
Editors: Chapman, Michael W.
Title: Chapman’s Orthopaedic Surgery, 3rd Edition
Copyright ©2001 Lippincott Williams & Wilkins
> Table of Contents > SECTION IX – PEDIATRIC DISORDERS > CHAPTER 173 – LEGG-CALVÉ-PERTHES DISEASE
CHAPTER 173
LEGG-CALVÉ-PERTHES DISEASE
John A. Herring
J. A. Herring: Chief of Staff, Department of Orthopaedics, Texas Scottish Rite Hospital for Children, Dallas, Texas, 75219.
INTRODUCTION
Legg-Calvé-Perthes disease is a form of idiopathic
avascular necrosis of the femoral head. Although the exact etiology of
the disorder is not known, the association of Legg-Calvé-Perthes
disease with delayed skeletal maturation suggests a systemic
susceptibility to the problem. Some children have abnormalities of
coagulation with decreases in the factors involved in thrombolysis,
which may predispose them to avascular necrosis.
avascular necrosis of the femoral head. Although the exact etiology of
the disorder is not known, the association of Legg-Calvé-Perthes
disease with delayed skeletal maturation suggests a systemic
susceptibility to the problem. Some children have abnormalities of
coagulation with decreases in the factors involved in thrombolysis,
which may predispose them to avascular necrosis.
The clinical course is quite variable, making it
difficult for the clinician to know for certain which patients need and
will benefit from treatment. Current use of the lateral pillar
radiographic classification has improved our ability to assess severity
and prognosis in an individual case. Children younger than 6 years of
age at onset usually have a benign course, and major treatment is not
often necessary because they have a longer growing time to remodel
abnormalities. Children between 6 and 9 years of age at onset have more
symptoms and often benefit from surgical treatment. Children older than
9 years of age have a more severe course, and their response to
treatment is less predictable. In the long run, 50% of patients have no
disability as adults and the other half develop degenerative hip
disease by the fifth or sixth decade of life.
difficult for the clinician to know for certain which patients need and
will benefit from treatment. Current use of the lateral pillar
radiographic classification has improved our ability to assess severity
and prognosis in an individual case. Children younger than 6 years of
age at onset usually have a benign course, and major treatment is not
often necessary because they have a longer growing time to remodel
abnormalities. Children between 6 and 9 years of age at onset have more
symptoms and often benefit from surgical treatment. Children older than
9 years of age have a more severe course, and their response to
treatment is less predictable. In the long run, 50% of patients have no
disability as adults and the other half develop degenerative hip
disease by the fifth or sixth decade of life.
Treatment has been based on the containment principle,
which means positioning the femoral head within the acetabulum in such
a way as to reduce lateralization and collapse of the softened head. In
the past, this was done with braces, but at present, femoral or pelvic
osteotomies are preferred.
which means positioning the femoral head within the acetabulum in such
a way as to reduce lateralization and collapse of the softened head. In
the past, this was done with braces, but at present, femoral or pelvic
osteotomies are preferred.
COURSE OF DISEASE AND NATURAL HISTORY
The initial events in the course of Legg-Calvé-Perthes
disease are well established. The femoral head becomes ischemic for
reasons unknown and for an unknown period of time. Several studies
suggest that at least two episodes of ischemia are necessary to produce
the typical changes of Legg-Calvé-Perthes disease (7,27). More recent studies have shown that a number of children have deficiencies of proteins S and C and hypofibrinolysis (8,9).
The original studies suggested that the majority of children were
deficient in these factors, but subsequent reports have found only a
small proportion patients with Legg-Calvé with these coagulopathies (14).
disease are well established. The femoral head becomes ischemic for
reasons unknown and for an unknown period of time. Several studies
suggest that at least two episodes of ischemia are necessary to produce
the typical changes of Legg-Calvé-Perthes disease (7,27). More recent studies have shown that a number of children have deficiencies of proteins S and C and hypofibrinolysis (8,9).
The original studies suggested that the majority of children were
deficient in these factors, but subsequent reports have found only a
small proportion patients with Legg-Calvé with these coagulopathies (14).
P.4424
Following the ischemic episode, the femoral head becomes
radiodense, then appears fragmented radiographically as dead bone is
resorbed, and finally reossifies with new bone formation. These
sequential phases have been classified by Waldenström (30)
as increased density, fragmentation, reossification, and residual
stages. No treatment to date has been shown to either accelerate or
delay the healing process, although it was initially thought that
femoral osteotomy resulted in more rapid healing. This was disproved in
studies by Clancy and Steel (4) and Kendig and Evans (15).
