
Editors: Tornetta, Paul; Einhorn, Thomas A.; Damron, Timothy A.
Title: Oncology and Basic Science, 7th Edition
Copyright ©2008 Lippincott Williams & Wilkins
> Table of Contents > Section I
– Evaluation and Management of Musculoskeletal Oncology Problems > 4
– Treatment Principles > 4.1 – Surgical Margins
– Evaluation and Management of Musculoskeletal Oncology Problems > 4
– Treatment Principles > 4.1 – Surgical Margins
4.1
Surgical Margins
Robert Quinn
Appropriate surgical planning for the treatment of
musculoskeletal tumors requires proper histologic diagnosis and
staging. The type of surgical margin most appropriate for a given tumor
is, to a large extent, dictated by the appropriate stage.
musculoskeletal tumors requires proper histologic diagnosis and
staging. The type of surgical margin most appropriate for a given tumor
is, to a large extent, dictated by the appropriate stage.
Terminology
-
The pathologic definitions in Table 4.1-1 are essential to the understanding of surgical margins.
Surgical Margins
-
The surgical procedures and margins are defined in Table 4.1-2.
Surgical Procedures
Principles of Selecting the Appropriate Surgical Procedure
-
Selection of the most appropriate surgical margin is dependent upon the overall treatment goals of the patient.
-
Table 4.1-3 shows some example tumor types according to surgical stage for each type of surgical procedure.
-
If the goal of treatment is to establish
the best chance of cure, then the most appropriate margin is that which
will provide the lowest risk of local recurrence.-
Most aggressive benign tumors: rarely
life- or limb-threatening, and these are often best treated with a less
aggressive procedure, accepting a low rate of local recurrence in
exchange for improved functional outcome
|
Table 4.1-1 Terms Pertaining to Surgical Margins
|
||||||||
|---|---|---|---|---|---|---|---|---|
|
|
Table 4.1-2 Definitions of Surgical Procedures Related to Margins
|
||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Types of Surgical Procedures
-
Figures 4.1-1 and 4.1-2 illustrate the respective planes of dissection that would be performed with these types of resections and amputations.
Intralesional Procedure
-
Debulking or curettage of a tumor from within the tumor itself
Indications
-
This type of procedure may be performed for diagnosis (i.e., with an open biopsy), for cure, or for palliation.
-
Biopsy
-
When surgery is to be performed for
sarcomas with curative intent, the carefully planned biopsy is an
acceptable initial intralesional procedure. -
An intralesional margin obtained following resection is generally unplanned and unlikely to be curative.
-
-
Palliation
-
An intralesional procedure might be
performed in the presence of metastatic disease where the primary goal
of surgery is palliation and the secondary goal is tumor removal. -
Example: Impending pathologic fracture of the femur
-
Primary goal of the procedure is stabilization
P.52
with an intramedullary rod, but intralesional curettage of the tumor is performed for two reasons:-
To allow further strengthening of the construct by replacing tumor with polymethylmethacrylate
-
To afford potentially greater efficacy of adjuvant radiation or chemotherapy
-
-
-
 |
|
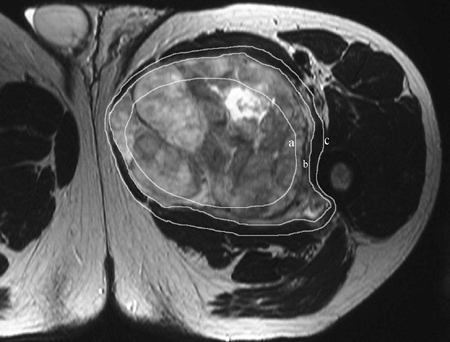
Figure 4.1-1
Magnetic resonance imaging of a soft tissue sarcoma in the adductor compartment of the thigh demonstrating potential surgical margins. Dissection along line a would constitute an intralesional margin, along line b would be a marginal resection, and along line c would be a wide margin. A radical margin would entail removal of the entire adductor compartment. |
Residual Disease and Risk of Recurrence
-
By definition this type of procedure
leaves behind macroscopic, or at least microscopic, disease. This is
acceptable for benign nonaggressive lesions (stage 1 or 2), but it is
not desirable for aggressive benign or malignant lesions except when
palliation is the goal. -
For many benign bone and soft tissue
tumors (enchondroma, nonossifying fibroma, eosinophilic granuloma),
this procedure will result in a very small risk of local recurrence. -
For most malignancies, this procedure will result in a high rate of local recurrence.
Marginal Procedure
-
A more aggressive excision performed
through the reactive zone to minimize the amount of residual
microscopic tumor, but leaving the potential for both satellite and
skip lesions -
For soft tissue tumors an en bloc excision (“shell-out” procedure) is performed.
