
Editors: Frassica, Frank J.; Sponseller, Paul D.; Wilckens, John H.
Title: 5-Minute Orthopaedic Consult, 2nd Edition
Copyright ©2007 Lippincott Williams & Wilkins
> Table of Contents > Neurofibromatosis
Neurofibromatosis
Paul D. Sponseller MD
Description
-
Most common single gene disorder in humans
-
The disease involves multiple organ
systems; the skeletal and nervous systems account for the greatest
number of clinical features. -
The most common form is NF1 (addressed here); NF2 refers to bilateral acoustic neuromas.
-
The manifestations of NF1 may not develop until late childhood.
-
Some signs may be present at birth, but
neurofibromas may take years to become apparent, and diagnosis usually
is made in later childhood.
-
-
Synonym: von Recklinghausen disease
Epidemiology
Incidence
-
~1 in 3,000 newborns (1,2)
-
Males and females are affected equally.
Risk Factors
Advanced paternal age has been associated with an increased incidence of NF.
Genetics
-
Inherited in an autosomal-dominant pattern
-
Presents in ~1/2 of the patients as new mutations
-
Thought to occur with complete penetrance
Etiology
-
Genetic disorder
-
Secondary to a defect in the protein neurofibromin
Associated Conditions
-
Nearly 50% of people have cognitive delays ranging from severe retardation to slight learning disabilities (2).
-
A few patients develop metabolic bone disease that results in a type of osteomalacia.
-
Hypertension on the basis of renal artery stenosis or pheochromocytoma may be found.
Signs and Symptoms
-
To establish the diagnosis, 2 of the following National Institutes of Health diagnostic criteria must be met (Fig. 1):
-
6 café-au-lait spots measuring ≥5 mm in children and ≥15 mm in adults
-
1 optic glioma
-
≥2 Lisch nodules on the iris
-
1 osseous lesion typically seen in NF,
including vertebral scalloping, dystrophic scoliosis, rib penciling, or
pseudarthrosis of a long bone -
A 1st-degree relative with the disease
-
Axillary or inguinal freckling
-
Cutaneous or plexiform neurofibromas
-
-
Symptoms vary, depending on the criteria:
-
Plexiform neurofibromas often are associated with pain and neurologic deficit in the distribution of the particular nerve.
-
Cutaneous neurofibromas usually cause few symptoms.
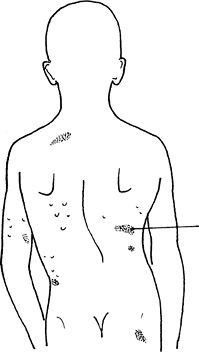 Fig. 1. This patient displays multiple café-au-lait spots, subcutaneous neurofibromas, and scoliosis characteristic of NF.
Fig. 1. This patient displays multiple café-au-lait spots, subcutaneous neurofibromas, and scoliosis characteristic of NF.
-
Physical Exam
-
Examine the neck and spine for deformity.
-
Inspect all the skin, including the axillae.
-
Ophthalmologic referral should be made so that the eyes can be examined with a slit lamp for Lisch nodules and optic glioma.
-
Limb lengths should be measured and checked for angulation (Fig. 2).
Tests
Lab
No laboratory tests reveal abnormalities specific for NF.
Imaging
-
The skeletal manifestations usually can be identified on plain radiographs:
-
May show posterior vertebral body scalloping
-
The dystrophic type of scoliosis is
characterized by penciling of the ribs, severe apical rotation, short,
segmented curves, and malformed vertebrae (3,4) (Figs. 3 and 4). -
The features of the pseudarthrosis that
can occur in long bones can range from a cystic appearance to severely
thinned and pointed pseudarthrosis, which fractures at birth. -
Sclerosis and constriction also can be found at the pseudarthrosis site.
-
Dural ectasia and pseudomeningocele also can affect the spine.
![]() Fig. 2. Distal anterolateral bow associated with NF1.
Fig. 2. Distal anterolateral bow associated with NF1.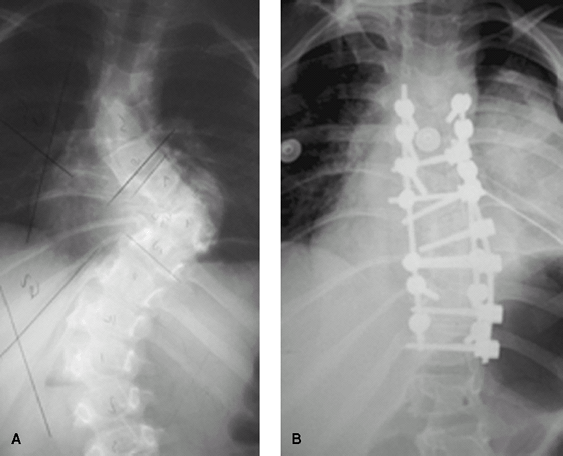 Fig. 3. Dystrophic scoliosis with NF1. A: Dystrophic scoliosis has short, sharp curves with penciling of the ribs. B: After surgical correction.
Fig. 3. Dystrophic scoliosis with NF1. A: Dystrophic scoliosis has short, sharp curves with penciling of the ribs. B: After surgical correction.
-
-
When instrumentation is planned to
correct a spinal deformity, MRI should be obtained to evaluate the
spinal canal for these changes. -
CT scanning may be helpful in assessing the laminae and pedicles for fixation.
