
Authors: Doyle, James R.
Title: Hand and Wrist, 1st Edition
Copyright ©2006 Lippincott Williams & Wilkins
> Table of Contents > Section III – Emergency Department > 16 – Injection Injuries
16
Injection Injuries
Injection injuries may occur secondary to penetration of
the skin by fluids under high pressure, therapeutic injections
(infusions) of chemotherapeutic agents, or self-injection of various
narcotic agents in addiction.
the skin by fluids under high pressure, therapeutic injections
(infusions) of chemotherapeutic agents, or self-injection of various
narcotic agents in addiction.
High-Pressure Injection Injuries
History
These injuries are most often seen in commercial
painters, mechanics, heavy equipment operators, and others who work
with various fluids under high pressure. The fluids or materials
involved may be paint or paint solvents, grease, or hydraulic fluids
under high pressure. A common history is that of a painter cleaning his
spray gun at the end of the day and checks to see if the gun is clean
by spraying the tip of his finger to see if the resultant spray is
clear. A similar scenario is that of a heavy equipment operator who
notes a leak in a hydraulic line and tries to correct it by holding a
rag around the leak. Yet another scenario is the mechanic who wants to
know if he still has some grease in his gun, and therefore places the
tip of the grease gun on the tip of his finger and pulls the release
trigger.
painters, mechanics, heavy equipment operators, and others who work
with various fluids under high pressure. The fluids or materials
involved may be paint or paint solvents, grease, or hydraulic fluids
under high pressure. A common history is that of a painter cleaning his
spray gun at the end of the day and checks to see if the gun is clean
by spraying the tip of his finger to see if the resultant spray is
clear. A similar scenario is that of a heavy equipment operator who
notes a leak in a hydraulic line and tries to correct it by holding a
rag around the leak. Yet another scenario is the mechanic who wants to
know if he still has some grease in his gun, and therefore places the
tip of the grease gun on the tip of his finger and pulls the release
trigger.
Pathomechanics of Injury
All of the above described scenarios result in the easy
penetration of the skin envelope by the various high-pressure fluids.
The materials fill the tissue spaces and travel along fascial planes in
the line of least resistance. They are very injurious to the tissues,
and that—combined with the mechanical factors of increased tissue
pressure—produces ischemia and tissue necrosis. Latex or water-based
paint is the least noxious of the listed materials, but are still
associated with significant soft tissue changes.
penetration of the skin envelope by the various high-pressure fluids.
The materials fill the tissue spaces and travel along fascial planes in
the line of least resistance. They are very injurious to the tissues,
and that—combined with the mechanical factors of increased tissue
pressure—produces ischemia and tissue necrosis. Latex or water-based
paint is the least noxious of the listed materials, but are still
associated with significant soft tissue changes.
Diagnosis and Physical Findings
-
The diagnosis is made by the history of what at first may seem a very minimal injury that later develops into a major problem with pain that may be out of proportion to the physical findings.
-
These patients may be seen in an
emergency room setting. The initial findings may not be very striking
in terms of appearance of the digit or hand, but as the condition
develops they may be associated with severe pain. -
The worker may be hesitant to admit the true mechanism of the injury due to embarrassment.
-
The initial physical findings may be
negligible, with little or no evidence of penetration except for some
swelling in the digit or palm. -
As the chemical irritation develops, there is increased swelling and signs of inflammation. Pain becomes a major factor.
Treatment
-
Treatment consists of early decompression through appropriate incisions.
-
The aim is to decompress the involved area and to remove as much of the injected material as possible.
-
Amputation may be avoided by early
treatment that includes wide debridement, open drainage, repeat
debridement as indicated, and delayed wound closure (Figure 16-1).
Prognosis
-
These injuries result in severe tissue ischemia with necrosis, which may result in amputation.
-
Rates of amputation vary from 16% to 48%.
-
The outcome from these injuries depends
on the type and amount of material injected, the presence of infection,
and the interval between injury and removal of the injected material. -
Stiffness is a recognized complication, and the overall prognosis is guarded in these injuries.
