion-distraction fracture
is important, because this may alter the treatment in patients with
these injuries compared to those with severe ligamentous injury.
complex severe loading mechanisms. These are by definition unstable
injuries with a component of shearing and/or rotational displacement. A
special note in the pediatric population is the documentation of this
injury pattern in young patients exposed to nonaccidental trauma.15,35
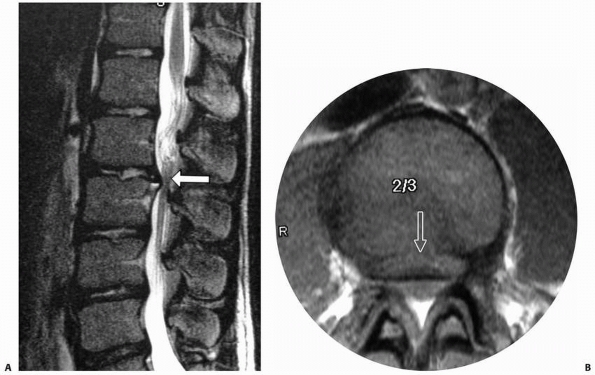
that do not fit the Denis classification include apophyseal avulsion
fractures and SCIWORA. Apophyseal injuries, typically of the lumbar
spine, occur in adolescents as a result of trauma. The mechanism is
thought to be related to flexion with a portion of the posterior corner
of the vertebral body (ring apophysis) fracturing and displacing
posteriorly into the spinal canal. Symptoms may mimic disc herniation,
although the offending structure is bone and cartilage rather than disc
material (Fig. 19-5).16,18
who described their experience at the University of Pittsburgh. They
noted a series of patients presenting with traumatic SCIs that were not
evident on plain radiographs or tomograms. Several mechanisms to
explain these findings have been proposed, including spinal cord
stretch and vascular disruption/infarction. MRI studies have confirmed
patterns of both cord edema and hemorrhage in such cases.25 Important additional facts about SCIWORA include the finding that some
patients had a delayed onset of their neurologic deficits. Transient
neurologic symptoms were persistent in many who later developed a
lasting deficit. Additionally, the younger patients (less than 8 years
old) had more severe neurologic involvement.5,50,51
 |
|
FIGURE 19-5 Ring apophyseal avulsion injuries. A.
This lateral MRI image demonstrates displacement of the ring apophysis, which functionally acts as a disc herniation. This, however, represents largely a bony and cartilaginous fragment, which results in neural element compression. B. Transverse image demonstrating canal stenosis associated with this injury. |
with a suspected spinal injury, plain radiographs are usually valuable.
An alert, cooperative patient without pain or tenderness in the back
can be cleared without radiographs. However, any patient with a
significant mechanism or associated injury (motor vehicle accident,
fall from greater than 10 feet, major long bone fracture, cervical or
head injury) requires thoracolumbar spine radiographs if they have
spinal tenderness, are obtunded, or have a distracting injury. Initial
films should include supine AP and lateral views of the thoracic and
lumbar spine. In addition, due to the strong association between
cervical spine fractures and thoracolumbar spine fractures after blunt
vehicular trauma, routine imaging of the complete spine when a cervical
fracture is identified is indicated.75
findings that should be sought in all cases. On AP radiographs, soft
tissue shadows may be widened by paravertebral hematoma. The bony
anatomy is viewed to evaluate for loss of height of the vertebral body
as compared to adjacent levels. Similar comparisons can be made with
regard to pedicle width and interspinous spacing. The lateral
radiographs give important information about the sagittal plane:
anterior vertebral wedging or collapse or posterior element distraction
or fracture. Careful scrutiny of the plain radiographs is always
prudent; however, the CT scan will nearly always be used to clarify any
suspected fractures. Antevil et al.1
reported the sensitivity of plain radiographs to be 70% (14 of 20
patients) for spine trauma, while the sensitivity was 100% for CT
scanning (34 of 34 patients).
trauma patients. Multidetector scanners allow rapid assessment with
axial, coronal, and sagittal images for patients with plain x-ray
abnormalities. The axial images are best for evaluating the integrity
of the spinal canal in cases of a burst fracture, while the sagittal
views will demonstrate vertebral body compression as well as posterior
element distraction or fracture. In addition, major dislocations easily
seen on plain radiographs will be better understood with regard to the
space left in the spinal canal for the neurologic elements. The amount
of spinal canal compromise has been correlated with the probability of
neurological deficit.48
Although more difficult to obtain in a multiply injured patient, this
study is mandatory in patients with a neurologic deficit in order to
assess the potential cause of cord dysfunction. The MRI is able to
distinguish areas of spinal cord hemorrhage and edema. Assessment of
the posterior ligamentous complex it critical in differentiating stable
and unstable burst fractures, as well as compression fractures and
flexion-distraction injuries. Although
subject
to overinterpretation, MRI has been shown to correlate very well with
intraoperative findings of the structural integrity of the posterior
soft tissues.39
extremities through the torso. The twelve thoracic and five lumbar
vertebrae are joined by intravertebral discs and strong ligaments, both
anteriorly and posteriorly. The bony architecture of the vertebrae
varies, with the smaller thoracic vertebrae having a more shingled
overlapping configuration compared to the lumbar segments. The thoracic
facets are oriented in the sagittal plane while those in the lumbar
spine lie nearly in the sagittal plane (Fig. 19-6).
 |
|
FIGURE 19-6 A,B.