-
For more aggressive benign tumors of bone
(aneurysmal bone cyst, chondroblastoma, osteoblastoma) and even some
low-grade chondrosarcomas, acceptance of a marginal margin by way of an
extended intralesional curettage will result in a measurable risk of
local recurrence but not high enough to warrant the additional
morbidity of obtaining a wide margin except occasionally in expendable
bones such as the fibula, rib, or ilium.-
Extended intralesional curettage
procedure: A marginal curettage is performed, and the margin is then
extended into the reactive zone or even into normal tissue mechanically
with a bur and~hor using cytostatic or cytocidal agents such as liquid
nitrogen, phenol, laser, or alcohol.
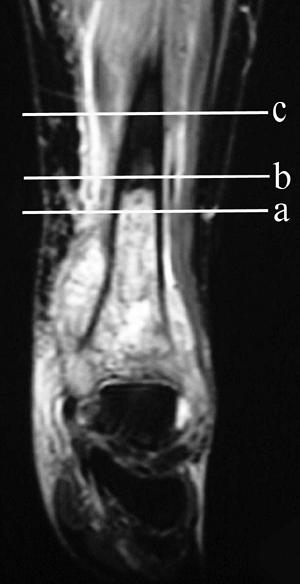
![]() Figure 4.1-2
Figure 4.1-2
Magnetic resonance imaging of a high-grade osteosarcoma of the distal
tibia illustrating margins possible obtained at different levels of
amputation: intralesional (a), marginal (b), and wide (c). A radical margin would be obtained with a knee disarticulation. -
-
Amputations that achieve marginal margins
-
May be performed as a palliative procedure
-
May result from unsuccessful attempt at a wide margin amputation
-
May be performed with plans to use adjunctive treatment to minimize recurrence
-
P.53
Wide Margins
-
When the plane of dissection passes
through normal tissue some distance beyond the reactive zone,
theoretically eliminating satellite lesions but potentially leaving
skip lesions behind
Indications
-
Cure: Appropriate margin to achieve cure
for majority of bone and soft tissue sarcomas, for occasional isolated
bone metastases (such as renal carcinoma), and for some particularly
aggressive benign tumors such as desmoid-type fibromatosis -
Palliation: Occasionally wide resection
will also be performed for the treatment of metastatic disease when the
tumor is felt to be poorly responsive to other adjuvant measures.
Amputation With Wide Margins
-
Performed with curative intent when limb salvage is not indicated
-
When limb-sparing surgery would leave an
extremity with compromised vascularity or limited function inferior to
that which would be obtained with a prosthesis -
If a patient would prefer amputation in
deference to the more complex nature of a reconstructive procedure and
the potential associated complications
Radical Resection
-
Removal of the entire compartment(s)
involved by the tumor, including the entire bone for bone tumors and
the entire muscle compartment from origin to insertion for soft tissue
tumors or soft tissue extension from bone tumors -
Radical resections are largely of
historical importance but were thought to be necessary in some cases to
eliminate both satellite and skip lesions. In practice, skip lesions
are rare, probably represent metastatic disease, and can generally be
recognized on imaging studies provided the entire compartment is
visualized. Hence, prophylactic removal of the entire compartment
without evidence of skip lesions is rarely indicated.-
If the skip lesion is in close proximity to the primary, both will generally be resected with a single wide margin.
-
If the skip lesion is more remote from
the primary, two separate wide resections will generally suffice and
often allow better functional outcome than a radical resection.
-
Suggested Reading
Enneking
WF, Maale GE. The effect of inadvertent tumor contamination of wounds
during the surgical resection of musculoskeletal neoplasms. Cancer 1988;62(7):1251–1256.
WF, Maale GE. The effect of inadvertent tumor contamination of wounds
during the surgical resection of musculoskeletal neoplasms. Cancer 1988;62(7):1251–1256.
Enneking WF, Spanier SS, Goodman MA. A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop Relat Res 1980;(153):106–120.
Enneking
WF, Spanier SS, Malawer MM. The effect of the anatomic setting on the
results of surgical procedures for soft parts sarcoma of the thigh. Cancer 1981;47(5):1005–1022.
WF, Spanier SS, Malawer MM. The effect of the anatomic setting on the
results of surgical procedures for soft parts sarcoma of the thigh. Cancer 1981;47(5):1005–1022.
Rydholm A. Surgical margins for soft tissue sarcoma. Acta Orthop Scand Suppl 1997;273:81–85.
Rydholm A, Rooser B. Surgical margins for soft-tissue sarcoma. J Bone Joint Surg [Am] 1987;69(7):1074–1078.
Virkus WW, Marshall D, Enneking WF, et al. The effect of contaminated surgical margins revisited. Clin Orthop Relat Res 2002;(397):89–94.
Wolf RE, Enneking WF. The staging and surgery of musculoskeletal neoplasms. Orthop Clin North Am 1996;27(3):473–481.