
Editors: Frassica, Frank J.; Sponseller, Paul D.; Wilckens, John H.
Title: 5-Minute Orthopaedic Consult, 2nd Edition
Copyright ©2007 Lippincott Williams & Wilkins
> Table of Contents > Snapping Hip
Snapping Hip
Paul D. Sponseller MD
Description
-
Snapping of the hip is a sensation that is normally felt on an infrequent basis by many people.
-
If it becomes frequent or painful, patients may seek attention and treatment.
-
The causes may include structures outside or inside the joint.
-
-
Synonyms: Popping hip; Tendinitis; Coxa saltans
General Prevention
-
Perform adequate stretching before and after sports.
-
Avoid frequent intramuscular injections into the gluteal muscles.
Epidemiology
-
Snapping of the hip may occur at any age, including in the elderly.
-
It is slightly more common in females than in males.
Incidence
-
Uncommon clinical problem
-
No statistics on frequency or prevalence
Risk Factors (1,2,3,4)
-
Coxa vara, or decreased angle of the
femoral neck, renders the greater trochanter more prominent and
increases the risk of snapping. -
Another risk factor is a history of
multiple intramuscular injections into the buttock, which may cause
fibrosis of the gluteus and, in turn, may predispose to snapping. -
Athletes who increase their training to an extreme degree may also develop this condition.
Genetics
No known genetic predisposition exists.
Etiology
-
Internal:
-
A structure in front of the joint, such
as the psoas tendon, causes the snapping by riding over the front of
the femoral head or the pubic ramus.
-
-
External:
-
May be from snapping of the iliotibial band or the anterior fibers of the gluteus maximus riding over the greater trochanter.
-
May follow multiple intramuscular
injections into the buttock, which render the gluteus and iliotibial
band fibrotic and contracted.
-
-
Intra-articular:
-
Includes loose bodies or a tear in the acetabular labrum, which may cause sensation of snapping or clicking.
-
Rarely, may occur after total hip arthroplasty secondary to malposition or loosening of the femoral component.
-
Associated Conditions
Snapping hip usually occurs in isolation and is not related to any systemic conditions or other skeletal problems.
Signs and Symptoms
-
The patient has a sensation of muscle jumping over the front or the side of the hip.
-
The patient may be able to point to the location of snapping, thus aiding in the diagnosis.
-
-
The patient may have difficulty getting into or arising from a squat.
-
The diagnosis may be confirmed by
blocking the movement of the psoas or the iliotibial band during
flexion and extension of the hip.
History
-
Patients note the spontaneous onset of snapping or popping of the hip, usually in the absence of trauma.
-
It is more common in athletes than in the general population, and typically begins in the juvenile or adolescent period (1,2).
-
Ask the patient about what activity or position produces the snapping, and its frequency.
Physical Exam
-
Ask the patient to point to the area where the snapping is felt.
-
This procedure is helpful in distinguishing snapping of the iliotibial band (lateral) from the psoas (anteriorly).
-
-
Ask the patient if, he/she can reproduce the snapping.
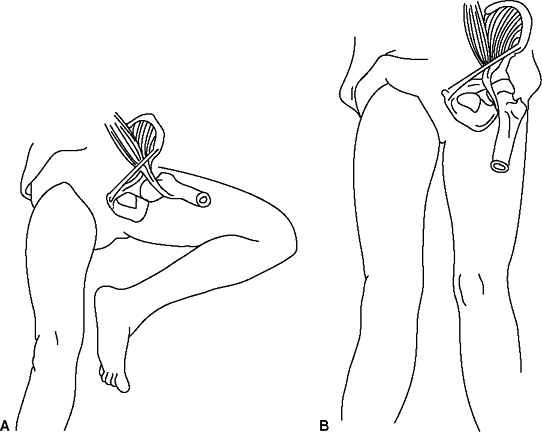 Fig. 1. Artist’s sketch of movement of the iliopsoas tendon during snapping hip. A: The tendon is lateral to the pelvic brim with the hip in flexion and abduction. B:
Fig. 1. Artist’s sketch of movement of the iliopsoas tendon during snapping hip. A: The tendon is lateral to the pelvic brim with the hip in flexion and abduction. B:
Snapping hip is reproduced as the tendon moves to a more medial
position on the pelvic brim with extension and adduction of the hip.
(Reprinted with permission of Dobbs MB, Gordon JE, Luhmann SJ, et al.
Surgical correction of the snapping iliopsoas tendon in adolescents. J Bone Joint Surg 2002;84A:420–424.) -
For psoas tendon snapping over the pectineal eminence, the “figure 4” test is helpful.
-
This test consists of the patient
actively moving the affected hip from extension to a “figure 4” or
flexed and abducted position while keeping the foot in the midline (Fig. 1) (1).
-
-
To test for the snapping iliotibial band,
the patient is placed in the lateral position on the opposite hip, and
the hip in question is flexed and extended in progressively greater
adduction.-
Note the presence of abduction contracture, reproduction of symptoms, and actual snapping.
-
Tests
Imaging
-
Plain radiography of the pelvis is indicated to rule out any bony abnormality of the pelvis or joint.
-
CT scan may be helpful if a structural abnormality is found.
-
Ultrasound has been reported to document dynamically the snapping and possibly to guide injection, but it requires experience (1,5).
-
Iliopsoas bursography is done under fluoroscopy, with contrast medium injected anteriorly into the bursa.
-
If the psoas tendon is the cause, it may be seen to flip over the front of the hip corresponding with the symptoms.