Thoracic spine posterior and lateral views demonstrating the overlapping lamina and spinous processes present in this region. The circles mark the location of the thoracic pedicles, which may be important in surgical reconstruction. C,D. Lumbar spine posterior and lateral projections demonstrating the differences in lumbar spine anatomy. Again, the circles mark locations of the lumbar pedicles relative to the facets and transverse processes. |
adjacent and linked rib cage, as well as the smaller intervertebral
discs. The ribs make an important connection between the vertebra with
each rib head articulating across a given disc’s space. This is in
contrast to the relatively mobile lumbar segments, which have thick
intravertebral discs that permit substantial flexion-extension, lateral
bending, and axial rotation motion. The junction between the stiffer
thoracic spine and more flexible lumbar spine is a region of frequent
injury because of this transition between these two regions, which have
differing inherent regional stability.
posterior longitudinal ligaments, facet capsules, ligamentum flavum,
and interspinous and supraspinous ligaments. Together, these structures
limit the motion between vertebrae to protect the neurologic
elements.
The anterior longitudinal ligament is rarely disrupted in flexion
injuries but may be rendered incompetent by extension loading or a
severe fracture dislocation. On the contrary, flexion is the primary
mechanism of injury to the posterior ligaments—supraspinous and
interspinous, facet capsule, and ligamentum flavum. The healing
capacity of the completely torn posterior ligamentous complex is
limited, whereas bony fractures are more likely to heal with resultant
stability.
thoracolumbar spine as well. The space within the canal is largest in
the lumbar spine. The spinal cord traverses the entirety of the
thoracic spine and typically terminates as the conus medullaris at the
L-1 or L-2 level. The cauda equina occupies the dural tube below this
level, and injuries below L-1 are generally less likely to lead to
permanent neurologic deficit. This is not to say that compression at
this level cannot be serious, and careful examination of the perineum
for sensation as well as rectal tone is important in the evaluation of
potential conus medullaris and cauda equina syndromes.
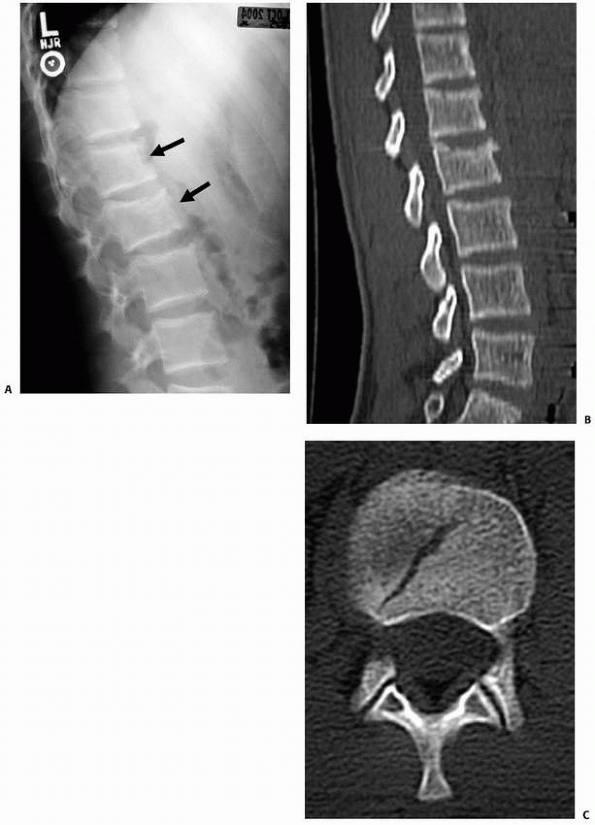
most likely fractures to occur in the thoracic spine secondary to axial
compression and flexion loading. The anterior aspect of the vertebral
body is involved, but the posterior wall of the vertebral body is by
definition intact. The degree of wedging is variable, as is the loss of
anterior height. These are nearly always stable injuries, although
examination of the posterior soft tissues is required to rule out any
more severe flexion-distraction injury, and a CT scan is required to
rule out a burst fracture (Fig. 19-7).
the most common thoracolumbar fracture pattern and can nearly always be
treated with immobilization with a brace that limits flexion, provides
pain relief, and reduces further loading of the fracture. Most
fractures heal in 4 to 6 weeks without significant additional collapse;
however, radiographs in the first several weeks should be obtained to
follow the sagittal alignment. Long-term studies have suggested modest
remodeling capacity of compression fractures occurring in childhood.43,54
Asymmetric growth at the endplates seems to allow some correction in
the wedged alignment over time in the skeletally immature patient.