-
Characteristic long-bone lesions can
include anything from benign scalloping of cortices to permeative
lesions that resemble malignant disease radiographically.![]() Fig. 4. Dystrophic cervical changes. A: Dystrophic change in NF1 may involve the neck. B: After surgery.
Fig. 4. Dystrophic cervical changes. A: Dystrophic change in NF1 may involve the neck. B: After surgery.

P.273

Pathological Findings
-
The disorder is 1 of cells of neural
crest origin: The cells of the embryonic neural crest are destined to
form tissue in many different organ systems, accounting for the diverse
manifestations of the disease. -
Lisch nodules of the iris are hamartomatous deposits.
-
The bone in pseudarthrosis typically is fibrotic, with few osteoblasts.
-
Cutaneous neurofibromas are composed of Schwann cells and connective tissue.
Differential Diagnosis
-
Proteus syndrome most closely resembles NF in its manifestations.
-
Patients with isolated congenital
pseudarthrosis of the tibia must be monitored for NF because the
café-au-lait spots may develop later NF. -
NF2 consists of only bilateral acoustic neuromas.
General Measures
-
Patients should be seen regularly by a
geneticist or primary physician to rule out developmental delay, growth
disturbance, scoliosis, or neurologic deterioration. -
Patients usually are functional, except those who are severely mentally handicapped.
-
No specific dietary requirements exist.
Activity
-
Bracing for prepseudarthrosis of the tibia, especially during activities, is recommended.
-
Otherwise, activity should not be restricted unnecessarily.
Medication
Although speculative, angiogenesis inhibitors may be
used to decrease the vascularity of plexiform neurofibromas and allow
easier surgical removal.
used to decrease the vascularity of plexiform neurofibromas and allow
easier surgical removal.
P.274
Surgery
-
Dystrophic scoliosis should be treated surgically if any evidence of progression is seen.
-
Anterior and posterior fusions usually
are recommended if focal kyphosis or a curve >50–60° is present in a
skeletally immature patient. -
When diagnosed, patients with dystrophic
tibial changes should be braced, and the bracing should be continued
until skeletal maturity. -
If fracture occurs, use intramedullary
nails (with bone grafting or vascularized fibula bone grafting) or
compression and distraction (Ilizarov) treatment with ring fixators.-
All treatment should be protected after union occurs until the end of growth.
-
-
Plexiform neurofibromas should not be
treated surgically because total removal is nearly impossible and
neurologic deficits typically occur. -
Leg-length inequality should be charted
and followed with serial scanograms to ascertain the timing of
contralateral leg epiphysiodesis or limb lengthening.
Prognosis
Life expectancy may be compromised by severe mental retardation and malignant disease.
Complications
-
Patients with NF1 have a high incidence of malignancy.
-
Usually, these tumors are of the central nervous system.
-
Plexiform neurofibromas also can degenerate into neurofibrosarcomas.
-
Amputation of a leg may be necessary in a
patient with severe pseudarthrosis because correction of the nonunion
is not always successful. -
In rare instances, the function of the patient may be best served with amputation.
-
Some patients with dystrophic scoliosis have malformed vertebrae.
-
If substantial kyphosis exists, correction can cause neurologic compromise.
-
Spinal cord monitoring should be performed during all spinal procedures.
Patient Monitoring
-
Annual scanograms are indicated for limb-length discrepancy.
-
Physical examinations for detection of scoliosis should be performed on a yearly basis while the child is growing.
-
Hypertension is a common finding in patients with NF and should be monitored regularly.
References
1. Akbarnia BA, Gabriel KR, Beckman E, et al. Prevalence of scoliosis in neurofibromatosis. Spine 1992;17:S244–S248.
2. Alman
BA, Goldberg MJ. Syndromes of orthopaedic importance. In: Morrissy RT,
Weinstein SL, eds. Lovell and Winter’s Pediatric Orthopaedics, 6th ed.
Philadelphia: Lippincott Williams & Wilkins, 2006:251–313.
BA, Goldberg MJ. Syndromes of orthopaedic importance. In: Morrissy RT,
Weinstein SL, eds. Lovell and Winter’s Pediatric Orthopaedics, 6th ed.
Philadelphia: Lippincott Williams & Wilkins, 2006:251–313.
3. Crawford AH, Jr, Bagamery N. Osseous manifestations of neurofibromatosis in childhood. J Pediatr Orthop 1986;6:72–88.
4. Vitale MG, Guha A, Skaggs DL. Orthopaedic manifestations of neurofibromatosis in children: an update. Clin Orthop Relat Res 2002;401:107–118.
P.275
Codes
ICD9-CM
237.7 Neurofibromatosis
Patient Teaching
-
The incidence of tumors (especially those
of the nervous system), including optic gliomas, astrocytomas, and
acoustic neuromas, is increased.-
Education about the early signs of auditory, visual, or motor disturbances should be discussed with patients.
-
-
Educate the patient regarding the need to protect against pseudarthrosis of the tibia until skeletal maturity.
-
Discuss the potential for limb-length discrepancy when pseudarthrosis of the lower extremity or limb gigantism is present.
-
Typical discrepancy in both disorders rarely exceeds 6 cm.
-
-
If possible, bracing of pseudarthrosis in the tibia should be attempted.
-
Bracing for dystrophic scoliosis is not effective.
-
Bracing for the more commonly encountered
idiopathic type of scoliosis should be instituted when the regular
indications for idiopathic scoliosis are met.
FAQ
Q: Should soft-tissue neurofibromas be removed?
A: Only if they are growing excessively or are causing symptoms.