During the fragmentation phase in more severe disease, the head loses
height, enlarges, and may flatten. As the head enlarges, the anterior
and lateral portions of the head extrude from the acetabulum. Over
several years, the femoral head completely reossifies and may remain
round in mild cases, become ovoid in moderate cases, and become
flattened in severe cases. Stulberg and colleagues (29) classified these groups according to femoral head status as:
radiodense, then appears fragmented radiographically as dead bone is
resorbed, and finally reossifies with new bone formation. These
sequential phases have been classified by Waldenström (30)
as increased density, fragmentation, reossification, and residual
stages. No treatment to date has been shown to either accelerate or
delay the healing process, although it was initially thought that
femoral osteotomy resulted in more rapid healing. This was disproved in
studies by Clancy and Steel (4) and Kendig and Evans (15).
During the fragmentation phase in more severe disease, the head loses
height, enlarges, and may flatten. As the head enlarges, the anterior
and lateral portions of the head extrude from the acetabulum. Over
several years, the femoral head completely reossifies and may remain
round in mild cases, become ovoid in moderate cases, and become
flattened in severe cases. Stulberg and colleagues (29) classified these groups according to femoral head status as:
|
The prognosis for a child with Legg-Calvé-Perthes
disease can be estimated to some degree. The most frequently reported
prognostic factor is the age of the child at the onset of the disease.
Most, but not all, children presenting at younger than 6 years of age
have a good prognosis, whereas those between 6 and 9 years of age have
a variable course. Children older than 9 years of age presenting with
Legg-Calvé-Perthes disease have a worse prognosis than those with an
earlier onset. Within these general guidelines, the disease is quite
variable, and individual prognostication is difficult.
disease can be estimated to some degree. The most frequently reported
prognostic factor is the age of the child at the onset of the disease.
Most, but not all, children presenting at younger than 6 years of age
have a good prognosis, whereas those between 6 and 9 years of age have
a variable course. Children older than 9 years of age presenting with
Legg-Calvé-Perthes disease have a worse prognosis than those with an
earlier onset. Within these general guidelines, the disease is quite
variable, and individual prognostication is difficult.
There are several classifications of severity of
Legg-Calvé-Perthes disease. The Catterall classification delineates
four groups based on areas of femoral head involvement (2):
Legg-Calvé-Perthes disease. The Catterall classification delineates
four groups based on areas of femoral head involvement (2):
|
In addition, the presence of two or more risk factors
(extrusion, Gage’s sign, lateral calcification, and a horizontal growth
plate) suggests a worse prognosis.
(extrusion, Gage’s sign, lateral calcification, and a horizontal growth
plate) suggests a worse prognosis.
Because of problems with reproducibility of this
classification, a newer system—the lateral pillar classification—has
come into general use (Table 173.1 and Fig. 173.1, Fig. 173.2 and Fig. 173.3) (12).
In this scheme, the lateral portion of the femoral head is evaluated on
the anteroposterior (AP) radiograph in the early fragmentation stage of
the disease.
classification, a newer system—the lateral pillar classification—has
come into general use (Table 173.1 and Fig. 173.1, Fig. 173.2 and Fig. 173.3) (12).
In this scheme, the lateral portion of the femoral head is evaluated on
the anteroposterior (AP) radiograph in the early fragmentation stage of
the disease.
 |
|
Table 173.1. Lateral Pillar Classification
|
 |
|
Figure 173.1.
Lateral pillar group A classification. AP radiograph of the left hip showing well-demarcated lateral pillar. There is no loss of height in the lateral segment of the femoral head in spite of some changes in radiodensity. |
 |
|
Figure 173.2. Lateral pillar group B classification.
|
 |
|
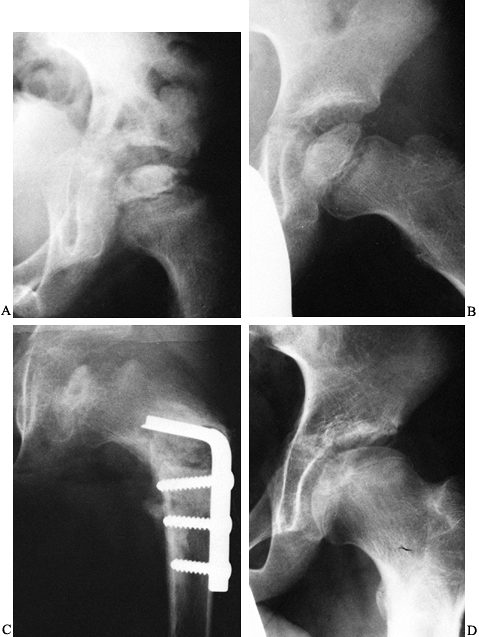
Figure 173.3.