Long-term results of compression fractures have been generally
favorable, although fractures of the endplates are associated with
later disc degeneration.34
more than 40 degrees or markedly alters the local sagittal alignment,
surgical treatment may be considered. This is most frequent in multiple
adjacent compression fractures that together create unacceptable
kyphosis. The preferred surgical treatment of such fractures is
generally a posterior compression instrumentation construct that spans
one or two levels above and below the affected vertebrae. Anterior
surgical treatment is rarely required. The intact posterior vertebral
wall provides a fulcrum to achieve kyphosis correction. The method of
posterior fixation may be either hooks or pedicle screws. A posterior
fusion over the instrumented segments ensures a lasting stable
correction. Cadaver studies and clinical studies on the use of balloon
vertebroplasty with calcium phosphate cement in adult patients are
encouraging, as this technique may be a potentially viable option to
treat compression fractures with significant angulation.36,69,70
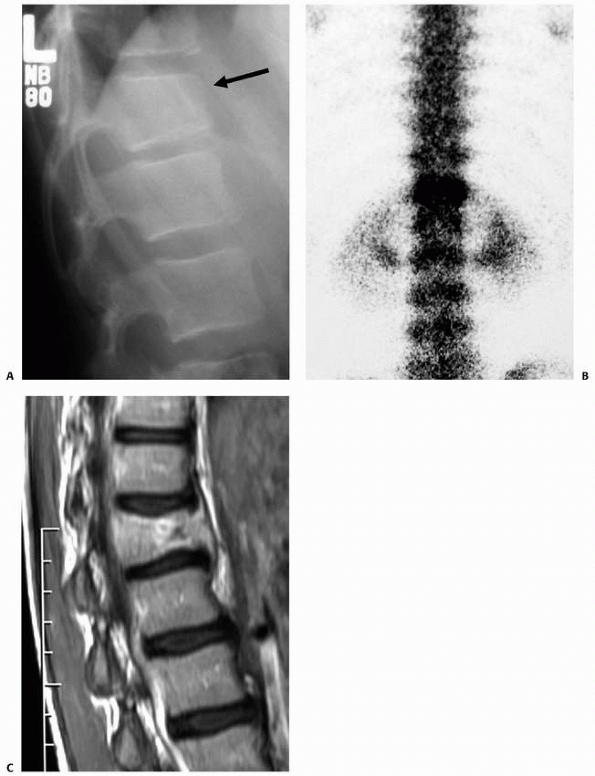
children and adolescents to a degree that predisposes them to
insufficiency fractures that are most often compression fractures (Fig. 19-8).
Multiple-level fractures are more frequent in this setting, and
problematic kyphosis may develop. Differentiating new from old
fractures can be difficult if serial radiographs are not available. A
thoracolumbosacral orthosis (TLSO) for a period of time longer than
typically used for simple compression fracture healing may be necessary
to prevent progressive kyphosis, though treating the primary cause of
the osteopenia is critical to maintaining normal alignment in such
cases. An endocrinologic evaluation and assessment of bone density by
dual energy x-ray absorptiometry are advised.
extend into the posterior wall of the vertebral body are labeled as
burst fractures. The treatment and classification of this fracture
pattern are controversial areas of spinal trauma management. There are
clearly some burst fractures that can be easily managed nonoperatively
in a brace and others that collapse further, resulting in increased
deformity unless surgically stabilized. Defining the characteristics of
stable and unstable burst fractures has been attempted by several
authors.14,24,46
An additional compounding variable in the treatment algorithm is SCI,
which is more frequent with burst fractures than with compression
fractures.
and unstable burst fractures has been attempted based on the degree of
comminution, loss of vertebral height, kyphotic wedging, and integrity
of the posterior ligamentous complex. A load-sharing classification
system assigns points based on comminution, fragment apposition, and
kyphosis.46 Although the Denis
classification suggests that all burst fractures are unstable because
of the involvement of at least two columns, it is clear that in many
cases the addition of a third-column injury (posterior ligamentous
complex) is required to result in a truly unstable condition. Some
advocate differentiating stable and unstable burst fractures solely on
the integrity of the posterior ligamentous complex.63,76
When a burst fracture is deemed stable, it must be done so on a
presumptive basis. Treatment is then based on an extension molded cast
or TLSO with the goal of allowing an upright position and ambulation.64
Frequent radiographic and neurologic follow-up is necessary to identify
early failures. Depending on the age of the patient and severity of the
fracture, immobilization is suggested for a duration of 2 to 4 months.
yet much of the adult literature provides valuable information about
the outcomes to expect following nonoperative treatment. Most of these
fractures in adults heal with little change in kyphosis and function
and minimal, if any, residual pain.73 It is reasonable to expect adolescent patients to heal at least as well and probably even faster. Wood et al.76
compared operative and nonoperative treatment in a prospective
randomized study of patients with burst fractures who were
neurologically intact with a normal posterior ligamentous complex. The
radiologic
and functional outcomes were not substantially different, and these
authors concluded that nonoperative treatment should be considered when
the posterior ligamentous complex and neurologic function are intact.76
Functional outcome does not appear to correlate with the degree of
spinal kyphosis, although long-term studies of scoliosis treatment do
suggest that an alteration of sagittal alignment may be detrimental
(flat back syndrome) in the long term.
 |
|
FIGURE 19-7 A.
This lateral radiograph demonstrates two upper lumbar vertebrae with slight loss of height suggestive of compression fractures. B,C. The CT images confirm an intact posterior vertebral body wall. This injury, therefore, represents a compression fracture rather than a burst fracture injury. |
however, these three-column injuries are often operatively stabilized.
When surgical treatment is selected, either an anterior or posterior
approach can be used, although this also remains controversial.
