
Authors: Koval, Kenneth J.; Zuckerman, Joseph D.
Title: Handbook of Fractures, 3rd Edition
Copyright ©2006 Lippincott Williams & Wilkins
> Table of Contents > V – Pediatric Fractures and Dislocations > 42 – Pediatric Orthopedic Surgery: General Principles
42
Pediatric Orthopedic Surgery: General Principles
Overview
-
The development and growth of the
skeletal system from gestation to skeletal maturity create interrelated
fibrous, tendinous, cartilaginous, and osseous changes resulting in
patterns of susceptibility and reparative response that distinguish the
pediatric patient from the adult. -
As a rule, the younger the patient, the
greater the remodeling potential; thus, absolute anatomic reduction in
a child is less important than in a comparable injury in an adult.
EPIDEMIOLOGY
-
The overall mortality rate of children
has fallen from 1 in 250 per year in 1900 to 1 in 4,000 per year in
1986; this has been attributed to improved public education, preventive
devices, and medical care. -
The leading cause of death in children age 1 to 14 is accidental trauma.
-
Skeletal trauma accounts for 10% to 15%
of all childhood injuries, with approximately 15% to 30% of these
representing physeal injuries (phalanx fractures are the most common
physeal injury). -
Over the past 50 years, the increasing
fracture incidence in children has been mainly attributed to increased
sports participation. -
From the ages of 0 to 16 years, 42% of boys will sustain at least one fracture compared with 27% of girls.
-
The overall ratio of boys to girls who
sustain a single, isolated fracture is 2.7:1. The peak incidence of
fractures in boys occurs at age 16 years, with an incidence of 450 per
10,000 per year; the peak incidence in girls occurs at age 12 years,
with an incidence of 250 per 10,000 per year. -
Open fractures in this population are rare (<5%).
ANATOMY
-
Pediatric bone has a higher water content
and lower mineral content per unit volume than adult bone. Therefore,
pediatric bone has a lower modulus of elasticity (less brittle) and a
higher ultimate strain-to-failure than adult bone. -
The physis (growth plate) is a unique
cartilaginous structure that varies in thickness depending on age and
location. It is frequently weaker than bone in torsion, shear, and
bending, predisposing the child to injury through this delicate area. -
The physis is traditionally divided into
four zones: reserve (resting/germinal), proliferative, hypertrophic,
and provisional calcification (or enchondral ossification) (Fig. 42.1). -
The periosteum in a child is a thick fibrous structure (up to several millimeters) that encompasses the entire bone except the
P.472
articular ends. The periosteum thickens and is continuous with the
physis at the perichondral ring (ring of LaCroix), offering additional
resistance to shear force.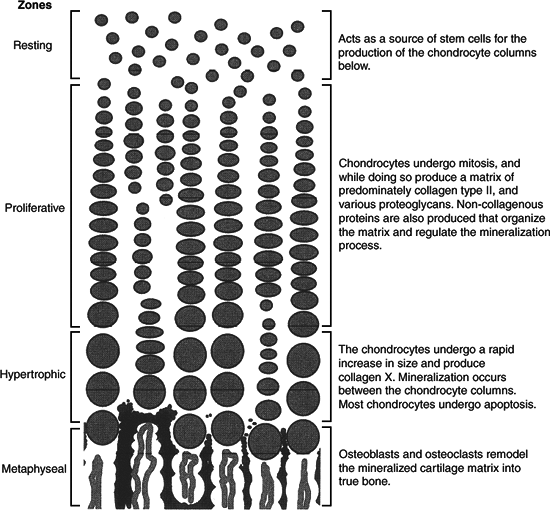 Figure
Figure
42.1. The figure shows the process of endochondral ossification within
the physis. Although not as organized, endochondral ossification
follows a similar pattern during fracture repair.(From Bucholz RW, Heckman JD, Court-Brown C, et al., eds. Rockwood and Green’s Fractures in Adults, 6th ed. Philadelphia: Lippincott Williams & Wilkins, 2006.) -
As a general rule, ligaments in children
are functionally stronger than bone. Therefore, a higher proportion of
injuries that produce sprains in adults result in fractures in children. -
The blood supply to the growing bone
includes a rich metaphyseal circulation with fine capillary loops
ending at the physis (in the neonate, small vessels may traverse the
physis, ending in the epiphysis).