Lateral pillar group C classification. AP radiograph of the pelvis of a boy who has had a varus osteotomy for Legg-Calvé-Perthes disease. A: The lateral portion of the femoral head is lucent and collapsed relative to the central portion. B: AP radiograph 9 months later showing further collapse of the lateral pillar. C: AP radiograph several years later showing flattening of the femoral head. |
The natural history of Legg-Calvé-Perthes disease has
been well studied, and all reports state that the majority of
individuals with the disorder do well through most of their adult lives
(6,10,23). McAndrew and Weinstein (17)
have shown that with follow-up studies of 48 years, about 50% of the
patients will develop severe enough hip disability to require a total
hip replacement by their fifth or sixth decade of life. In these
studies, those with onset of disease after 9 years of age had the
highest incidence of poor results. These studies demonstrate that
long-term prognosis is closely related to the roundness of the femoral
head and the congruity of the hip joint.
been well studied, and all reports state that the majority of
individuals with the disorder do well through most of their adult lives
(6,10,23). McAndrew and Weinstein (17)
have shown that with follow-up studies of 48 years, about 50% of the
patients will develop severe enough hip disability to require a total
hip replacement by their fifth or sixth decade of life. In these
studies, those with onset of disease after 9 years of age had the
highest incidence of poor results. These studies demonstrate that
long-term prognosis is closely related to the roundness of the femoral
head and the congruity of the hip joint.
P.4425
P.4426
TREATMENT CONCEPTS
The earliest treatment efforts for Legg-Calvé-Perthes disease were directed at relief from weight bearing (16).
This was a natural evolution, because in those early days, the disorder
had just been distinguished from tuberculosis, and weight relief was
the mainstay of treatment for tuberculous hips. With time, the concept
of maintaining abduction along with bed rest became the basis for
containment therapy (20). Subsequent studies showed good results with weight-bearing abduction devices, and ambulatory containment was born (11,19).
This was a natural evolution, because in those early days, the disorder
had just been distinguished from tuberculosis, and weight relief was
the mainstay of treatment for tuberculous hips. With time, the concept
of maintaining abduction along with bed rest became the basis for
containment therapy (20). Subsequent studies showed good results with weight-bearing abduction devices, and ambulatory containment was born (11,19).
Salter (24) produced avascular
necrosis in pigs and found that those animals whose hips were kept in
abduction had femoral heads that remained round, whereas the femoral
heads of the untreated animals flattened. Based on this work, surgical
containment, either with femoral or pelvic osteotomy, has been commonly
performed for Legg-Calvé-Perthes disease.
necrosis in pigs and found that those animals whose hips were kept in
abduction had femoral heads that remained round, whereas the femoral
heads of the untreated animals flattened. Based on this work, surgical
containment, either with femoral or pelvic osteotomy, has been commonly
performed for Legg-Calvé-Perthes disease.
INDICATIONS FOR CONTAINMENT TREATMENT
Today there is considerable disagreement among different
centers concerning indications for treatment of Legg-Calvé-Perthes
disease. Our current approach is based on preliminary data from a
long-term multicenter study that compared the treatment methods of
range of motion, bracing, femoral osteotomy, and Salter osteotomy.
centers concerning indications for treatment of Legg-Calvé-Perthes
disease. Our current approach is based on preliminary data from a
long-term multicenter study that compared the treatment methods of
range of motion, bracing, femoral osteotomy, and Salter osteotomy.
We recommend containment treatment for those children who meet the following criteria:
-
Age at onset of disease between 6 and 10 years
-
Lateral pillar group B involvement with bone age at onset of more than 6 years
-
Lateral pillar group C involvement
-
Hips with a reasonable range of motion
We recommend symptomatic treatment for the following:
-
All lateral pillar group A hips
-
Lateral pillar group B hips with a bone age at onset of 6 years or less
-
Any children younger than 6 years of age at the onset of the disease
Symptomatic treatment consists of reduction of
activities when pain and limp worsen, and occasional periods of rest or
traction when necessary for loss of range of motion. Anti-inflammatory
medications are used when necessary. If persistent loss of motion
occurs, a period of a few months of ambulatory abduction bracing may
help the patient maintain range of motion.
activities when pain and limp worsen, and occasional periods of rest or
traction when necessary for loss of range of motion. Anti-inflammatory
medications are used when necessary. If persistent loss of motion
occurs, a period of a few months of ambulatory abduction bracing may
help the patient maintain range of motion.
The treatment of children older than 10 years of age at
onset is difficult. Many surgeons perform containment surgery, with the
caution that all may not go well. These children often lose range of
motion after surgery and may even need abduction casting or bracing
postoperatively. The combination of femoral and pelvic osteotomy may be
appropriate in this age group.
onset is difficult. Many surgeons perform containment surgery, with the
caution that all may not go well. These children often lose range of
motion after surgery and may even need abduction casting or bracing
postoperatively. The combination of femoral and pelvic osteotomy may be
appropriate in this age group.