Anterior stabilization generally involves discectomy and strut grafting
that spans the fractured vertebra. Stabilization with a plate or
dual-rod system is appropriate. Posterior
options
include pedicle screw fixation one or two levels above and below the
fractured vertebra. Advances in the application of posterior
instrumentation for thoracolumbar fractures has demonstrated
encouraging, early outcomes with fracture stabilization without fusion
and in minimally invasive surgical techniques.72,74
 |
|
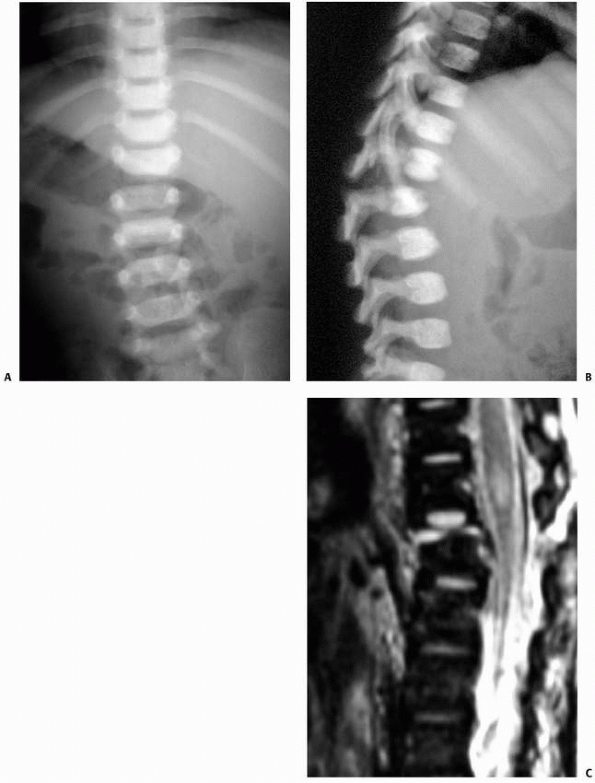
FIGURE 19-8 A.
Lateral radiograph demonstrating what appears to be a routine compression fracture. The patient did not have a significant history of trauma; however, pain was present and a bone scan was obtained to further evaluate this site. B. The bone scan demonstrated markedly increased uptake, confirming an acute process and prompting additional study. C. An MRI was obtained, which demonstrated loss of height and a lesion within the anterior aspect of the vertebral body, which was later confirmed to be an infectious process. |
the surgical treatment of a burst fracture is largely dictated by
surgeon preference and, to some degree, the features of the fracture.
Posterior approaches are familiar to all surgeons and can easily be
extended over many levels. Decompression of the spinal cord can be
achieved by indirect or direct methods. Restoration of the sagittal
alignment frequently leads to spontaneous repositioning of the
posteriorly displaced vertebral body fracture fragments. If additional
reduction of posterior wall fragments is required, direct fracture
reduction can be accomplished with a posterolateral or transpedicular
decompression.20 This also allows additional anterior column bone grafting that may add structural integrity and speed fracture healing.
through a corpectomy of the fractured vertebra. Structural strut
grafting restores the integrity of the anterior column. With this
graft, a load-sharing anterior plate or rod system completes the
reconstruction. This approach deals most directly with the pathology,
which in a burst fractures lies within the anterior and middle
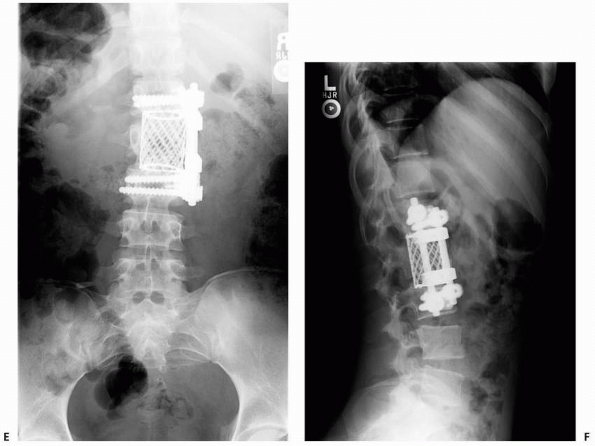
vertebral columns (Fig. 19-9).
Proponents of the anterior approach cite better biomechanical
stabilization of the unstable spine, better correction of segmental
kyphosis, and less loss of correction postoperatively.61,62,77
 |
|
FIGURE 19-9 Burst fracture. A.
This teenage patient presented with loss of vertebral body height associated with a motorcycle accident after jumping more than 20 feet. His neurologic examination was intact. B. CT scan confirmed a burst fracture component with very little retropulsion into the spinal canal. This appeared to be a stable injury and was initially managed with an orthosis. There was poor compliance with the orthosis and further collapse (C,D). (continues) |
dictated by the particular injury pattern and the associated abdominal
injuries. In general, these fractures are reduced by an extension
moment that can be maintained with either a cast or internal fixation.
A hyperextension cast is idea for younger patients (less than
approximately 10 years) with a primary bony injury pattern and no
significant intra-abdominal injuries. As described above, the posterior
disruption may pass through ligaments or joint
capsules
in a purely soft tissue plane of injury or traverse an entirely bony
path. The distinction is important, because bony fractures have the
potential for primary bony union, while the severe ligamentous injuries
are less likely to heal with lasting stability without surgical
intervention. As such, the greater the degree of ligamentous/facet
disruption, the more likely the need for stabilization with an
arthrodesis of the injured motion segment. Options for internal
fixation include posterior wiring in young children (supplemented with
a cast) and segmental fixation in a primarily compressive mode (Fig. 19-10).