MECHANISM OF INJURY
-
Because of structural differences,
pediatric fractures tend to occur at lower energy than adult fractures.
Most are a result of compression, torsion, or bending moments. -
Compression fractures are found most
commonly at the metaphyseal diaphyseal junction and are referred to as
“buckle fractures” or “torus fractures.” Torus fractures rarely cause
physeal injury, but they may result in acute angular deformity. Because
P.473
torus
fractures are impacted, they are stable and rarely require manipulative
reduction. If manipulated, they usually regain the original fracture
deformity as swelling subsides. -
Torsional injuries result in two distinct patterns of fracture, depending on the maturity of the physis.
-
In the very young child with a thick
periosteum, the diaphyseal bone fails before the physis, resulting in a
long spiral fracture. -
In the older child, similar torsional injury results in a physeal fracture.
-
-
Bending moments in the young child cause
“greenstick fractures” in which the bone is incompletely fractured,
resulting in a plastic deformity on the concave side of the fracture.
The fracture may need to be completed to obtain an adequate reduction. -
Bending moments can also result in
microscopic fractures that create plastic deformation of the bone with
no visible fracture lines on plain radiographs; permanent deformity can
result. -
In the older child, bending moments
result in transverse or short oblique fractures. Occasionally, a small
butterfly fragment may be seen; however, because pediatric bone fails
more easily in compression, there may only be a buckle of the cortex.
CLINICAL EVALUATION
-
Pediatric trauma patients should undergo
full trauma evaluation with attention to airway, breathing,
circulation, disability, and exposure. This should ideally be performed
under the direction of a general surgical trauma team or pediatric
emergency specialist (see Chapter 2). -
Children are not good historians;
therefore, keen diagnostic skills may be required for even the simplest
problems. Parents may not be present at the time of injury and cannot
always provide an accurate history. It is important to evaluate the
entire extremity, because young children cannot always localize the
site of injury. -
As a general rule, children will tolerate
more pain and hardship than adults, especially if they understand what
you are about to do and trust you. It is therefore important to explain
everything to children, listen to their suggestions whenever possible,
and stop when they ask you to do so. -
Neurovascular evaluation is mandatory, both before and after manipulation.
-
Periodic evaluation for compartment
syndrome should be performed, particularly in a nonverbal patient who
is irritable and who has a crush-type mechanism of injury. A high index
of suspicion should be followed by compartment pressure monitoring. -
Intracompartmental blood loss from long bone fractures of the lower extremities can be a serious problem for the young child.
-
Child abuse must be suspected in the following scenarios:
-
Transverse femur fracture in a child <1 year old or a transverse humerus fracture in a child <3 years old.
-
Metaphyseal corner fractures (caused by a traction/rotation mechanism).
-
A history (mechanism of injury) that is inconsistent with the fracture pattern.
-
An unwitnessed injury that results in fracture.
-
Multiple fractures in various stages of healing.
-
Skin stigmata suggestive of abuse: multiple bruises in various stages of resolution, cigarette burns, etc.
P.474 -
-
It is the obligation of the physician to
ensure that the child is in a safe environment. If there is any
question of abuse, the child should be admitted to the hospital and
social services notified.
RADIOGRAPHIC EVALUATION
-
Radiographs should include appropriate
orthogonal views of the involved bone as well as the joint proximal and
distal to the suspected area of injury. Should there be uncertainty as
to the location of a suspected injury, the entire extremity may be
placed on the radiographic plate. -
A thorough understanding of normal ossification patterns is necessary to adequately evaluate plain radiographs.