RESTORATION OF MOTION
It is essential to regain range of motion before
instituting containment treatment. In the child who has had recent
onset of Legg-Calvé-Perthes disease and presents in the early
radiographic stages, motion is usually relatively easily regained.
Often a few days of bed rest are sufficient to regain enough abduction
to “cover” the femoral head radiographically. If the hip is more
resistant to loosening up, then a program of night traction in
abduction may be helpful. After this, bracing or surgical containment
may be instituted.
instituting containment treatment. In the child who has had recent
onset of Legg-Calvé-Perthes disease and presents in the early
radiographic stages, motion is usually relatively easily regained.
Often a few days of bed rest are sufficient to regain enough abduction
to “cover” the femoral head radiographically. If the hip is more
resistant to loosening up, then a program of night traction in
abduction may be helpful. After this, bracing or surgical containment
may be instituted.
The child who has had symptoms for many months and who
has reached the fragmentation stage may require more vigorous methods
to regain motion. Try full-time traction and bed rest and, if these
measures are insufficient, institute a period in Petrie plasters. The
usual procedure is to evaluate the patient under anesthesia and perform
an arthrogram to assess femoral head flattening. If the hip can be
abducted sufficiently to cover the cartilaginous head, apply long-leg
plasters with an abduction bar. If the hip will not abduct, decide
whether “hinge abduction” is occurring. This is a condition in which
the head levers out of the acetabulum with abduction instead of moving
within the socket. If there is hinge abduction, containment surgical
procedures are contraindicated because severe hip stiffness may ensue.
If the head abducts but motion is limited by tight adductor muscles, an
adductor tenotomy may be helpful, followed by the Petrie casts.
has reached the fragmentation stage may require more vigorous methods
to regain motion. Try full-time traction and bed rest and, if these
measures are insufficient, institute a period in Petrie plasters. The
usual procedure is to evaluate the patient under anesthesia and perform
an arthrogram to assess femoral head flattening. If the hip can be
abducted sufficiently to cover the cartilaginous head, apply long-leg
plasters with an abduction bar. If the hip will not abduct, decide
whether “hinge abduction” is occurring. This is a condition in which
the head levers out of the acetabulum with abduction instead of moving
within the socket. If there is hinge abduction, containment surgical
procedures are contraindicated because severe hip stiffness may ensue.
If the head abducts but motion is limited by tight adductor muscles, an
adductor tenotomy may be helpful, followed by the Petrie casts.
SURGICAL CONTAINMENT TREATMENTS
FEMORAL OSTEOTOMY
Some surgeons attempt to obtain sufficient range of
motion to cover the hip before femoral osteotomy, but others perform
the procedure even when there is reduced motion (Fig. 173.4).
Because there is the occasional very stiff hip after the operation, I
recommend that the surgery be performed only in children with at least
30° of hip abduction. In those patients who lack this motion, I regain
range of motion by using Petrie casts for 6 weeks before performing
femoral osteotomy. If the patient has had Legg-Calvé-Perthes disease
for many months, there may be flattening of the femoral head, and thus
I perform an arthrogram before
motion to cover the hip before femoral osteotomy, but others perform
the procedure even when there is reduced motion (Fig. 173.4).
Because there is the occasional very stiff hip after the operation, I
recommend that the surgery be performed only in children with at least
30° of hip abduction. In those patients who lack this motion, I regain
range of motion by using Petrie casts for 6 weeks before performing
femoral osteotomy. If the patient has had Legg-Calvé-Perthes disease
for many months, there may be flattening of the femoral head, and thus
I perform an arthrogram before
P.4427
P.4428
osteotomy.
If the femoral head levers out of the joint with abduction (hinge
abduction), a varus osteotomy is contraindicated. Instead, a trial
period of Petrie casts may be instituted with repeat arthrogram to
determine if the hinge abduction has resolved, in which case the
osteotomy may be performed. Otherwise, other procedures such as valgus
osteotomy may be appropriate in these late cases.
