
Editors: Frassica, Frank J.; Sponseller, Paul D.; Wilckens, John H.
Title: 5-Minute Orthopaedic Consult, 2nd Edition
Copyright ©2007 Lippincott Williams & Wilkins
> Table of Contents > Hip Anatomy and Examination
Hip Anatomy and Examination
Timothy S. Johnson MD
Lawrence A. McGuigan PA-C, MMS
Description
-
Bones (Fig. 1):
-
Pelvis and femur bone
-
The acetabulum is the “socket.”
-
-
Muscles:
-
Flexors: Iliopsoas, sartorius, rectus femoris
-
Extensors: Gluteus maximus, hamstring muscles
-
Abductors: Gluteus medius, gluteus minimus
-
Adductors: Gracilis, pectineus, adductor longus, adductor brevis, adductor magnus
-
-
Nerves:
-
Femoral: Hip flexors
-
Obturator: Adductors
-
Superior gluteal: Abductors
-
-
Ligaments:
-
Sacroiliac: Sacrum to ilium
-
Sacrotuberous: Sacrum to ischial tuberosity
-
Sacrospinous: Sacrum to ischial spine
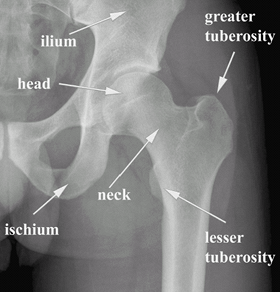 Fig. 1. AP radiograph of a left hip.
Fig. 1. AP radiograph of a left hip.
-
Signs and Symptoms
History
Thorough history of the mechanism of injury and nature of pain
Physical Exam (1)
-
Initial procedures:
-
Have the patient disrobe.
-
Examine the lumbar spine.
-
Examine the knee.
-
Check the neurovascular status.
-
-
Standing inspection:
-
Compare the height of the iliac crests in the horizontal plane. (Asymmetry suggests leg-length discrepancy.)
-
Look for muscle atrophy and correlate with gait inspection, if possible.
-
-
Gait inspection (2):
-
Observe for asymmetry between left and right.
-
Antalgic gait: Shortened stride and decreased stance phase on the affected leg
-
Make note of pain and endurance.
-
Trendelenburg limp:
 Fig. 2. AP radiograph of a right hip with osteoarthritis.
Fig. 2. AP radiograph of a right hip with osteoarthritis.-
Evaluate for pelvic tilt during the stance phase of gait.
-
Positive finding occurs when the patient
leans to the affected side, placing the center of gravity over the hip
and effectively unloading the abductor muscles.
-
-
-
Supine examination:
-
Look for leg-length discrepancy (measure
from the inferior edge of the anterior superior iliac spine to the
inferior edge of the medial malleolus on both sides). -
Compare active and passive ROM.
-
Hip flexion: 110–120°
-
Hip extension: 10–15°
-
Abduction: 45–50°
-
Adduction: 20–30°
-
Internal rotation: 15–45°
-
External rotation: 40–65°
-
Extension: 30°
-
Note guarding, pain, and spasm.
-
-
-
Antalgic gait may be caused by hip, back, or other lower limb problems.
-
Weakness, muscle atrophy, decreased sensation, and asymmetric deep tendon reflexes suggest spine abnormality.
-
Osteoarthritis of the hip (3) (Fig. 2):
-
Typically presents with start-up pain, morning stiffness, and deep groin pain
-
Hip flexion with simultaneous internal rotation reproduces groin pain.
-
Presents with decreased active and passive ROM:
-
Hip flexion contracture is common
-
-
Radiographs: Joint space narrowing and osteophyte formation
-
-
Greater trochanteric bursitis:
-
Typically presents as lateral hip pain
-
Patients are exquisitely tender to palpation of greater trochanter.
-
Resisted hip abduction reproduces lateral hip pain.
-
-
Buttock and posterior hip pain:
-
Indicates lumbar spine abnormality until proven otherwise
-
Radicular pain produced by deep palpation of the sciatic nerve differentiates sciatica from intra-articular abnormality.P.179
-
With the patient in the lateral decubitus position, flex the hip and knee to 90°.
-
Palpate the nerve midway between the greater trochanter and the ischium.
-
-
-
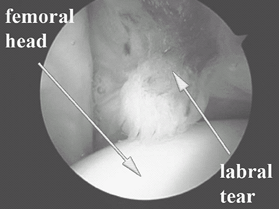
Labral tears/femoroacetabular impingement (4) (Fig. 3):
-
Young athletic patients
-
Typically presents as groin pain during or after activity
-
Hip flexion with simultaneous internal rotation reproduces groin pain.
-
Radiographs may be normal.
-
MRI can confirm diagnosis.
-
Examine for and rule out inguinal hernia.
![]() Fig. 3. Arthroscopic photograph of a labral tear.
Fig. 3. Arthroscopic photograph of a labral tear.
-
Tests
-
Trendelenburg test (to evaluate strength of the gluteus medius muscle):
-
Have the patient perform a single-leg stand on the affected side and try to maintain the pelvis level with the floor.
-
If the pelvis tilts to maintain the
single-leg stand, it is a sign of abductor weakness or hip joint pain,
and the test is positive.
-
-
Thomas test (to evaluate flexion contracture):
-
With the patient supine, place your hand under the lumbar spine and bring 1 leg up into full flexion.
-
Have the patient hold it there by grasping the knee with both hands.
-
Bring the other leg into full extension.
-
Any loss of extension is a flexion contracture.
-
References
1. DeAngelis NA, Busconi BD. Assessment and differential diagnosis of the painful hip. Clin Orthop Relat Res 2003;406:11–18.
2. Perry J. Pathologic gait. Instr Course Lect 1990;39: 325–331.
3. Hoaglund FT, Steinbach LS. Primary osteoarthritis of the hip: etiology and epidemiology. J Am Acad Orthop Surg 2001;9:320–327.
4. Scopp JM, Moorman CT, III. The assessment of athletic hip injury. Clin Sports Med 2001;20: 647–659.
Additional Reading
Hoppenfeld S. Physical examination of the hip and pelvis. In: Physical Examination of the Spine & Extremities. Norwalk, CT: Appleton & Lange, 1976:143–169.
Hoppenfeld S, deBoer P. The hip and acetabulum. In: Surgical Exposures in Orthopaedics: The Anatomical Approach, 3rd ed. Philadelphia: Lippincott, Williams & Wilkins, 2003:365–453.
Moore KL, Dalley AF, II. Lower limb. In: Clinically Oriented Anatomy, 4th ed. Philadelphia: Lippincott Williams & Wilkins, 1999:503–663.
FAQ
Q: What is the most common cause of lateral hip pain?
A: Greater trochanteric bursitis.
Q: Arthritis of the hip joint usually presents with complaints of pain in which area of the hip?
A: The groin.