
Editors: Chelly, Jacques E.
Title: Peripheral Nerve Blocks: A Color Atlas, 3rd Edition
Copyright ©2009 Lippincott Williams & Wilkins
> Table of Contents > Section IV – Ultrasound > 38 – Ultrasound Guided Obturator Nerve Block
38
Ultrasound Guided Obturator Nerve Block
Andrew Gray
Julie Soong
The lateral adductor brevis muscle. The anterior division of the
obturator nerve usually lies superficial to the adductor brevis muscle.
The posterior division of the nerve usually lies deep to the adductor
brevis muscle. Both divisions produce broad, flat, hyperechoic images
at the lateral border of the adductor brevis muscle. The obturator
artery, which is sandwiched between the obturator internus and externus
muscles.
Sterile prep of the skin. The transducer is placed in the axial plane
and the needle is inserted at a steep angle, in plane, at the lateral
border of the transducer. The anterior division is identified
superficial to the adductor brevis muscle and the posterior division
P.292
is
identified deep to the adductor brevis muscle. The needle is advanced
under direct vision until a medial contraction is observed at a current
of 0.5 mA. Injection proceeds until the posterior division is
surrounded by a hypoechoic ring. Five mL of local anesthetic usually
suffices. The needle is withdrawn and directed toward the anterior
division. Injection of local anesthetic proceeds until the anterior
division is surrounded by local anesthetic.
 |
|
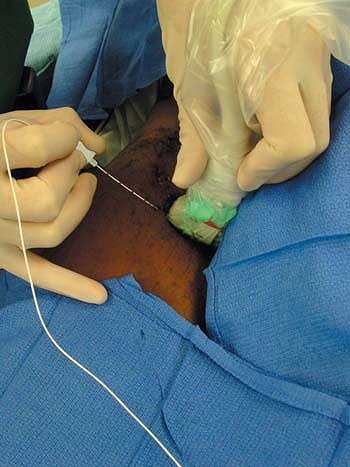
Figure 38-1. Photograph of the position of the ultrasound transducer for short axis (transverse cross section)
imaging and in-plane needle placement for obturator nerve block. The patient is supine with the ipsilateral leg straight and slightly externally rotated. In this example, an insulated 5-cm, 22-gauge block needle is used to confirm nerve identity with evoked motor response. |
 |
|
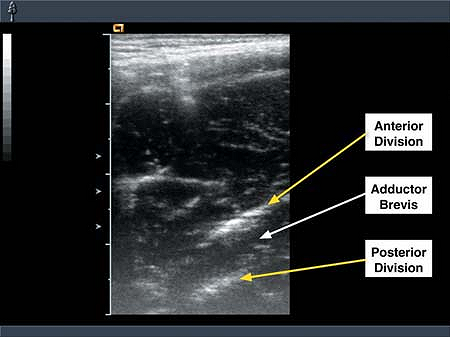
Figure 38-2.
Sonogram of the obturator nerve divisions in the medial thigh. The anterior and posterior divisions are seen in short axis view (transverse cross section) separated by the adductor brevis muscle. Large tick marks are 10 mm apart. |
P.293
-
The femoral vein and lymphatics lie close to the needle path. Care should be taken to avoid these when possible.
-
Puncture of the obturator artery has led to intraperitoneal or retroperitoneal hemorrhage.
-
In some patients, the divisions can be
traced proximally. The anterior division usually lies anterior to the
obturator externus. The posterior division usually lies deep to the
obturator externus muscle or pierces the obturator externus before
running behind this muscle (Fig. 38-2).
Suggested Reading
Gray AT. Ultrasound-guided regional anesthesia: current state of the art. Anesthesiology 2006; 104:368–373.