 |
|
Figure 173.4. A 7 1/2-year-old boy with recent onset of symptoms. A:
An anteroposterior radiograph of the left hip showing the risk signs of lucency of the lateral portion of the femoral head, metaphyseal lucency, and lateral widening of the joint space. B: An abduction-internal rotation radiograph of the left hip. There is adequate coverage of the femoral head on this view. Note the subchondral lucency over two thirds of the femoral head, classifying this as a Salter-Thompson type B. There is also lateral calcification, another of Catterall’s risk signs. C: An AP radiograph following a varus proximal femoral osteotomy fixed with a blade plate. The neck-shaft angle is 118°. D: An AP radiograph 4 years after osteotomy showing satisfactory roundness of the femoral head. The blade plate was removed 1 year postoperative. |
The osteotomy is usually performed at the
subtrochanteric level. There are a variety of opinions as to how much
varus and derotation should be used. Some surgeons estimate the amount
of varus based on the amount of abduction required to cover the lateral
portion of the femoral head under the acetabulum. Most surgeons,
however, seek a certain neck-shaft angle regardless of the estimated
coverage. A commonly used angle is 115° to 120°. A greater amount of
varus will result in an abductor limp that may persist. Some remodeling
of the neck-shaft angle will occur in younger children with lesser
involvement, but older children and those with severe disease may not
have the growth capacity to remodel the neck-shaft angle. Rab (22)
has published a review of preoperative radiographic evaluation for
osteotomies about the hip, which is helpful in the planning stage.
subtrochanteric level. There are a variety of opinions as to how much
varus and derotation should be used. Some surgeons estimate the amount
of varus based on the amount of abduction required to cover the lateral
portion of the femoral head under the acetabulum. Most surgeons,
however, seek a certain neck-shaft angle regardless of the estimated
coverage. A commonly used angle is 115° to 120°. A greater amount of
varus will result in an abductor limp that may persist. Some remodeling
of the neck-shaft angle will occur in younger children with lesser
involvement, but older children and those with severe disease may not
have the growth capacity to remodel the neck-shaft angle. Rab (22)
has published a review of preoperative radiographic evaluation for
osteotomies about the hip, which is helpful in the planning stage.
Some surgeons also derotate the femur, based on the
concept that this will improve anterior coverage of the femoral head.
This may cause the patient to out-toe and probably should be done
minimally, if at all. Other surgeons perform a proximal osteotomy, and
extend or anteriorly angulate the osteotomy to improve anterior
coverage.
concept that this will improve anterior coverage of the femoral head.
This may cause the patient to out-toe and probably should be done
minimally, if at all. Other surgeons perform a proximal osteotomy, and
extend or anteriorly angulate the osteotomy to improve anterior
coverage.
Rigidly fix these osteotomies with one of the blade
plates or screw plate devices specifically designed for children.
Immobilize in a cast those patients requiring muscle releases and those
who cannot cooperate with limited weight bearing. (Remember that these
children tend to be extremely active.) See Chapter 166 for more details on the operative technique.
plates or screw plate devices specifically designed for children.
Immobilize in a cast those patients requiring muscle releases and those
who cannot cooperate with limited weight bearing. (Remember that these
children tend to be extremely active.) See Chapter 166 for more details on the operative technique.
Complications often occur because of inadequate fixation
with these active children. Malunion into varus is a serious problem,
which will result in a poor gait. Nonunion, however, is uncommon. The
more severely involved hips may become progressively stiffer following
the osteotomy. When this occurs, the varus of the osteotomy results in
adduction of the thigh. It may be necessary to return the patient to
the operating room for adductor muscle releases and placement of Petrie
casts for a period of time to restore hip range of motion. We have even
had to return patients to brace wear for 6 to 8 weeks to maintain
abduction postoperatively.
with these active children. Malunion into varus is a serious problem,
which will result in a poor gait. Nonunion, however, is uncommon. The
more severely involved hips may become progressively stiffer following
the osteotomy. When this occurs, the varus of the osteotomy results in
adduction of the thigh. It may be necessary to return the patient to
the operating room for adductor muscle releases and placement of Petrie
casts for a period of time to restore hip range of motion. We have even
had to return patients to brace wear for 6 to 8 weeks to maintain
abduction postoperatively.
Remove the fixation plate a year after the osteotomy. At
that time, if there is excessive varus (perhaps less than 110°
neck-shaft angle), an arrest of the greater trochanter may be
appropriate to keep the trochanter below the femoral head.
Occasionally, when excessive varus has been introduced, it may be
necessary to perform a valgus femoral osteotomy subsequently to restore
a normal gait.
that time, if there is excessive varus (perhaps less than 110°
neck-shaft angle), an arrest of the greater trochanter may be
appropriate to keep the trochanter below the femoral head.
Occasionally, when excessive varus has been introduced, it may be
necessary to perform a valgus femoral osteotomy subsequently to restore
a normal gait.
SALTER INNOMINATE OSTEOTOMY
The prerequisites for an innominate osteotomy are similar to those of the femoral osteotomy but are more rigorous (Fig. 173.5).
Salter has recommended that a full range of motion be obtained and that
an arthrogram show no flattening of the femoral head as a prerequisite
to his operation (25,26).
In practice, many surgeons perform the procedure when an adequate range
of motion has been obtained and the flattening of the femoral head is
mild.