 |
|
FIGURE 19-9 (Continued)
Given the lack of compliance and progressive kyphosis, the patient underwent anterior reconstruction with an iliac crest strut graft and plating (E,F). |
 |
|
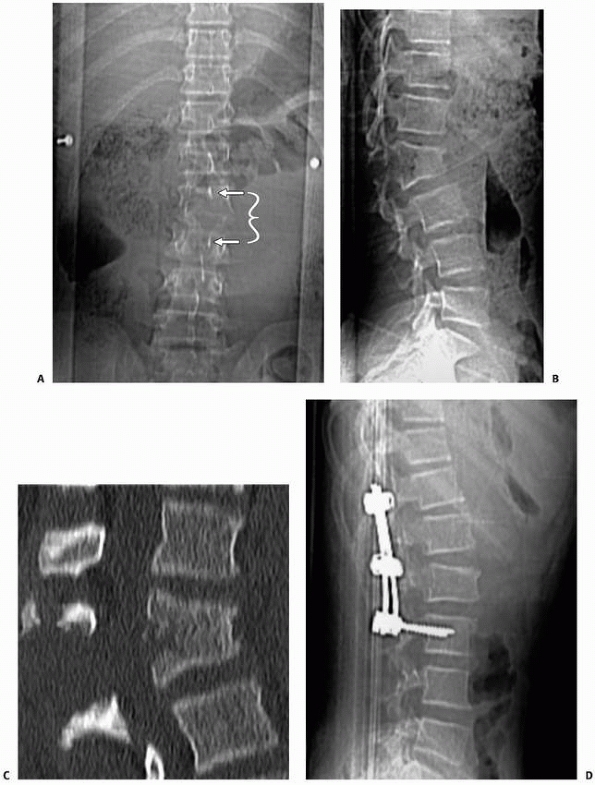
FIGURE 19-10 Flexion-distraction injury. A,B.
Plain radiographs of a restrained backseat passenger who was involved in a motor vehicle accident. The wedging of L2 with posterior distraction is visible on the lateral radiograph. The intraspinous widening is noted on the AP radiograph as well (arrows). C. Sagittal CT images confirm the injury pattern. D. Lateral radiographs following reconstruction with posterior spinal instrumentation. |
surgical stabilization. When the spinal cord function remains intact,
instrumented fusion gives the greatest chance for maintaining cord
function. On the other hand, if a complete SCI has occurred, internal
fixation will aid in the rehabilitation process, allowing early
transfers and upright sitting. At least two levels above and below the
level of injury should be instrumented to ensure restoration of
stability. In cases of SCI below the age of 10 years, a longer fusion
may be considered to reduce the incidence and severity of subsequent
paralytic scoliosis. Those injured after the adolescent growth spurt
are at low risk for late deformity if the fracture is well aligned at
the time of initial fixation (Fig. 19-11).
 |
|
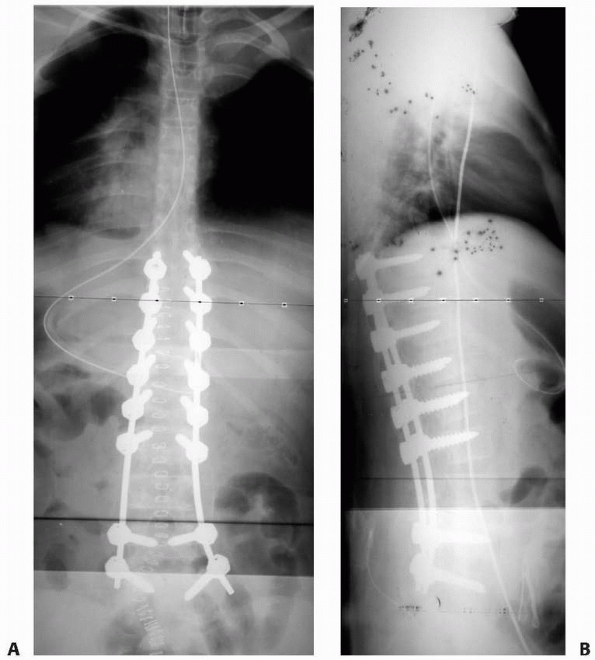
FIGURE 19-11 A,B.
AP and lateral radiographs demonstrating reconstruction after a lower thoracic level complete SCI associated with fracturedislocation in the lumbar spine combined with a burst fracture in the lower thoracic spine. Given the complete paraplegia present, a relatively long instrumentation construct was selected to provide a stable foundation in this skeletally immature patient. Four years postoperatively, the patient has no evidence of progressive spinal deformity; however, there is certainly some risk remaining of developing pelvic obliquity and upper thoracic deformity given the paraplegia. |
off-the-shelf Jewitt brace. Occasionally, a fracture is too proximal
for such an orthosis and an extension to the chin/occiput is required.
For fractures proximal to T6, a Minerva brace is used. These fractures
typically heal within 4 to 6 weeks, when the immobilization can be
discontinued. Activities should be limited for an additional 6 weeks.
Compression fractures with more than 50% loss of anterior vertebral
height are considered for either a closed reduction in an extension
molded body cast or surgical correction with posterior instrumentation.
The determination of which of these two approaches to choose is based
on associated injuries and a discussion with the family. Compression
fractures associated with neurological injury are managed surgically.
with burst fractures is nonoperative approach in light of recent
studies. If the neurologic status is normal and the posterior soft
tissues are intact, a TLSO or cast is used for 3 months. A cast is used
when local kyphosis is more than 20 degrees, and the cast is placed in
a hyperextension position in an
attempt
to restore sagittal alignment. If the posterior soft tissues are
disrupted (and the patient is neurologically intact), posterior
surgical stabilization is preferred. An anterior decompression is used
in patients with SCI if canal compromise is more than 50%.
findings: associated abdominal injuries and the presence of a
ligamentous component to the fracture. If either exists, surgical
treatment is the preferred approach. Casting in extension is
appropriate for fractures that transverse an entirely bony plane
without intra-abdominal pathology. A thigh is incorporated into the
cast for greater control of lumbar lordosis. Surgical treatment is by a
posterior approach and includes only the involved vertebrae.