-
Psoas tendon and bursa can be injected with steroid and lidocaine at this time.
-
If the injection relieves symptoms, it is additional confirmation of the diagnosis.
-
-
Injection of the greater trochanteric bursa does not require imaging but is a helpful confirmatory test.
-
A hip arthrogram, combined with CT scan may be helpful in diagnosing a torn acetabular labrum.
-
MRI may be helpful to rule out other conditions or diagnose acetabular labral tears (5,6).
P.407
Diagnostic Procedures/Surgery
Hip arthroscopy may be useful in confirming an intra-articular cause and treating a torn labrum or loose body.
Pathological Findings
-
Internal type of snapping hip:
-
The psoas and iliacus tendons ride in a shallow groove between the iliopectineal eminence and the anterior inferior iliac spine.
-
They may cause snapping by riding over each other, over the psoas bursa, or over the bone during flexion and extension.
-
-
The iliotibial band attaches to the tensor fasciae latae and the gluteus maximus and minimus.
-
It remains taut during flexion and extension, and it rides over the trochanteric bursa.
-
Any thickening of this bursa, or increasing tension of the tendon, may contribute to the snapping.
-
Differential Diagnosis
-
Snapping of the meniscus may masquerade as snapping hip because the hip and knee usually flex together.
-
Exostosis around the hip may contribute to snapping.
-
Habitual hip subluxation in children and adolescents is an uncommon phenomenon, which may be confused with a snapping hip.
General Measures
-
Injection into the appropriate region is an intermittent step between physical therapy and surgery.
-
It may be done using a mixture of local
anesthetics (e.g., lidocaine) to confirm the diagnosis and steroids to
interrupt the inflammatory cycle and perhaps provide permanent relief.
-
-
Make the diagnosis by physical examination and imaging.
-
The extent of treatment depends on how much snapping bothers the patient.
-
If the snapping is severe, the following are advised:
-
Avoidance of provocative activities
-
Stretching exercises
-
Anti-inflammatory medications
-
Injection with steroids may be repeated every 6 months.
-
Surgery
-
-
-
The patient should refrain from
activities involving flexion and extension, or adduction (such as
running on the side of an incline), which may predispose to snapping.
Special Therapy
Physical Therapy
Stretching the iliotibial band or psoas tendon may alleviate the problem.
Medication
First Line
-
NSAIDs:
-
Dosing schedules vary from quick-onset, short duration, to once-a-day agents, which are less effective for acute pain.
-
Gastrointestinal upset is a possible side
effect, and these drugs are to be used cautiously in patients with a
history of gastric ulcer disease.
-
-
Narcotics should be avoided.
Surgery
-
If other measures do not help, surgery may be offered, depending on the underlying cause.
-
If the cause is the iliotibial band, it can be incised over the greater trochanter to relieve the pressure.
-
If the cause is the psoas tendon, it may be lengthened at the pelvic brim.
-
-
Surgery is reserved for the most
recalcitrant cases because the results are unpredictable when no
structural abnormalities have been identified. -
Intra-articular factors, such as a loose body or a torn acetabular labrum, may be dealt with appropriately.
Prognosis
-
Usually not a long-standing problem
-
Does not lead to arthritis
Complications
-
Failure to improve is the most common complication (1).
-
Femoral neuropathy is another possible risk of psoas lengthening.
Patient Monitoring
Because this condition is benign, patients may be allowed to self-monitor and return for follow-up if symptoms warrant.
References
1. Dobbs MB, Gordon JE, Luhmann SJ, et al. Surgical correction of the snapping iliopsoas tendon in adolescents. J Bone Joint Surg 2002;84A: 420–424.
2. Lyons JC, Peterson LFA. The snapping iliopsoas tendon. Mayo Clin Proc 1984;59:327–329.
3. Schaberg JE, Harper MC, Allen WC. The snapping hip syndrome. Am J Sports Med 1984;12: 361–365.
4. Wahl
CJ, Warren RF, Adler RS, et al. Internal coxa saltans (snapping hip) AS
a result of overtraining. A report of 3 cases in professional athletes
with a review of causes and the role of ultrasound in early diagnosis
and management. Am J Sports Med 2004;32:1302–1309.
CJ, Warren RF, Adler RS, et al. Internal coxa saltans (snapping hip) AS
a result of overtraining. A report of 3 cases in professional athletes
with a review of causes and the role of ultrasound in early diagnosis
and management. Am J Sports Med 2004;32:1302–1309.
5. Shabshin N, Rosenberg ZS, Cavalcanti CFA. MR imaging of iliopsoas musculotendinous injuries. Magn Reson Imaging Clin N Am 2005;13: 705–716.
6. Tatu
L, Parratte B, Vuillier F, et al. Descriptive anatomy of the femoral
portion of the iliopsoas muscle. Anatomical basis of anterior snapping
of the hip. Surg Radiol Anat 2001;23:371–374.
L, Parratte B, Vuillier F, et al. Descriptive anatomy of the femoral
portion of the iliopsoas muscle. Anatomical basis of anterior snapping
of the hip. Surg Radiol Anat 2001;23:371–374.
Codes
ICD9-CM
-
719.65 Snapping hip
-
726.0 Bursitis
Patient Teaching
The phenomenon of a snapping tendon or other structure,
including the rationale for rest and stretching, should be explained to
the patient.
including the rationale for rest and stretching, should be explained to
the patient.
FAQ
Q: Is snapping hip likely to lead to arthritis?
A: No. It does not normally lead to arthritis because most causes are outside the joint.