Salter has recommended that a full range of motion be obtained and that
an arthrogram show no flattening of the femoral head as a prerequisite
to his operation (25,26).
In practice, many surgeons perform the procedure when an adequate range
of motion has been obtained and the flattening of the femoral head is
mild.
 |
|
Figure 173.5.
An 11-year-old boy with a history of 4 months of right hip discomfort and limp. Children of this age often have the poorest results regardless of treatment. A: Anabduction-internal rotation radiograph showing adequate coverage of the right femoral head. The head is in the phase of increased density, and risk factors have not yet appeared. B: An anteroposterior radiograph 3 months after Salter innominate osteotomy. The pins have been removed, and the osteotomy is healed. The femoral head is showing signs of flattening. C: An AP radiograph 20 months after osteotomy. The femoral head has healed and is reasonably round. D: An AP radiograph 6 years after osteotomy. The femoral head has further flattened over the intervening years. |
The operation is usually performed as originally
described. Salter has emphasized lengthening the iliopsoas to reduce
the pressure on the hip. Some surgeons prefer the Kalamchi modification
of the procedure, which moves the distal fragment of the osteotomy into
a notch in the posterior part of the pelvis (13).
The purpose of this technique is to avoid lengthening the pelvis and
increasing the pressure on the femoral head. Other surgeons add a shelf
of cancellous bone over the femoral head to add to coverage. Most
surgeons immobilize the hips in spica casts for 6 weeks, but some use
screw fixation for the osteotomy and allow partial weight bearing until
the osteotomy has healed. See Chapter 166 for details on operative technique.
described. Salter has emphasized lengthening the iliopsoas to reduce
the pressure on the hip. Some surgeons prefer the Kalamchi modification
of the procedure, which moves the distal fragment of the osteotomy into
a notch in the posterior part of the pelvis (13).
The purpose of this technique is to avoid lengthening the pelvis and
increasing the pressure on the femoral head. Other surgeons add a shelf
of cancellous bone over the femoral head to add to coverage. Most
surgeons immobilize the hips in spica casts for 6 weeks, but some use
screw fixation for the osteotomy and allow partial weight bearing until
the osteotomy has healed. See Chapter 166 for details on operative technique.
An occasional complication of the procedure is hip
stiffness, which at times can be severe. As with the femoral osteotomy,
it may be necessary to perform muscle releases and use Petrie casts and
braces postoperatively to regain range of motion. As with any
osteotomy, it is important to position the osteotomy fragments properly
and obtain secure internal fixation. If the fixation pins or screws are
improperly placed, the osteotomy will displace posteriorly and be
ineffective.
stiffness, which at times can be severe. As with the femoral osteotomy,
it may be necessary to perform muscle releases and use Petrie casts and
braces postoperatively to regain range of motion. As with any
osteotomy, it is important to position the osteotomy fragments properly
and obtain secure internal fixation. If the fixation pins or screws are
improperly placed, the osteotomy will displace posteriorly and be
ineffective.
VALGUS OSTEOTOMY
A valgus osteotomy of the femur is occasionally
indicated for the patient who presents late with well-established head
deformity and hinge abduction (3,21).
The purpose of the osteotomy is to reduce the adduction of the thigh
and allow better weight-bearing alignment. At times, the femoral head
will remodel after this procedure. This should be considered a late,
reconstructive operation and is not appropriate as primary treatment.
See Chapter 29, Chapter 104, and Chapter 166 for details on the operation.
indicated for the patient who presents late with well-established head
deformity and hinge abduction (3,21).
The purpose of the osteotomy is to reduce the adduction of the thigh
and allow better weight-bearing alignment. At times, the femoral head
will remodel after this procedure. This should be considered a late,
reconstructive operation and is not appropriate as primary treatment.
See Chapter 29, Chapter 104, and Chapter 166 for details on the operation.
COMBINED FEMORAL AND PELVIC OSTEOTOMY
The use of combined femoral varus and pelvic osteotomy (either Salter type or Chiari) has been advocated for severely
P.4429
P.4430
involved hips, especially in children older than 9 years of age at the
onset of the disease. The current reports of this approach suggest that
there is an improvement in outcome, but more evaluation is necessary
before this procedure should be done commonly (5,18).
REMOVAL OF LOOSE BODY
Occasionally, a patient with Legg-Calvé-Perthes disease
will develop an osteochondritic lesion, usually many years after the
onset of the disorder. The symptoms of locking and popping suggest the
diagnosis, which then may be confirmed with arthrography or computed
tomography (CT) scanning. Arthroscopy may allow removal of either a
loose body or, more commonly, a softened area in the center of the
femoral head (1,28).