Monosegmental pedicle screw fixation is generally preferred.
The timing of such intervention depends on the associated injuries and
the ability of the patient to tolerate surgical intervention; however,
stabilization as early as possible is preferred. SCI nearly always
complicates the management of these injuries, and a deteriorating
neurologic examination makes surgical treatment of the spine an
emergency that should be treated as quickly as possible.
recommendations of the Third National Acute Spinal Cord Injury Study
and prescribe methylprednisolone if it can be given within eight hours
of the time of injury. We are skeptical that this provides significant
benefit, but we believe this remains the current medical and legal
standard.
-
Do not hesitate to get advanced imaging, especially CT scanning.
-
Understand the mechanics of the injury to develop a rational treatment plan.
-
Always seek to identify additional levels of spinal injury when one is discovered.
-
Document the neurologic examination precisely and repeat it often.
-
Watch for associated injuries, both musculoskeletal and others.
-
Do not let MRI/CT findings replace a careful examination of the back.
-
Monitor neurologic status carefully
because an unrecognized change may limit the ability to intervene early
and prevent permanent sequelae.
management of acute SCI associated with thoracolumbar fractures. These
include both nonoperative and operative methods of treatment.
Investigations into the benefits of steroids in mitigating the effects
of the secondary phase of SCI that follows the acute trauma have been
mixed, although clinical trials have suggested benefit in specific
instances.
the neural tissue, possibly with compression remaining from fracture
fragments or displacement. Once the initial injury occurs, biochemical
cascades are set into motion, resulting in further injury of spinal
cord tissue. Experimental studies have suggested that steroids
administered early in the postinjury period could limit of these
detrimental secondary effects. Based on randomized clinical trails of
methylprednisolone administration after acute spinal cord injury,6,7
current recommendations for steroid use are dependent on the timing of
administration relative to the occurrence of the injury. If the time
lapse is less than 3 hours, a bolus of 30 mg/kg of methylprednisolone
is followed by an hourly infusion of 5.4 mg/kg for 24 hours duration.
If the lapse between injury and treatment is 3 to 8 hours, an infusion
of the same dose is continued for 48 hours. More importantly, if more
than 8 hours have passed following the SCI, no steroids are recommended.7
steroid use, there has been an increased complication rate. Infection
is the most common with both pneumonia and sepsis occurring. Steroids
are known to depress the immune response.19 These issues have resulted in an inconsistent adoption of the National Acute Spinal Cord Injury Study recommendations.
 |
|
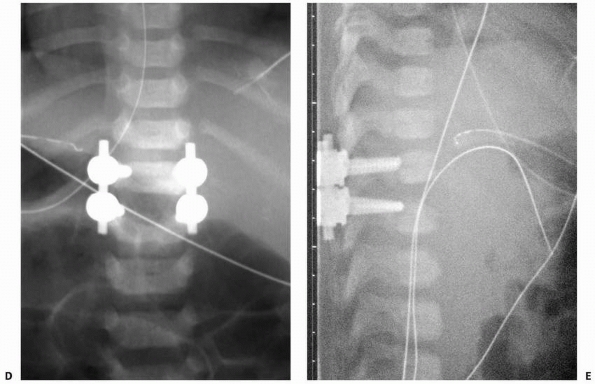
FIGURE 19-12 A,B.
This 8-month-old child presented with an incomplete SCI and a thoracolumbar fracture dislocation due to nonaccidental trauma. The malalignment of the vertebral segments is noted on both the AP and lateral projections. C. The MRI demonstrated a three-column injury with a fracture through the vertebral endplate. (continues) |
SCI also remains debated. Traditional teaching suggests no benefit to
decompression when a complete SCI exists. This may be true, but if
early decompression of an incomplete SCI is beneficial, and there are
experimental data to suggest it is, then it may be impossible to
determine early on if the patient has an incomplete injury but remains
in spinal shock. Spinal shock may last for 24 hours, leaving an
incomplete SCI patient completely unresponsive with regard to spinal
cord function. The data to suggest a benefit to early decompression are
largely experimental; however, a clinical study also reported a
benefit. In a series of 91 pediatric patients, 66 with immediate
decompression were compared to 25 with whom decompression was delayed.
Improvement of at least one Frankel grade occurred in one half of the
early decompression patients compared to
one quarter of those that who had delayed decompression.52
Early surgery has been documented to shorten the intensive care unit
stays and length of hospitalizations, shorten time on mechanical
ventilation support, and lower overall complication rates in patients
with thoracolumbar spine injuries.11
 |
|
FIGURE 19-12 (Continued) D,E. The patient had an open reduction and instrumentation with pedicle screw fixation using a 3.5-mm cervical system.
|
against spinal cord decompression if the MRI documents persistent
compression in the setting of an SCI. Pediatric patients have a
substantial potential for recovery, and reducing pressure on the neural
elements may be important in maximizing functional recovery. There is
little controversy if spinal cord function is deteriorating in a
patient with a known compressive lesion. This is an emergency that
warrants decompression by either an anterior or posterior approach.
Realignment of the spinal column and removal of fragments from the
canal are required. The exact surgical approach depends on the location
of offending structures and the nature of the instability.