Therapeutic Injection Injuries
Injections or infusions are ordinarily safe, but may
lead to serious problems because of incorrect placement of needles or
catheters, or because of fluid extravasation with tissue necrosis. The
latter complication may be seen with
lead to serious problems because of incorrect placement of needles or
catheters, or because of fluid extravasation with tissue necrosis. The
latter complication may be seen with
P.250
intravenous
chemotherapeutic agents used in cancer therapy, and may result in
significant soft tissue loss that requires appropriate soft tissue
coverage.
 |
|
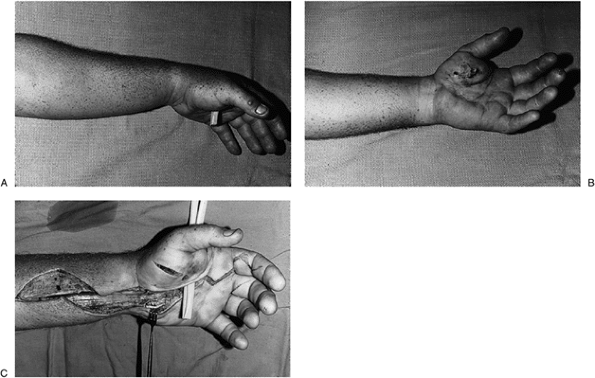
Figure 16-1 A, B.
This 25-year-old, left-handed backhoe operator detected a small leak in one of the hydraulic lines on the machine, and attempted to stop it by forcibly holding an oil rag over the leak. He felt a stinging sensation in his hand and let go of the line. About 2 hours later he had increasing pain in his left hand and went to a local emergency room, where his pain was considered to be “inappropriate.” He was sent home with pain pills. Later that night he was diagnosed with a hydraulic fluid injection injury; the site of entry at the thenar eminence was opened through a small incision, and a small drain inserted. C. Further consultation revealed the extensive nature of the injury, and a comprehensive decompression was performed both to remove additional hydraulic fluid and to debride the wound. Delayed wound closure was performed at a later date, and his residuals were those of mild to moderate stiffness in the left thumb. |
Medications designed for intravenous use mistakenly
placed into an artery may result in arterial spasm with muscle ischemia
and necrosis. Nerve injuries have been observed in the forearm
following extravasation of physiologic intravenous fluids used for
rehydration, due to increased hydrostatic pressure rather than any
toxicity specific to the fluid. Steroid injection used for treatment of
carpal tunnel syndrome, if placed intrafascicularly, may have an
adverse effect on nerve function.
placed into an artery may result in arterial spasm with muscle ischemia
and necrosis. Nerve injuries have been observed in the forearm
following extravasation of physiologic intravenous fluids used for
rehydration, due to increased hydrostatic pressure rather than any
toxicity specific to the fluid. Steroid injection used for treatment of
carpal tunnel syndrome, if placed intrafascicularly, may have an
adverse effect on nerve function.
Self-Inflicted Injection Injuries
These injuries may present in a variety of ways because
many different agents may be used. The portal may or may not be readily
evident. Manifestations include infection, edema, and chronic
induration of soft tissues. Portals may be intravenous or
intra-arterial. If sufficient changes are produced in the arterial
lining or wall, ischemia or necrosis may be seen.
many different agents may be used. The portal may or may not be readily
evident. Manifestations include infection, edema, and chronic
induration of soft tissues. Portals may be intravenous or
intra-arterial. If sufficient changes are produced in the arterial
lining or wall, ischemia or necrosis may be seen.
Suggested Reading
Frederick
HA, Carter PR, Littler JW. Injection injuries to the median and ulnar
nerves at the wrist. J Hand Surg 1992;17A:645–647.
HA, Carter PR, Littler JW. Injection injuries to the median and ulnar
nerves at the wrist. J Hand Surg 1992;17A:645–647.
MacKinnon
SE, Hudson AR, Gentili F, et al. Peripheral nerve injection injury with
steroid agents. Plastic Reconstr Surg 1982;69:482–489.
SE, Hudson AR, Gentili F, et al. Peripheral nerve injection injury with
steroid agents. Plastic Reconstr Surg 1982;69:482–489.
Pinto
MR, Turkula-Pinto LD, Cooney WP, et al. High-pressure injection
injuries of the hand: review of 25 patients managed by open wound
technique. J Hand Surg 1993;18A:125–130.
MR, Turkula-Pinto LD, Cooney WP, et al. High-pressure injection
injuries of the hand: review of 25 patients managed by open wound
technique. J Hand Surg 1993;18A:125–130.
Stanley D, Connolly WB. Iatrogenic injection injuries of the hand and upper limb. J Hand Surg 1992;17B:442–46.