Sometimes an anterior arthrotomy to locate the loose body is
appropriate, but it may be necessary to dislocate the hip to find the
loose body.
will develop an osteochondritic lesion, usually many years after the
onset of the disorder. The symptoms of locking and popping suggest the
diagnosis, which then may be confirmed with arthrography or computed
tomography (CT) scanning. Arthroscopy may allow removal of either a
loose body or, more commonly, a softened area in the center of the
femoral head (1,28).
Sometimes an anterior arthrotomy to locate the loose body is
appropriate, but it may be necessary to dislocate the hip to find the
loose body.
My current approach to the treatment of a patient with
Legg-Calvé-Perthes disease who presents when the disease is in the
phase of increased density or early fragmentation follows: For a child
whose bone age is six years or less, I institute conservative treatment
(rest, anti-inflammatory agents) until there is enough fragmentation to
determine lateral pillar classification. If the patient’s hip is
determined to be class A, I perform no further treatment. If the hip is
determined to be class B, I continue symptomatic treatment, and if it
is Class C, I prefer containment surgery, usually a Salter osteotomy.
Legg-Calvé-Perthes disease who presents when the disease is in the
phase of increased density or early fragmentation follows: For a child
whose bone age is six years or less, I institute conservative treatment
(rest, anti-inflammatory agents) until there is enough fragmentation to
determine lateral pillar classification. If the patient’s hip is
determined to be class A, I perform no further treatment. If the hip is
determined to be class B, I continue symptomatic treatment, and if it
is Class C, I prefer containment surgery, usually a Salter osteotomy.
For a child whose bone age is greater than six years, if
clinical signs are minimal, I observe the patient until I am certain of
a significant degree of disease beyond class A. If significant clinical
signs are present, I allow the patient to regain range of motion
conservatively and consider containment surgery (I prefer Salter
osteotomy).
clinical signs are minimal, I observe the patient until I am certain of
a significant degree of disease beyond class A. If significant clinical
signs are present, I allow the patient to regain range of motion
conservatively and consider containment surgery (I prefer Salter
osteotomy).
In a child older than age 10, decision making is
difficult. I consider containment surgery if the disease is in the
early phase. Usually a Salter osteotomy is performed, sometimes
combined with a proximal femoral varus osteotomy. In children in this
age group, one must recognize that the overall prognosis is poor.
difficult. I consider containment surgery if the disease is in the
early phase. Usually a Salter osteotomy is performed, sometimes
combined with a proximal femoral varus osteotomy. In children in this
age group, one must recognize that the overall prognosis is poor.
REFERENCES
Each reference is categorized according to the following
scheme: *, classic article; #, review article; !, basic research
article; and + , clinical results/outcome study.
scheme: *, classic article; #, review article; !, basic research
article; and + , clinical results/outcome study.
+ 1. Bowen JR, Kumar VP, Joyce JD, Bowen JC. Osteochondritis Dissecans following Perthes’ Disease. Arthroscopic-operative Treatment. Clin Orthop Relat Res 1986;209:49.
* 2. Catterall A. The Natural History of Perthes’ Disease. J Bone Joint Surg 1971;53B:37.
* 3. Catterall A. Legg-Calvé-Perthes Disease. London: Churchill-Livingston, 1982.
! 4. Clancy M, Steel HH. The Effect of an Incomplete Intertrochanteric Osteotomy on Legg-Calvé-Perthes Disease. J Bone Joint Surg 1985;67A:213.
+ 5. Crutcher JP, Staheli LT. Combined Osteotomy as a Salvage Procedure for Severe Legg-Calvé-Perthes disease. J Pediatr Orthop 1992;12:151.
P.4431
* 6. Eaton G. Long-term Results of Treatment in Coxa Plana: A Follow-up Study of Eighty-eight Patients. J Bone Joint Surg 1967;49A:1031.
! 7. Freeman MAR, England JPS. Experimental Infarction of the Immature Canine Femoral Head. Proc R Soc Med 1969;62:431.
! 8. Glueck
C, Crawford A, Roy D, et al. Association of Antithrombotic Factor
Deficiencies and Hypofibrinolysis with Legg-Perthes Disease. J Bone Joint Surg 1996;78A:3.
C, Crawford A, Roy D, et al. Association of Antithrombotic Factor
Deficiencies and Hypofibrinolysis with Legg-Perthes Disease. J Bone Joint Surg 1996;78A:3.
! 9. Glueck
C, Glueck H, Greenfield D, et al. Protein C and S Deficiency,
Thromphilia, and Hypofibrinolysis: Pathophysiologic Causes of
Legg-Perthes Disease. Pediatr Res 1994;35:383.
C, Glueck H, Greenfield D, et al. Protein C and S Deficiency,
Thromphilia, and Hypofibrinolysis: Pathophysiologic Causes of
Legg-Perthes Disease. Pediatr Res 1994;35:383.