JL, Sise MJ, Sack DI, et al. Spiral computed tomography for the initial
evaluation of spine trauma: a new standard of care? J Trauma
2006:61:382-387.
M, St-Vil D, Lallier M, et al. Abdominal injuries associated with
thoracolumbar fractures after motor vehicle collision. Pediatr Surg
2001;36:760-762.
PP, Vogt MT, Ward WT. Pediatric spinal cord injury without radiographic
abnormality (SCIWORA): the absence of occult instability and lack of
indication for bracing. Spine 2002;27:2788-2800.
MB, Shepard MJ, Holford TR, et al. Administration of methylprednisolone
for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment
of acute spinal cord injury. Results of the Third National Acute Spinal
Cord Injury Randomized Controlled Trial. National Acute Spinal Cord
Injury Study. JAMA 1997;277:1597-1604.
LY, Glassman SD, Campbell MJ. Pediatric Spine fractures: a review of
137 hospital admissions. J Spinal Disord 2004;17:477-482.
WV, Dormans JP, Drummond DS, et al. Circumferential growth plate
fracture of the thoracolumbar spine from child abuse. J Pediatr Orthop
1996;16:210-214.
A, Thaleisnik M, Fishel B, et al. Recovery of neurologic function after
spinal cord injury in Israel. Spine 2002;27:1733-1735.
JG, Deuser WE, Beilman GJ. Early surgery for thoracolumbar spine
injuries decreases complications. J Trauma 2004;56:52-57.
GH, Nelson BJ, Beghard JS, et al. Functional outcome of thoracolumbar
burst fractures managed with hyperextension casting or bracing and
early mobilization. Spine 1996;21:2170-2175.
F. The three-column spine and its significance in the classification of
acute thoracolumbar spinal injuries. Spine 1983;8:817-831.
P, Hansen CM, Christofersen MR. Child abuse presenting as a
thoracolumbar spinal fracture dislocation: a case report. Pediatr Emerg
Care 1994;10:83-86.
JL, Runge M, Badoz A, et al. Radiology of posterior lumbar apophyseal
ring fractures: report of 13 cases. Neuroradiology 1988;30:337-344.
S, Safavi-Abbasi S, Theodore N, et al. Thoracolumbar and sacral spinal
injuries in children and adolescents: a review of 89 cases. J Neurosurg
2007;106:426-433.
S, Raque G, Appel S, et al. The two-edged sword of large-dose steroids
for spinal cord trauma. Ann Surg 1993;218:419-425.
G, Coman TC, Zaccone C, et al. Posterolateral approach in the treatment
of unstable vertebral body fractures of the thoracic-lumbar junction
with incomplete spinal cord injury in the paediatric age group. Childs
Nerv Syst 2003;19:35-41.
RA, Gaebler-Spira D, Sisung C, et al. Functional improvement after
pediatric spinal cord injury. Am J Phys Med Rehabil 2002;81:458-463.
S, Mehta S, Dormans JP. Langerhans cell histiocytosis of the spine in
children. Long-term follow-up. J Bone Joint Surg Am 2004;86-A:1740-1750.
FE, Levine AM, Joslyn JN, et al. Pure thoracolumbar facet dislocation:
clinical features and CT appearance. Radiology 1986;161:505-508.
SD, Court-Brown CM. Rationale for the management of flexion-distraction
injuries of the thoracolumbar spine based on a new classification. J
Spinal Disord 1989; 2:176-183.
PA, Pang D. Magnetic resonance imaging in the evaluation of spinal cord
injury without radiographic abnormality in children. Neurosurgery
1994;35:406-414.
J, Bastiani-Griffet F, El-Hayek T, et al. Management of seat-belt
syndrome in children. Gravity of 2-point seat-belt. Eur J Pediatr Surg
2002;12:63-66.
MN, Zabramski JM, Browner CM, et al. Pediatric spinal trauma. Review of
122 cases of spinal cord and vertebral column injuries. Neurosurg Clin
N Am 1988;68: 18-24.
T, Kanada K, Abumi K. Relationship between traumatic spinal canal
stenosis and neurologic deficits in thoracolumbar burst fractures.
Spine 1988;13:1268-1272.
JF, Miller PQ, Panacek EA, et al. Epidemiology of thoracolumbar spine
injury in blunt trauma. Acad Emerg Med 2001;8:866-872.
K, Kirkpatrick AW, Finkelstein J, et al. Blunt abdominal aortic trauma
in association with thoracolumbar spine fractures. Injury
2001;32:201-207.
LI, Serlo WS, Tervonen OA, et al. Posttraumatic findings of the spine
after earlier vertebral fracture in young patients: clinical and MRI
study. Spine 2000;25: 1104-1108.
PK, Marks SC. Vertebral body fractures in child abuse.
Radiologic-histopathologic correlates. Invest Radiol 1992;27:715-722.
P, Repantis T, Petsinis G, et al. Direct reduction of thoracolumbar
burst fractures by means of balloon kyphoplasty with calcium phosphate
and stabilization with pedicle-screw instrumentation and fusion. Spine
2008;33:E100-E108.
JE, Dickson JH, Carter RE. Paralytic spinal deformity following
traumatic spinal-cord injury in children and adolescents. J Bone Joint
Surg Am 1981;63:47-53.
HM, Kim HS, Kim DJ, et al. Reliability of magnetic resonance imaging in
detecting posterior ligament complex injury in thoracolumbar spinal
fractures. Spine 2000;25: 2079-2084.