-
Comparison views of the opposite
extremity may aid in appreciating subtle deformities or in localizing a
minimally displaced fracture. -
“Soft signs” such as the posterior fat pad sign in the elbow should be closely evaluated.
-
A skeletal survey may be helpful in searching for other fractures in cases of suspected child abuse or multiple trauma.
-
Computed tomography may be useful in evaluating complicated intraarticular fractures in the older child.
-
Magnetic resonance imaging can be
valuable in the preoperative evaluation of a complicated fracture; it
may also help evaluate a fracture not clearly identifiable on plain
films. -
Arthrograms are valuable in the
intraoperative assessment of intraarticular fractures because
radiolucent cartilaginous structures will not be apparent on
fluoroscopic or plain radiographic evaluation. -
Bone scans may be used in the evaluation of osteomyelitis or tumor.
-
Ultrasound can be useful for identifying epiphyseal separation in infants.
CLASSIFICATION
Salter-Harris/Ogden Classification (Fig. 42.2)
Pediatric physeal fractures have traditionally been
described by the five-part Salter-Harris classification. The Ogden
classification has extended the Salter-Harris classification to include
periphyseal fractures, which do not radiographically appear to involve
the physis but may interfere with the physeal blood supply and result
in growth disturbance.
described by the five-part Salter-Harris classification. The Ogden
classification has extended the Salter-Harris classification to include
periphyseal fractures, which do not radiographically appear to involve
the physis but may interfere with the physeal blood supply and result
in growth disturbance.
Salter-Harris Types I to V
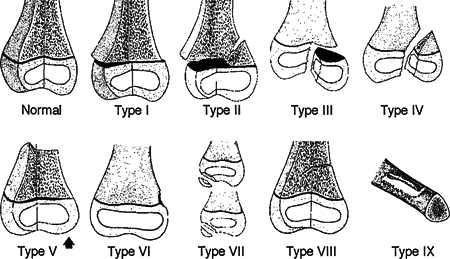
| Type I: | Transphyseal fracture involving the hypertrophic and calcified zones. Prognosis is usually excellent because of the preservation of the reserve and proliferative zones, although complete or partial growth arrest may occur in displaced fractures. |
| Type II: | Transphyseal fracture that exits through the metaphysis. The metaphyseal fragment is known as the Thurston-Holland fragment. The periosteal hinge is intact on the side with the metaphyseal fragment. Prognosis is excellent, although complete or partial growth arrest may occur in displaced fractures. |
| Type III: | Transphyseal fracture that exits the epiphysis, causing intraarticular disruption as well as disrupting the reserve and proliferative zones. Anatomic reduction and fixation without violating the physis are essential. Prognosis is guarded, because partial growth arrest and resultant angular deformity are common problems. |
| Type IV: | Fracture that traverses the epiphysis and the physis, exiting the metaphysis and disrupting all four zones of the physis. Anatomic reduction and fixation without violating the physis are essential. Prognosis is guarded, because partial growth arrest and resultant angular deformity are common. |
| Type V: | Crush injury to the physis. Diagnosis is generally made retrospectively. Prognosis is poor, because growth arrest and partial physeal closure are common. |
P.475
Ogden Types VI to IX
 |
|
Figure 42.2. Salter-Harris (Types I to V) and Ogden (Types VI to IX) classification of physeal injuries in children.
(From Ogden JA. Pocket Guide to Pediatric Fractures. Baltimore: Williams & Wilkins, 1987:25×2013;42.)