* 10. Gower WE, Johnston RC. Legg-Perthes Disease: Long-term Follow-up of Thirty-six Patients. J Bone Joint Surg 1971;53A:759.
* 11. Harrison
MH, Menon MP. Legg-Calvé-Perthes Disease. The Value of Roentgenographic
Measurement in Clinical Practice with Special Reference to the
Broomstick Plaster Method. J Bone Joint Surg 1966;48A:1310.
MH, Menon MP. Legg-Calvé-Perthes Disease. The Value of Roentgenographic
Measurement in Clinical Practice with Special Reference to the
Broomstick Plaster Method. J Bone Joint Surg 1966;48A:1310.
! 12. Herring JA, Neustadt JB, Williams JJ, et al. The Lateral Pillar Classification of Legg-Calvé-Perthes Disease. J Pediatr Orthop 1992;12:143.
+ 13. Kalamchi A. A Modified Salter Osteotomy. J Bone Joint Surg 1982;64A:183.
! 14. Kasser
JR, Hresko T, McDougall PA, et al. Prospective Re-evaluation of the
Association between Thrombotic Diathesis and Legg-Calvé-Perthes
Disease. Pediatric Orthopaedics Society of North America (POSNA) 1998 Annual Meeting. Cleveland, 1998, p 96.
JR, Hresko T, McDougall PA, et al. Prospective Re-evaluation of the
Association between Thrombotic Diathesis and Legg-Calvé-Perthes
Disease. Pediatric Orthopaedics Society of North America (POSNA) 1998 Annual Meeting. Cleveland, 1998, p 96.
! 15. Kendig RJ, Evans GA. Biologic Osteotomy in Perthes Disease. J Pediatr Orthop 1986;6:278.
* 16. Legg AT. An obscure affection of the hip joint. Boston Med Surg J 1910;162:202.
* 17. McAndrew MP, Weinstein SL. A Long-term Follow-up of Legg-Calvé-Perthes Disease. J Bone Joint Surg 1984;66:860.
+ 18. Olney BW, Asher MA. Combined Innominate and Femoral Osteotomy for the Treatment of Severe Legg-Calvé-Perthes Disease. J Pediatr Orthop 1985;5:645.
* 19. Petrie JG, Bitenc I. The abduction weight-bearing treatment in Legg-Perthes’s disease. J Bone Joint Surg 1971;53B:54.
* 20. Pike MM. Legg-Perthes Disease: A Method of Conservative Treatment. J Bone Joint Surg 1950;32A:663.
+ 21. Quain S, Catterall A. Hinge Abduction of the Hip: Diagnosis and Treatment. J Bone Joint Surg 1986;68B:61.
* 22. Rab G. Preoperative Roentgenographic Evaluation for Osteotomies about the Hip in Children. J Bone Joint Surg 1981;63A:306.
* 23. Ratliff AH. Perthes’ Disease: A Study of Thirty-four Hips Observed for Thirty Years. J Bone Joint Surg 1967;49B:102.
! 24. Salter R. Experimental and Clinical Aspects of Perthes’ Disease. J Bone Joint Surg 1966;48B:393.
* 25. Salter RB. Legg-Perthes Disease: The Scientific Basis for the Methods of Treatment and Their Indications. Clin Orthop Relat Res 1980;150:8.
* 26. Salter RB. The Present Status of Surgical Treatment for Legg-Perthes Disease. J Bone Joint Surg 1984;66A:961.
! 27. Sanchis
M, Zahir A, Freeman MA. The Experimental Stimulation of Perthes Disease
by Consecutive Interruptions of the Blood Supply to the Capital Femoral
Epiphysis in the Puppy. J Bone Joint Surg 1973;55A:335.
M, Zahir A, Freeman MA. The Experimental Stimulation of Perthes Disease
by Consecutive Interruptions of the Blood Supply to the Capital Femoral
Epiphysis in the Puppy. J Bone Joint Surg 1973;55A:335.
+ 28. Schindler
A, Lechevallier J, Rao N, Bowen J. Diagnostic and Therapeutic
Arthroscopy of the Hip in Children and Adolescents: Evaluation of
Results. J Pediatr Orthop 1995;15:317.
A, Lechevallier J, Rao N, Bowen J. Diagnostic and Therapeutic
Arthroscopy of the Hip in Children and Adolescents: Evaluation of
Results. J Pediatr Orthop 1995;15:317.
* 29. Stulberg SD, Cooperman DR, Wallensten R. The Natural History of Legg-Calvé-Perthes disease. J Bone Joint Surg 1981;63A:1095.
* 30. Waldenström H. On Coxa Plana. Acta Chir Scand 1923;55:557.