M, Davidson D, Fleuriau-Chateau P, et al. Seat belt fracture with late
development of an enterocolic fistula in a child. A case report. Spine
1999;24:1151-1155.
TL, Berdon WE, Cassell I, et al. Thoracolumbar fracture with
listhesis—an uncommon manifestation of child abuse. Pediatric Radiology
2003;33:305-310.
KK, Anders M, Ralph H, et al. A modeling capacity of vertebral
fractures exists during growth—an up to 47-year follow-up. Spine
2003;28:2087-2092.
JK, Erkkila JC, Winter RB. Spine deformity subsequent to acquired
childhood spinal cord injury. J Bone Joint Surg Am 1981;63:1401-411.
R, Avanzi O. Correlation between neurologic deficit and spinal canal
compromise in 198 patients with thoracolumbar and lumbar fractures.
Spine 2005;30:787-791.
K, Reilly CW, Perdios A, et al. The spectrum of adominal injuries
associated with chance fractures in pediatric patients. Eur J Pediatr
Surg 2007;17:322-327.
SM, Selden NR, Quint DJ, et al. Immediate spinal cord decompression for
cervical spinal cord injury: feasibility and outcome. Trauma
2002;52:323-332.
P, DiSilvestre M, Greggi T. Treatment of spinal fractures in children
and adolescents: long-term results in 44 patients. Spine
2002;27:1989-1994.
JC, Kassis B, Glorion C, et al. Vertebral growth after thoracic or
lumbar fracture of the spine in children. J Pediatr Orthop
1997;17:115-120.
AB, Letts RM, Black GB. Pediatric Chance fractures: association with
intra-abdominal injuries and seatbelt use. Trauma 1990;30:384-391.
RC, Pui CH, Schell MJ. Vertebral compression fracture as a presenting
feature of acute lymphoblastic leukemia in children. Cancer
1988;61:589-592.
R, Guenther E, Carroll K, et al. The clinical presentation of pediatric
thoracolumbar fractures. J Trauma 2006;60:187-192.
RC, Best NM, Reilly TM, et al. Anterior-only stabilization of
three-column thoracolumbar injuries. J Spinal Disord Tech
2005;18:S7-S14.
RC, Renkens K, Hanson D, et al. Unstable thoracolumbar burst fractures
: anterior-only versus short-segment posterior fixation. J Spinal
Disord Tech 2006;19:242-248.
WJ, Liu TJ, Shen YS. Nonoperative treatment versus posterior fixation
for thoracolumbar junction burst fractures without neurologic deficit.
Spine 2001;26:1038-1045.
WJ, Shen YS. Nonsurgical treatment of three-column thoracolumbar
junction burst fractures without neurologic deficit. Spine
1999;24:412-415.
CJ, Taylor GA, Newman KD, et al. Safety-belt injuries in children with
lap-belt ecchymosis: CT findings in 61 patients. AJR Am J Roentgenol
1991;157:111-114.
JB, Allred D, Hyman J. Use of magnetic resonance imaging in evaluating
injuries to the pediatric thoracolumbar spine. J Pediatr Orthop
2001;21:288-293.
AD, Koreska J, Moseley CF. Progression of scoliosis in Duchenne
muscular dystrophy. J Bone Joint Surg Am 1989;71:1066-1074.
S, Ansell BM, Reeve J. Vertebral collapse in juvenile chronic
arthritis: its relationship with glucocorticoid therapy. Calcif Tissue
Int 1987;41:75-78.
JJ, van de Kraats EB, Oner FC, et al. Bone displacement and the role of
longtudinal ligaments during balloon vertebroplasty in traumatic
thoracolumbar fractures. Spine 2005;30:1832-1839.
JJ, van de Kraats EB, Oner Fc, et al. The reduction of endplate
fractures during balloon vertebroplasty: a detailed radiological
analysis of the treatment of burst fractures using pedicle screws,
balloon vertebroplasty, and calcium phosphate cement. Spine
2005;30:1840-1845.
MY, Hoh DJ, Leary SP, et al. High rates of neurological improvement
following severe traumatic pediatric spinal cord injury. Spine
2004;29:1493-1497.
ST, Ma HL, Liu CL, et al. Is fusion necessary for surgically treated
burst fractures of the thoracolumbar and lumbar spine? A prospective,
randomized study. Spine 2006; 31:2646-2652.
JN, Collalto P, Lehmann TR. Thoracolumbar “burst” fractures treated
conservatively: a long-term follow-up. Spine 1988;13:33-38.
MH, Glees M, Plieschnegger C, et al. Five-year follow-up examination
after purely minimally invasive posterior stabilization of
thoracolumbar fractures: a comparison of minimally invasive
percutaneously and conventionally open treated patients. Arch Orthop
Trauma Surg 2007;127:335-343.
JE, Hensberry R, Bozeman WP, et al. Risk of thoracolumbar fractures
doubled in victims of motor vehicle collisions with cervical spine
fractures. J Trauma 2006;61: 686-687.
K, Butterman G, Mehbod A, et al. Operative compared with nonoperative
treatment of a thoracolumbar burst fracture without neurological
deficit. J Bone Joint Surg 2003;85:773-781.
KB, Bohn D, Mehbod A. Anterior versus posterior treatment of stable
thoracolumbar burst fractures without neurologic deficit: a
prospective, randomized study. J Spinal Disord Tech 2005;18:S15-823.