|
| Type VI: | Injury to the perichondral ring at the periphery of the physis. Usually, this is the result of an open injury. Close follow-up may allow early identification of a peripheral physeal bar that is amenable to excision. Prognosis is guarded, because peripheral physeal bridges are common. |
| Type VII: | Fracture involving the epiphysis only. This includes osteochondral fractures and epiphyseal avulsions. Prognosis is variable and depends on the location of the fracture and the amount of displacement. |
| Type VIII: | Metaphyseal fracture. Primary circulation to the remodeling region of the cartilage cell columns is disrupted. Hypervascularity may cause angular overgrowth. |
| Type IX: | Diaphyseal fracture. The mechanism for appositional growth (the periosteum) is interrupted. Prognosis is generally good if reduction is maintained. Cross union between the tibia and fibula and between the radius and ulna may occur if there is intermingling of the respective periosteums. |
P.476
TREATMENT
-
Fracture management in the child differs
from that in an adult owing to the presence of a thick periosteum in
the case of a diaphyseal fracture or open physis in metaphyseal
fractures.-
The tough periosteum can be an aid to
reduction because the periosteum on the concave side of the deformity
is usually intact and can be made to serve as a hinge, preventing
overreduction. Longitudinal traction will not reliably unlock the
fragments when the periosteum is intact. Controlled recreation and
exaggeration of the fracture deformity are effective means of
disengaging the fragments to obtain reduction. -
A periosteal flap entrapped in the
fracture site or buttonholing of a sharp fracture end through the
periosteum can prevent an adequate reduction. -
Remanipulation of physeal injuries should not be attempted after 5 to 7 days.
-
-
Unlike in the adult, considerable
fracture deformity may be permitted, because the remodeling potential
of the young child is great.-
In general, the closer the fracture is to
the joint (physis), the better the deformity is tolerated (e.g., 45 to
60 degrees of angulation in a proximal humeral fracture in a young
child is permissible, whereas the midshaft fracture of the radius or
tibia should be brought to within 10 degrees of normal alignment.). -
Rotational deformity does not
spontaneously correct or remodel to an acceptable extent even in the
young child and should be avoided.
-
-
Severely comminuted or shortened
fractures may require skin or skeletal traction. Traction pins should
be placed proximal to the nearest distal physis (e.g., distal femur).
Care should be taken not to place the traction pin through the physis. -
Fracture reduction should be performed
under conscious sedation, followed by immobilization in either a splint
or bivalved cast. Univalving, particularly with a fiberglass cast, does
not provide adequate cast flexibility to accommodate extremity swelling. -
In children, casts or splints should
encompass the joint proximal and distal to the site of injury, because
postimmobilization stiffness is not a common problem for children. Only
in rare fractures should short arm or short leg casts be applied (e.g.,
stable torus fractures of the distal radius).P.477-
As soon as 2 days after cast application, children will run on short leg casts or climb monkey bars in short arm casts.
-
-
All fractures should be elevated at heart
level, iced, and frequently monitored by responsible individuals, with
attention to extremity warmth, color, capillary refill, and sensation.
Patients in whom pronounced swelling is an issue or for whom the
reliability of the guardian is in question should be admitted to the
hospital for observation. -
Fractures in which a reduction cannot be
achieved or maintained should be splinted and the child prepared for
general anesthesia, with which complete relaxation may be achieved. -
Intraarticular fractures, Salter-Harris
types III and IV, require anatomic reduction (<1 to 2 mm of
displacement both vertically and horizontally) to restore articular
congruity and to minimize physeal bar formation. -
Indications for open reduction include:
-
Open fractures.
-
Displaced intraarticular fractures (Salter-Harris types III and IV).
-
Fractures with vascular injury.
-
Fractures with an associated compartment syndrome.
-
Unstable fractures that require abnormal positioning to maintain closed reduction.
-
COMPLICATIONS
Complications unique to pediatric fractures include the following:
-
Complete growth arrest: This may occur
with physeal injuries in Salter-Harris fractures. It may result in limb
length inequalities necessitating the use of orthotics, prosthetics, or
operative procedures including epiphysiodesis or limb lengthening. -
Progressive angular or rotational
deformities: They may result from physeal injuries with partial growth
arrest or malunion. If these result in significant functional
disabilities or cosmetic deformity, they may require operative
intervention, such as osteotomy, for correction. -
Osteonecrosis: May result from disruption
of tenuous vascular supply in skeletally immature patients in whom
vascular development is not complete (e.g., osteonecrosis of the
femoral head in cases of slipped capital femoral epiphysis).